
Abstract
Chorioangioma is the most common benign tumour of the placenta. Smaller lesions are asymptomatic but larger lesions are associated with adverse prognosis. Antenatal ultrasonography with colour Doppler is the primary modality in diagnosing these lesions and their complications. Chorioangiomas are generally associated with polyhydramnios but can rarely present with oligohydramnios. We report a case of a large chorioangioma, which led to oligohydramnios, compromised fetal blood flow and reduced fetal growth. A live infant weighing 830 g was delivered by Caesarean section at 34 weeks but survived for only two days.
Introduction
A chorioangioma is a benign tumour of the placenta, consisting of blood vessels and stroma, that proliferates beyond normally developing chorionic villi. Clinical manifestations are rare in this condition and are usually associated with tumours greater than 5 cm in diameter. The adverse prognosis of these pregnancies, especially with larger lesions, makes the use of antenatal ultrasonography and colour Doppler important to detect these lesions and manage complications.
Case report
A 29-year-old gravida 2, para 1 was referred for routine obstetric ultrasound examination. The examination was performed using a MyLab™ 60 (Esaote, Genoa, Italy) ultrasound unit with a 3.5–7.5 MHz curvilinear transducer and convex volume transducer for three dimensional (3D) and four dimensional (4D) examinations. The first ultrasound examination was unremarkable and showed a single intrauterine fetus of 13 weeks gestation and an anteriorly located placenta. A second ultrasound examination at 19 weeks of pregnancy revealed a circumscribed, ovoid, intraplacental mass measuring 52 × 42 mm protruding into the amniotic cavity (Figure 1). Colour Doppler imaging revealed a large feeding vessel supplying the mass from the umbilical artery (Figure 2). Duplex Doppler showed both umbilical arterial and venous flow within the mass (Figure 3). Three dimensional ultrasound revealed a well circumscribed placental lesion projecting into the amniotic cavity (Figure 4). At 24 weeks of pregnancy, the fetal growth corresponded to only 22 weeks on ultrasound and the four quadrant amniotic fluid index (AFI) measured only 5 compared with the normal range of 8–24. 1 Follow-up scans demonstrated intrauterine growth restriction (IUGR) in the fetus, with oligohydramnios and an increase in the size of the placental mass. At 28 weeks, the umbilical artery showed elevated Doppler indices with a pulsatility index (PI) of 2.09, resistivity index (RI) of 1.00 and SD ratio of 4.96.
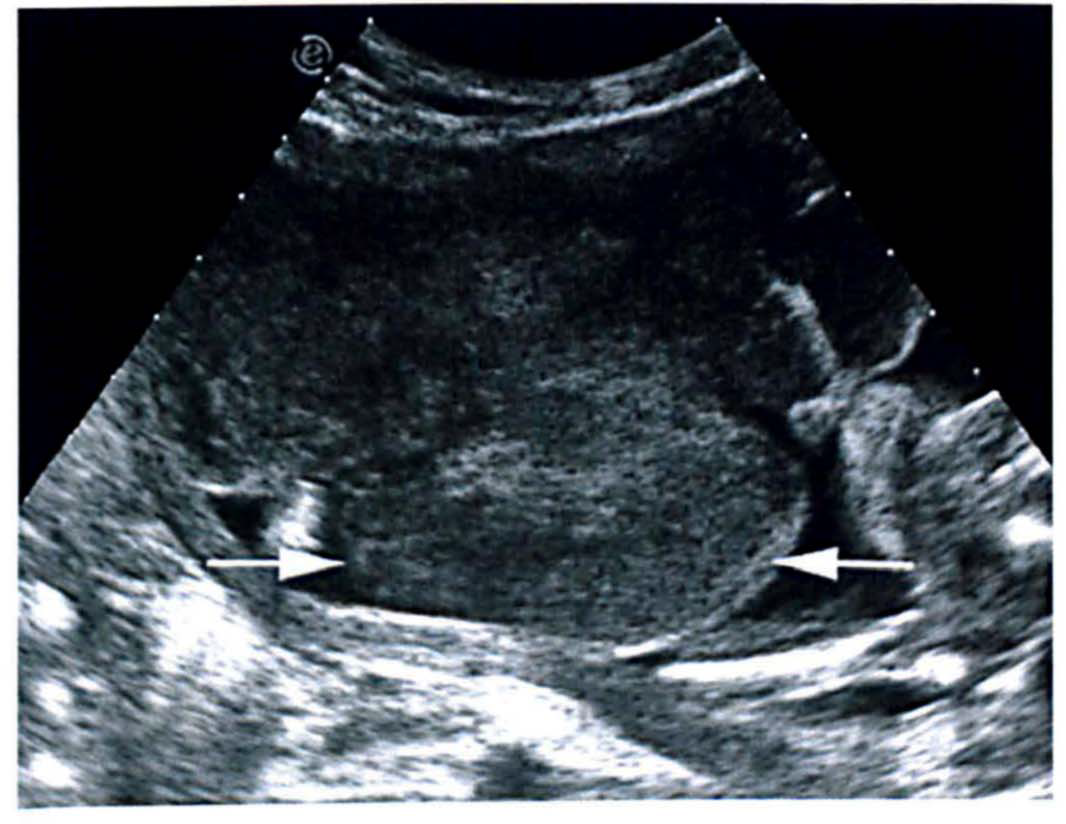
Grey-scale ultrasound shows a heterogeneous intraplacental mass (white arrows) protruding from the fetal surface of the placenta into the amniotic cavity
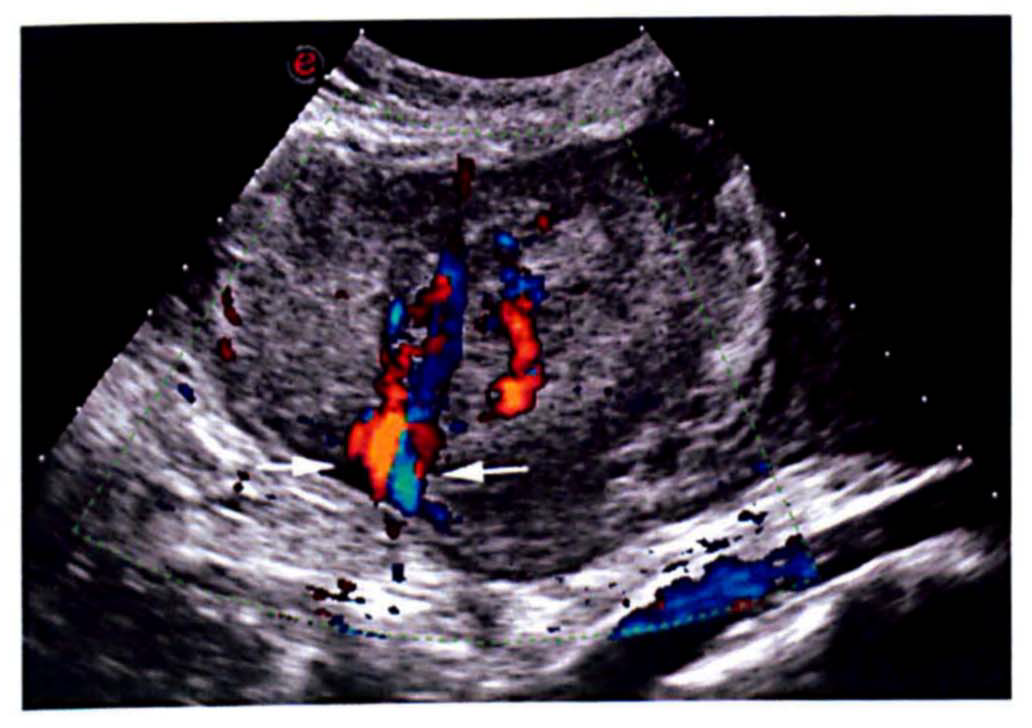
Colour Doppler imaging reveals a large feeding vessel supplying the mass from adjacent umbilical artery (white arrows)
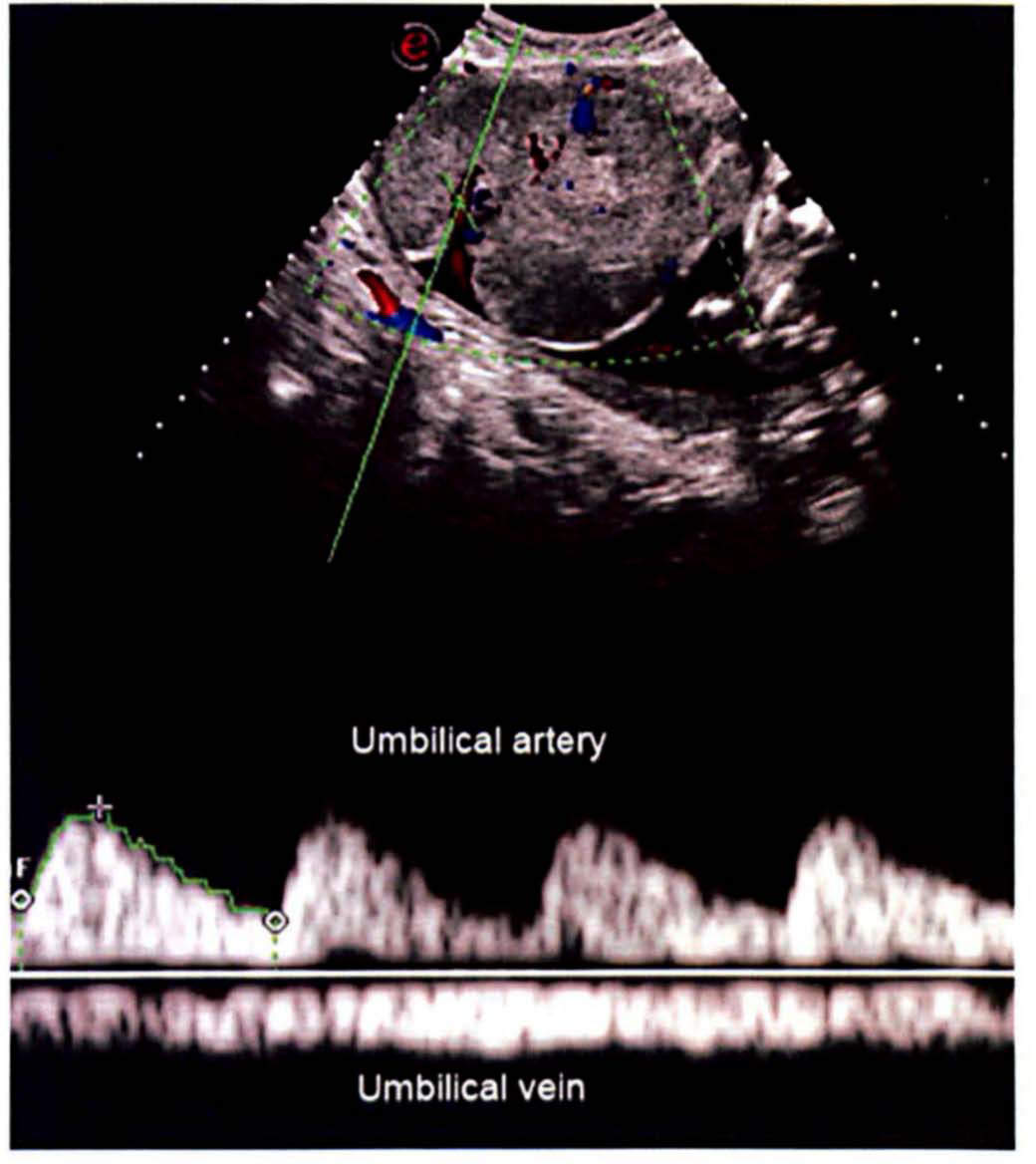
Duplex Doppler imaging reveals the spectral wave forms of both umbilical artery and umbilical vein supplying the placental mass
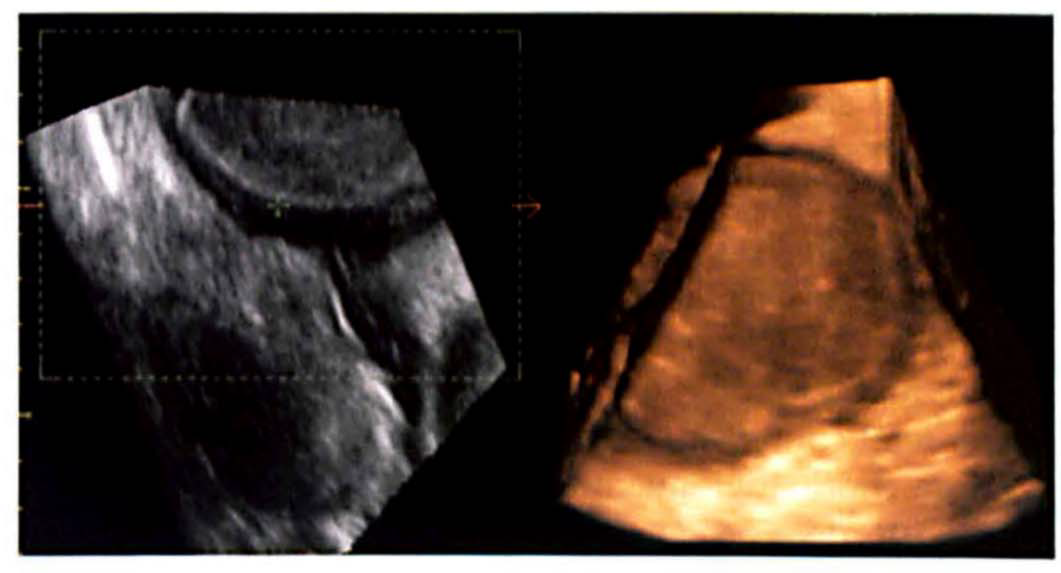
A three dimensional surface-rendered ultrasound image reveals a well circumscribed placental lesion projecting into the amniotic cavity
On ultrasound examination at 34 weeks, the fetus corresponded to only 26 weeks of gestation, the heterogeneous placental mass was approximately 10 × 12 cm, and there was severe oligohydramnios (AFI: 2). Duplex Doppler showed absent end diastolic flow in the umbilical artery. In view of the deteriorating fetal condition, a Caesarean section was performed and a live male infant weighing 830 g was delivered. Liquor was almost absent. The placenta was very thick and was removed without difficulty and sent for histological evaluation (Figure 5). The infant died after two days. The mother made an uneventful postoperative recovery.
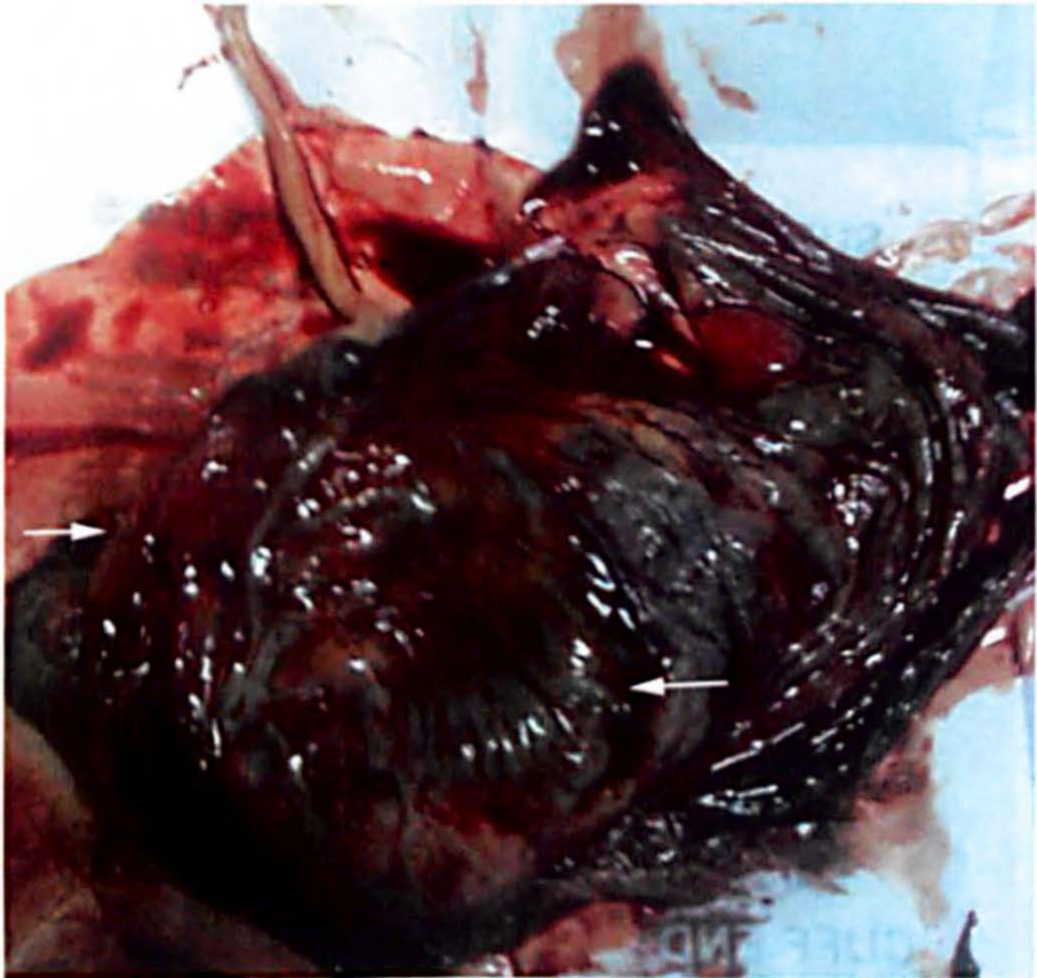
Gross specimen of the placenta, immediately after placental delivery, shows a large placental mass (white arrows) close to the umbilical cord
Histological analysis of the mass revealed multiple small, vascular spaces lined by endothelial cells within a collagenous stroma with hyalinization and fibrosis confirming the prenatal diagnosis of a placental chorioangioma.
Discussion
Chorioangioma, originally described by Clarke in 1798, is the most common tumour of the placenta, with a reported prevalence of approximately 0.5–1.0%. 2 Small tumours are usually asymptomatic but large tumours may be associated with arteriovenous shunting within the placenta leading to complications and increased perinatal mortality. 3 Larger lesions (>5 cm) can be associated with fetal morbidity (non-immune hydrops, IUGR, neonatal cardiomegaly, anaemia and thrombocytopenia) and mortality, as well as maternal morbidity such as polyhydramnios and preeclampsia. 4 The most common clinical complication associated with chorioangioma is polyhydramnios; however, oligohydramnios has also been reported. 5 The decrease in functional placental tissue causes placental insufficiency, which can lead to IUGR. 5 In our case, the patient developed both oligohydramnios and IUGR as the chorioangioma increased in size.
The first sonographic diagnosis of a placental chorioangioma was reported by Asokan et al. 6 in 1978. Usual grey scale findings include intraplacental subchorionic location, well-defined circumscription, complex echogenicity, which is different from the rest of the placenta, single or multiple tumours and protrusion into the amniotic cavity near the insertion of the umbilical cord. 7
Previous studies have demonstrated blood flow in all of these lesions by colour Doppler (either abundant blood flow or a single large feeding vessel) and differentiated chorioangiomas from placental haematomas by the existence of blood flow within the lesions.8, 9 Colour Doppler is also used to confirm that vascular channels in the tumour are contiguous with the fetal circulation as chorioangioma is a tumour supplied by the fetal circulation, thus ruling out other differential diagnoses such as a degenerated myoma, a placental teratoma and an incomplete hydatidiform mole. 9
Tumour size is the most important factor in influencing the prognosis of affected pregnancies. 3 The vascularity of the tumour may be an independent factor for fetal complications, regardless of the tumour size. 10 In avascular tumours, complications are not expected, but in vascular tumours containing numerous large vessels, serial ultrasound and Doppler examinations may be warranted to detect fetal complications and polyhydramnios. 10
Large chorioangiomas may undergo spontaneous infarction with decreased echogenicity, tumour volume and blood flow on colour Doppler. 2 Improvement of the clinical symptoms with favorable outcomes may be seen with the appearance of calcifications and reduced blood flow within the tumours. 9 Poor outcome correlates with the amount of additional vascularized tissue that the fetal cardiovascular system must perfuse and support, hence the importance of Doppler evaluation. 9
3D ultrasound facilitates a more precise evaluation of the placental surface features, vasculature and perfusion patterns. 3D surface-rendered images may add to the accuracy of diagnosing placental abnormalities, although their role has not yet been determined. 11
A review of the literature reveals a dismal prognosis regarding chorioangiomas diagnosed antenatally, because more than half of these pregnancies end either prematurely or in termination of the pregnancies or perinatal death. Therefore, every effort should be made to diagnose these lesions and their complications as early as possible. 9 An early diagnosis might result in improved outcomes with closer follow-up and the use of therapeutic interventions as indicated. 3 Small tumours are usually monitored with ultrasound every 6–8 weeks, whereas large tumours require serial ultrasound examinations every 1–2 weeks. 12 At our institute in South India, neonatal salvage rates are very poor for babies weighing less than 1000 g. It was the opinion of our gynaecologists that, in this case, prolonging the pregnancy would give a better chance for fetal survival and therefore delivery was delayed until 34 weeks. We believe earlier intervention is unlikely to have changed the outcome for this infant.
Chorioangioma is usually treated with expectant management. Possible interventions for maternal or fetal complications include serial fetal transfusions, fetoscopic laser coagulation of the vessels supplying the tumour, chemosclerosis with absolute alcohol and endoscopic surgical devascularization. 2
In cases for which ultrasound findings are equivocal, magnetic resonance (MR) imaging may be performed and a chorioangioma may appear as a heterogeneous mass with high T2 signal intensity. 2 There are no studies to demonstrate the sensitivity and specificity of MR imaging in distinguishing chorioangioma from other placental lesions, or if MR imaging can reveal smaller lesions than can ultrasound. 2 Therefore ultrasound with colour Doppler provides the mainstay for the antenatal diagnosis and surveillance of placental chorangiomas.
Conclusion
Chorioangioma is a benign tumour of the placenta but larger lesions are associated with maternal and fetal morbidity and mortality. Serial ultrasound examination and colour Doppler imaging should be performed in all cases to assess the growth and vascularity of the tumour, growth of the fetus, and development of fetal and maternal complications.