
Abstract
Introduction
This study evaluated the role of high-resolution ultrasonography in the assessment of pigmented skin lesions in correlation with clinico-pathological findings to predict malignant potential with high sensitivity and specificity.
Methods
A prospective cross-sectional study was carried out in 124 cases of pigmented skin lesions by using variable frequency (6–18 MHz) high-resolution ultrasonography and colour Doppler over a period of 14 months in Central Hospital, South Central Railway, Hyderabad, India. The correlation between sonographic parameters (greyscale imaging characteristics and vascular flow on colour Doppler) and pathological parameters (malignant and benign) were statistically analysed.
Results
For predicting malignancy, the presence of vascular flow on colour Doppler had good overall accuracy, specificity and negative predictive value but relatively low sensitivity and positive predictive value (respectively, 91%, 94%, 94%, 81% and 78%). However, greyscale imaging characteristics to predict malignancy had low overall accuracy, specificity and positive predictive value but high sensitivity and negative predictive value (respectively, 54%, 34%, 26%, 85% and 89%). There was a significant positive association between vascular flow on Doppler and malignancy (P = 0.0001) but the correlation between greyscale imaging findings and malignancy is not statistically significant (P = 0.0603).
Conclusions
High-resolution sonographic imaging is useful in non-invasive monitoring of pigmented lesions at risk and screening of pigmented lesions suspected of malignancy to give relevant information about the extent and nature of the disease and to stratify the high risk cases for surveillance and planning of the treatment.
Introduction
The non-invasive techniques at present for in vivo imaging of skin are confocal microscopy, optical coherence tomography, high-resolution ultrasonography (HRUS) and cutaneous magnetic resonance imaging (MRI). Confocal microscopy does not explore beyond 200 μm, solely allowing the study of the epidermis and lesions which affect it while optical coherence tomography does not allow in-depth exploration beyond the papillary dermis and the use of these techniques is still restricted. 1 Recently, 3 Tesla magnetic resonance imaging of skin was described by Aubry et al. 1 which allowed high spatial resolution imaging of the skin, particularly for the epidermis and the hypodermis. But its utility is limited as it requires high field strength magnets, dedicated coils, long acquisition times and is prone to multiple artefacts. It is also expensive, not easily accessible and cannot be performed on patients with contraindications to MRI examination.
High variable-frequency ultrasound is a recently available technique capable of clearly defining skin layers and deeper structures that also provide local perfusion patterns obtained in real time. 2 The transducers used in high variable frequency ultrasonography are able to focus on different tissue layers by modifying the applied frequency according to depth of tissue imaged. This enables visualization of the skin layers, underlying musculo-tendinous, cartilaginous and bony structures along with vasculature and perfusion patterns at the same resolution. Application of ultrasonic techniques provides non-invasive investigation within a lesion and the possibility of analyzing certain aspects of the skin that are inaccessible to the eye of the dermatologist and even to histological examination. 3 For diagnostic purposes, ultrasound examination makes it possible to recognize lesions causing morphological changes in the structure of the skin, to localize lesions and their extent, and to measure their thickness and density. It is expected to determine the size, contour, structure and penetration depth of skin tumours at an early stage. 3
High frequency cutaneous ultrasonography has an important contribution in the screening of pigmentary lesions at risk. The findings based on ultrasound examinations are, as far as their precision is concerned, ranked between the findings obtained by clinical examinations, and those based on pathohistological methods. 4 The inclusion of this method among the procedures used for the diagnosis of skin diseases is an attempt to replace, as far as possible, the invasive procedures, especially biopsy, with non-invasive ones. 5 In this study we aim to compare and correlate the results of HRUS and colour Doppler with clinical diagnosis and histopathologic analysis to establish its usefulness in the diagnosis and management of pigmented lesions of the skin.
Materials and methods
Subjects
The study was conducted over a period of 14 months between January 2011 and February 2012 in 124 cases of clinically evaluated pigmented lesions of skin in Central Hospital, South Central Railway, a tertiary care government hospital. The study was approved by the ethics committee of the institution (approval number MD/CH/138/RD), and informed consent was obtained from all patients. All the patients underwent detailed clinical examination followed by HRUS and histopathological analysis. The study team examining and reviewing all the cases included dermatologist, radiologist and pathologist with more than 10 years of experience in their respective fields. The inclusion criteria were (1) pigmented lesions without any previous treatment or biopsy, (2) patients with both single or multiple lesions. The exclusion criteria included (1) pregnant women, (2) previously resected or biopsied lesions, (3) patients under follow-up for residual disease or recurrence, (4) patients having diffuse pigmentation over large surface areas and (5) patients unwilling for biopsy.
Procedure
The study was performed using My-Lab™ 60 (Esaote, Genoa, Italy) US scanner having linear array high-frequency transducers with an operating bandwidth of 6–18 MHz and depth of 0–90 mm within the focal area of the transducer. The scanner's settings (overall gain, time gain compensation, Doppler gain, power output) were standardized. Colour Doppler imaging was performed by using lower frequencies, increasing the pulse repetition frequency and shifting the baseline according to the depth scanned to prevent aliasing. A copious amount of gel was used over the surface of the lesions and any hair present was displaced with gel towards the lesion margins to minimize artefacts. Compression was avoided in superficial lesions because this may have resulted in a false thinning of the lesions. The mirror image or contralateral unaffected skin was used as a control for skin thickness in inflammatory skin diseases.
The lesions were classified according to the sonographic appearance, into ‘focal’ and ‘diffuse’ patterns. A lesion seen as a hypoechoic or mixed echo oval solid form with relatively definable margins was considered as focal. An isoechoic or hyperechoic ill-defined area with poorly defined margins, with or without an increase of thickness of the dermis and/or the subcutaneous layers, was considered as diffuse.
The ultrasound report consisted of: (a) morphologic study of the lesion including the shape (linear, oval, irregular), echogenicity (hypoechoic/isoechoic/hyperechoic), internal echotexture (homogeneous/heterogeneous), extent (focal/diffuse), margins (well defined/ill defined) and level of invasion (involvement of underlying structures); (b) measurements of the lesion. These included the largest diameter in both longitudinal and transverse views and thickness measured from the entry echo to the deepest infiltration point of the lesion. Colour and power sonography was used in detecting the intralesional and perilesional flow signals to suggest the presence of vascularity. In the arterial vessels of lesions where spectral analysis could be acquired, colour Doppler was used to visualize abnormal intra- or peritumoural vessels with low-resistance pulsatile flow characteristic of the vascular pattern of malignant cutaneous lesions.
All the patients underwent complete surgical excision or partial biopsy of the lesions and the tissue was histologically analysed. The findings of ultrasound and colour Doppler were correlated with clinical features and histopathological analysis of the corresponding sections of the biopsied lesion.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics 17. The imaging characteristics of the lesions that were compared are echogenicity, extent, margins, internal echotexture and presence of vascularity, and the histopathological characteristics compared were malignant and benign nature of lesions. The study compared the sonographic and pathological parameters by two-way contingency table analysis which gave the Yates-corrected chi-square and Pearson's correlation coefficient. P value was obtained from two-tailed Fisher Exact Test. Analysis of the effectiveness of a diagnostic criterion was done obtaining sensitivity, specificity, positive and negative predictive values, positive and negative likelihood ratios, diagnostic and error odds ratios.
Results
Of the 124 patients recruited for this study, 43 were women and 81 were men, with an age range from 15 to 87 years (median 53 years). The average age of patients with malignancy was 63 years (SD 9.3) and 70% of malignant lesions were seen in men.
Data of cases examined on high-resolution ultrasonography and colour Doppler
Lesion location on high-frequency ultrasonography
Colour Doppler and power Doppler sonography has shown arterial vessels extending from the periphery of the tumour to the centre of the lesions in 77% (22/27) of the malignancies. Only 6% (6/97) of benign lesions revealed vascularity on Doppler examination.
Predictive values of high-frequency ultrasonography and Doppler characteristics for malignancy
Greyscale imaging characteristics compared-echogenicity, extent and margins, internal echotexture. PPV, positive predictive value; NPV, negative predictive value, figures indicated in percentage
Discussion
Dermatological ultrasonography was initiated in the 1970s by Harold and Miller, who used high-frequency ultrasound waves of 15 MHz. 6 Ultrasonography with variable frequency transducers from 5 to 20 MHz range can be used for combined evaluation of skin, subcutaneous tissues and deeper layers. In our study we have used variable frequency transducer of 6–18 MHz range to evaluate the lesions.
Ultrasonography of normal tissue at 18 MHz shows a well-defined hyperechoic band known as ‘entry echo’ at the interface between the transducer and the skin. It is produced by the difference in the acoustic impedance between gel and skin. Underneath, the dermis is seen as a hyperechoic layer. The subcutaneous tissue is seen as hypoechoic layer with diffuse hyperechoic connective tissue septa separating the adipose lobules. More deeply, the superficial fascia covering the muscular tissues can be seen as a hyperechoic regular line (Figure 1).
Normal skin: High frequency ultrasonography (at 18 MHz) showing the three distinctive layers of entry echo, dermis and subcutaneous tissue
High-frequency sonography shows both benign and malignant focal lesions as hypoechoic structures with respect to healthy skin. High-frequency sonography renders important preoperative information about the tumour size and especially about the tumour thickness in different skin tumours including cutaneous melanoma, basal cell carcinoma and squamous cell carcinoma. These tumours are visualized mainly as hypoechoic structures within the hyperechoic dermis. 7 The biological nature of a tumour may affect the extent to which high-frequency sound waves are transmitted through it as significant differences were noted in the attenuating characteristics between pigmented lesions. 8 Heterogeneity in internal echo images seemed to be related to histopathological structures, including calcification, cornified cysts, clusters of parakeratotic cells, apoptotic cells or necrosis in the tumour cell nests. 9
The identification of abnormal intra- or peritumoural low-resistance pulsatile flow signals suggests the malignant nature of the cutaneous lesion. 6 In a study of colour Doppler sonography in focal lesions of the skin and subcutaneous tissue by Giovagnorio et al. 10 the sensitivity and specificity of hypervascularity in malignant lesions were 90% and 100%, respectively, whereas the sensitivity and specificity of hypervascularity in malignant lesions in our study were 81% and 93%, respectively.
In our study, seborrheic keratoses on ultrasound were seen just beneath the entry echo corresponding to the epidermal origin on histology and were hypoechoic and heterogeneous with irregular surface and borders. The majority of the lesions were avascular (95%) and 76% of the lesions revealed posterior acoustic shadowing (Figure 2). Harland et al.
11
reported that high attenuation, prominent entry echo and irregular surface were seen in seborrheic keratosis which differentiated it from melanomas and other benign naevi due to surface keratinization of these tumours, which makes them reflective and irregular with shadowing.
Seborrheic keratosis: 13 × 2.8 mm hypoechoic, heterogeneous superficial lesion at dermo-epidermal junction compressing the underlying dermis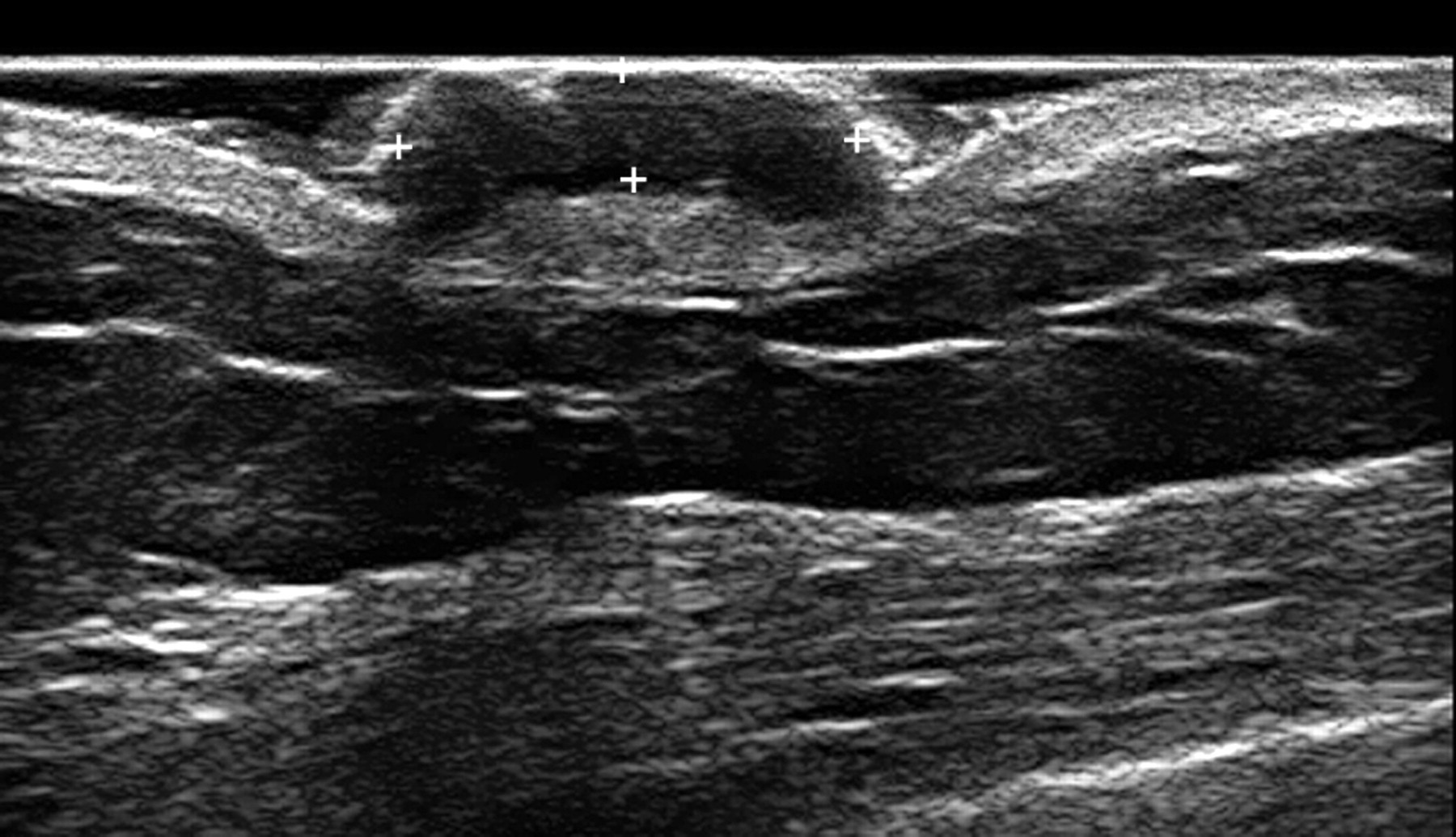
In our study, sonography revealed oval, hypoechoic, heterogeneous lesions in all the cases of basal cell carcinoma while hyperechoic spots, surface irregularity, posterior acoustic shadowing and vascularity were seen only in 83% of the cases (Figure 3). Uhara et al.
9
in their study suggested that hyperechoic spots corresponding to keratin nests on histological section might become a useful finding for differential diagnosis between basal cell carcinoma and melanoma as they were observed in three quarters of basal cell carcinoma lesions but not in any melanoma lesions.
Basal cell carcinoma: 24 × 6 mm hypoechoic lesion in the dermis with posterior shadowing and few intralesional vessels on colour Doppler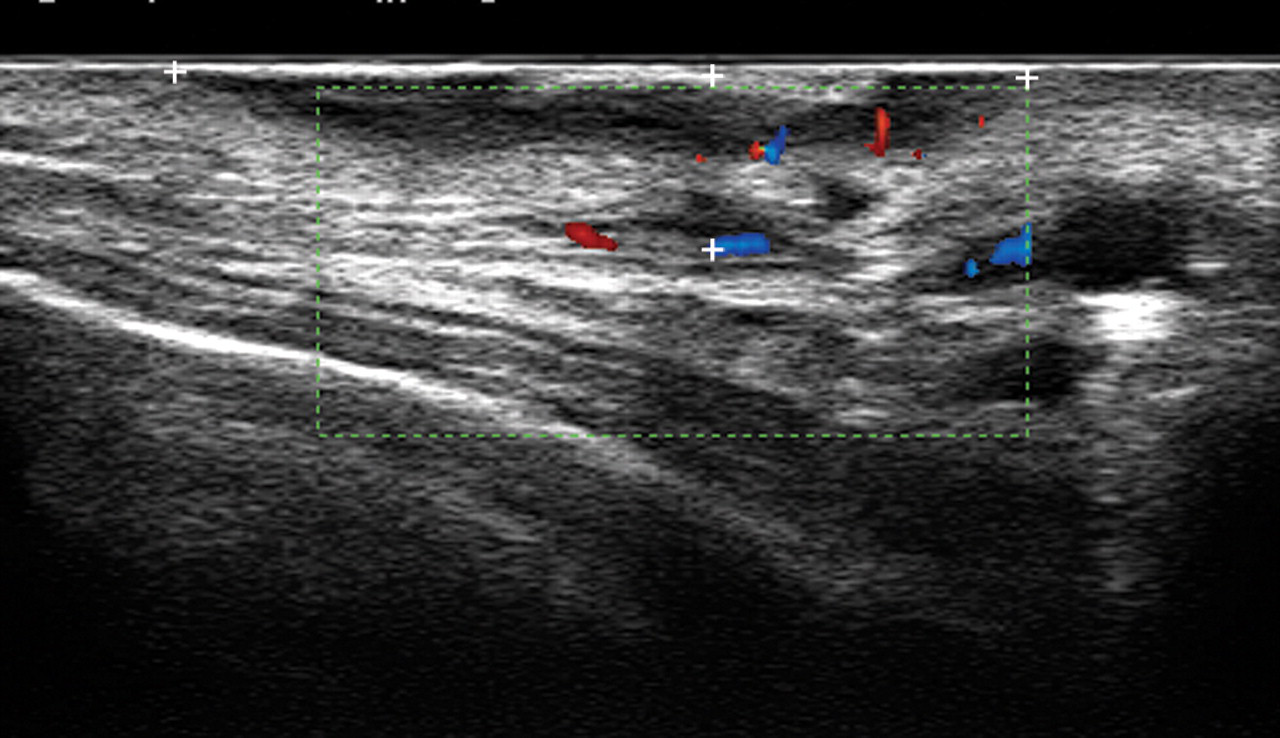
Malignant melanoma is a lethal but curable skin cancer and early detection is the basis for reducing the mortality rate with non-invasive skin imaging playing an important role in this regard. The tumour invasion depth according to Breslow
12
is the single most important prognostic factor in cutaneous malignant melanoma which can be measured accurately and noninvasively by using high-resolution ultrasound. Lassau et al.
13
in their study found that there was no difference between the sonographic patterns of melanomas and naevi as they were all hypoechoic with a homogeneous echostructure and well-defined lower and lateral margins. In our study malignant melanoma was hypoechoic, homogeneous and oval shaped with irregular borders and similar in imaging appearance to that of melanocytic naevi. Bessoud et al.
14
evaluated pigmented skin lesions with high-frequency sonography and showed that colour Doppler detection of intralesional vessels had a 100% specificity and 34% sensitivity in the distinction of melanomas from other pigmented skin lesions. Recognizing intralesional colour Doppler signal is helpful because it correlates with the Breslow's index and with patient survival. Flow signals are found in lesions thicker than 2 mm, particularly at their bases, and indicate a high-microvascular density.
15
Melanomas in our study revealed multiple intralesional vessels arising from the base of the lesion suggesting its highly vascular nature and this pattern of vascularity may be useful in differentiating malignant melanoma from benign naevi (Figure 4).
Malignant melanoma: 11 × 4 mm hypoechoic, homogeneous and oval lesion in the dermis. Colour Doppler shows a large vascular pedicle and diffuse perfusion of the lesion from multiple small vessels arising from the base of the lesion
Cutaneous lymphoma can present itself in a diffuse or a nodular form. Nodular lymphoma is seen as a hypoechoic solid nodule, with ill-defined margins; such a pattern is common to other diseases and therefore is not specific.
16
The primary cutaneous lymphomas in our study presented as multiple pigmented nodules on trunk and extremities. The lesions were seen in the dermis and the subcutaneous layer on sonography as multiple mixed echoic nodules with intralesional vessels. This appearance was similar to the type II pattern of cutaneous lymphomas described by Giovagnorio et al.
17
(Figure 5).
Primary cutaneous lymphoma: 16 × 4.8 mm mixed echoic coalescing nodules in the dermis and the subcutaneous layer with areas of perfusion on colour Doppler
Squamous cell carcinoma is a malignant tumour with a tendency to infiltrate the skin and adjacent tissue eroding the cartilage and bones with frequent lymph nodal metastases and local relapses. It is seen during sonography as a lesion with marginal irregularities, inhomogeneous hypoechoic structure and may show the presence of low-resistance pulsatile flow signals within or at the periphery of the tumour on Doppler.
16
The squamous cell carcinomas in our study were not as hypoechoic as other malignancies and were inhomogeneous in echotexture. Vascularity on Doppler was not seen in one case of squamous cell carcinoma and all the three cases of Bowen's disease which were included in this category (Figure 6).
Squamous cell carcinoma: Diffuse inhomogeneous, infiltrative lesion involving dermis, subcutaneous layer, underlying fascia and muscles with loss of normal architecture and multiple intralesional vessels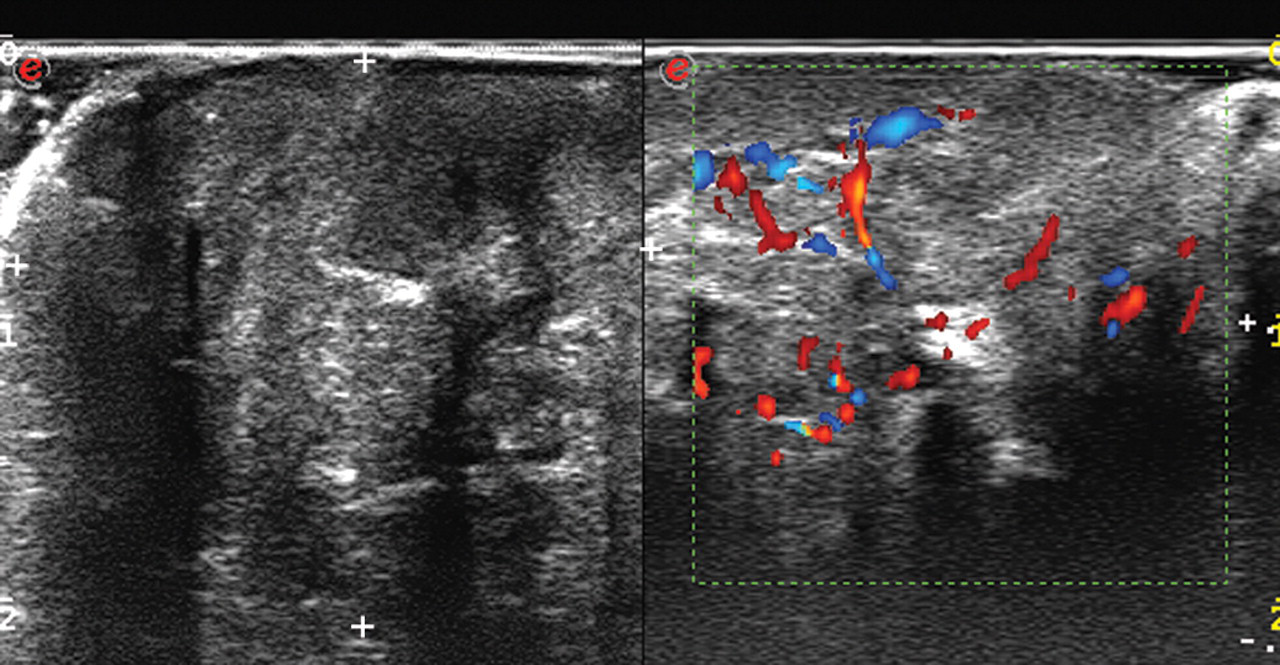
Cutaneous metastases in our study were seen clinically as pigmented nodules on the chest in post-treatment cases of carcinoma of the breast and lung and the lesions on sonography appeared as well-circumscribed, solid, hypoechoic, homogenous nodules in the skin and subcutaneous tissue.
Ultrasonography is the optimal method for the monitoring of congenital naevi which usually undergo malignant transformation during childhood. 5 Ultrasonography can identify the hypoechoic naevi penetrating the dermis during malignant transformation into melanomas.
In our study, naevi were seen as hypoechoic, homogeneous, linear or oval lesions with regular borders (Figure 7). Three superficial epidermal naevi could not be detected by sonography and on colour Doppler, vascularity was not seen in 89% of naevi.
Benign nevus: 7 × 1.3 mm hypoechoic, homogeneous oval lesion with well-defined borders embedded in the dermis
High-frequency sonography may also be used in the evaluation of diffusely pigmented cutaneous diseases and we have evaluated lesions of post inflammatory hyper pigmentation and contact dermatitis (both allergic and irritant). In the majority of these cases, no clear lesion was identified and the dermis was isoechoic to hyperechoic with increased thickness.
Scleroderma is sclerosis of the skin of unknown aetiology that can manifest itself as localized (morphea) or generalized forms. The lesions of morphea in our study were isoechoic to hyperechoic on sonography with diffusely increased thickness of dermis and subcutaneous tissue compared with the normal contra-lateral side (Figure 8). In comparison to the healthy skin, the ultrasound scan of sclerotic skin shows a wide entry echo and highly reflective, thicker dermis as a result of the collagen fibres accumulation.
16
Sonographic findings vary depending on disease activity and disease course and treatment efficacy can be monitored by high-resolution transducers in focal scleroderma.
6
Morphea: Diffusely increased thickness of dermis and subcutaneous tissue in the area of lesions compared to contralateral normal side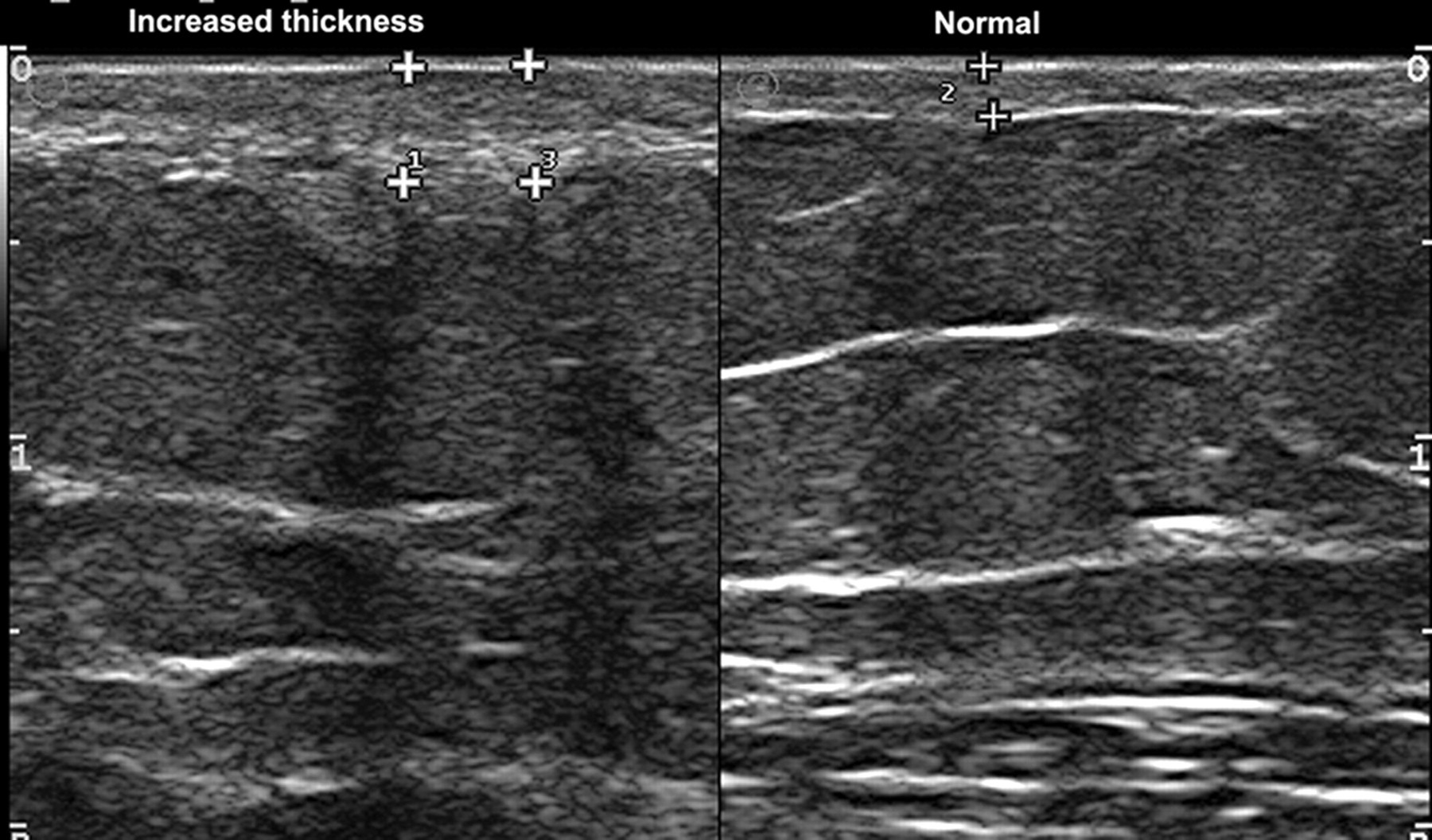
Limitations
The limitations of ultrasound are that, in its current version, it cannot detect lesions that are epidermal only or that measure less than 0.1 mm in depth, 2 overestimation of thickness compared to the actual histological tumour thickness in lesions with inflammatory peritumoural infiltration like melanomas and underestimation of thickness in ulcerated lesions. 7 The limitations in our study are that the thickness of lesions on ultrasound and histology were not compared and findings of ultrasound were made only once and by the same person hence intra-observer and inter-observer variability was not calculated.
Further study
Real time contrast-enhanced ultrasound is a recent technique under evaluation to provide quantitative perfusion parameters by using second generation ultrasound contrast agents to increase the sensitivity of Doppler examination. It is useful in morphologic and functional assessment of lesions providing quantitative perfusion parameters, which can be biomarkers for new antiangiogenic therapy monitoring. 18
In future, advances in sonography like tissue harmonic imaging, spatial compound imaging, panoramic views and three-dimensioal reconstruction techniques may increase resolution and image quality to provide specific and accurate diagnosis of individual lesions.
Conclusion
While realtime ultrasonography with colour Doppler cannot replace the histopathological examination, it may be performed after clinical examination to assess the morphological structure, extent and vascularity of both the visible and subclinical lesions, along with that of surrounding tissues. The primary advantage of ultrasonography and colour Doppler is that it is a simple, non-invasive modality providing realtime images of suspected pigmented lesions which can be repeated any number of times without much discomfort or adverse effect to the patient.
In conclusion, the findings on greyscale sonography combined with vascular flow signals on colour Doppler can be of great assistance in the assessment of pigmented lesions of skin to predict malignant potential with high sensitivity and specificity. It can also aid the clinician by giving relevant information about the extent and nature of the disease to stratify the high risk cases for surveillance and planning of the treatment. High resolution sonographic imaging can be useful as an alternative diagnostic modality in non-invasive monitoring of pigmented lesions at risk and screening of pigmented lesions suspected of malignancy as well as a guide to further histopathological examination to avoid indiscriminate biopsies and resections.
DECLARATIONS