
Abstract
Objectives
Postoperative complications associated with endovascular aneurysm repair (EVAR) mandate the need for lifelong surveillance. The aim of this audit was to compare the detection rates of endoleaks during the first 10 months of a combined sonographer-led colour Doppler ultrasound (CDUS) and radiologist-led contrast-enhanced computed tomography (CECT), postoperative EVAR surveillance programme, within a single National Health Service Hospital.
Methods
A prospective audit was carried out of all patients with EVAR, who had same-day CECT and CDUS surveillance examinations between March 2010 and January 2011. CECT examinations were reported by three consultant vascular radiologists. Of 66 CDUS examinations, 64 (97%) were performed and reported by four certified vascular sonographers. The reports of dual-modality, same-day scans were compared, to establish agreement on the presence and classification of the type, or absence of endoleaks. CECT was used as the gold standard, against which the sensitivity and specificity of CDUS in endoleak detection was determined.
Results
Sixty-six paired same-day CECT and CDUS reports were compared. Ten endoleaks were identified by CECT (15% incidence) and eight (80%) of 10 were type II. The number of observed agreements was 58 (88%) of 66; CDUS missed six endoleaks (five type II) and suggested two false-positives. CDUS had a sensitivity of 40% and a specificity of 96%. Conclusions: In our study, CDUS demonstrated an excellent specificity but had a low sensitivity for endoleak detection. We agree CDUS cannot effectively replace CECT as the sole imaging modality. Research to determine an international consensus for an effective and efficient postoperative EVAR surveillance patient pathway is required.
Introduction
Postoperative complications associated with endovascular aneurysm repair (EVAR) mandate the need for lifelong medical imaging surveillance. 1 These complications include endoleaks, 2 which are classified into five types (see Table 1).3-5
Endovascular aneurysm repair endoleak classification

Currently, contrast-enhanced computed tomography (CECT) remains the gold standard for postoperative EVAR surveillance to detect endoleaks.6-8 It is favoured for its high diagnostic accuracy, uniformity, availability, fast acquisition and reproducibility.1, 3 Its use as a lifelong surveillance tool is limited by factors such as a high dose of radiation, 9 injection of nephrotoxic contrast 10 and high cost. 11 Previous studies have suggested using duplex ultrasound (US) as an alternative postoperative EVAR surveillance modality.12-16 This modality is a safe option for patients with impaired renal function and those at risk of adverse reactions to contrast media, 10 uses no ionizing radiation and is more financially feasible. 11 The mobility of ultrasound machines is another key advantage over static CECT scanners. 17
Since 2005, EVAR has been performed within our Trust (York Teaching Hospital NHS Foundation Trust), on men and women with either an incidentally detected abdominal aortic aneurysm (AAA), a symptomatic AAA or a haemodynamically stable, ruptured AAA. Between 2005 and 2010, patients underwent postoperative EVAR surveillance, using CECT and abdominal radiographs, at one and 12 months and annually thereafter. In March 2010, based on a limited literature search,12-16 our Trust implemented colour Doppler ultrasound (CDUS) as a secondary surveillance method alongside CECT. The EVAR postoperative surveillance programme now consists of a same-day CECT and sonographer-led CDUS examination, at one and 12 months and annually thereafter.
The aim of this audit was to compare the detection rates of endoleaks, during the first 10 months of a combined sonographer-led CDUS and gold standard, radiologist-led CECT, postoperative EVAR surveillance programme, within a single National Health Service (NHS) Hospital.
Methods
Location
York Teaching Hospital NHS Foundation Trust.
Patient selection
JSF and MJN reviewed the Radiology Imaging System (RIS) reports of all patients enrolled in the postoperative EVAR surveillance programme. The reports of each pair of same-day, dual-modality EVAR surveillance examinations, from between March 2010 and January 2011, were included for analysis. Any patients, who died or did not have the same day dual-modality examination, were excluded from the final statistical analysis.
Type of EVAR stent and imaging practice
The stent-graft used in all EVARs was the Zenith Flex® (Cook Ireland Limited, Limerick, Ireland).
The EVAR procedures were done in conjunction with a vascular surgeon. Three consultant radiologists, with 4–6 years experience of the EVAR procedure and CECT EVAR interpretation, carried out the procedures and reported the patient's surveillance CECT (Table 2). The four sonographers, who carried out and reported the CDUS scans, hold a post-graduate certificate in vascular ultrasound. The sonographers and radiologists received in-house CDUS EVAR theoretical and practical mentoring by radiologist 3, and had less than one year's experience of using the technique (Table 2).
Practitioner experience in carrying out endovascular aneurysm repair procedures and reporting the postoperative contrast-enhanced computed tomography and colour Doppler ultrasound surveillance scans
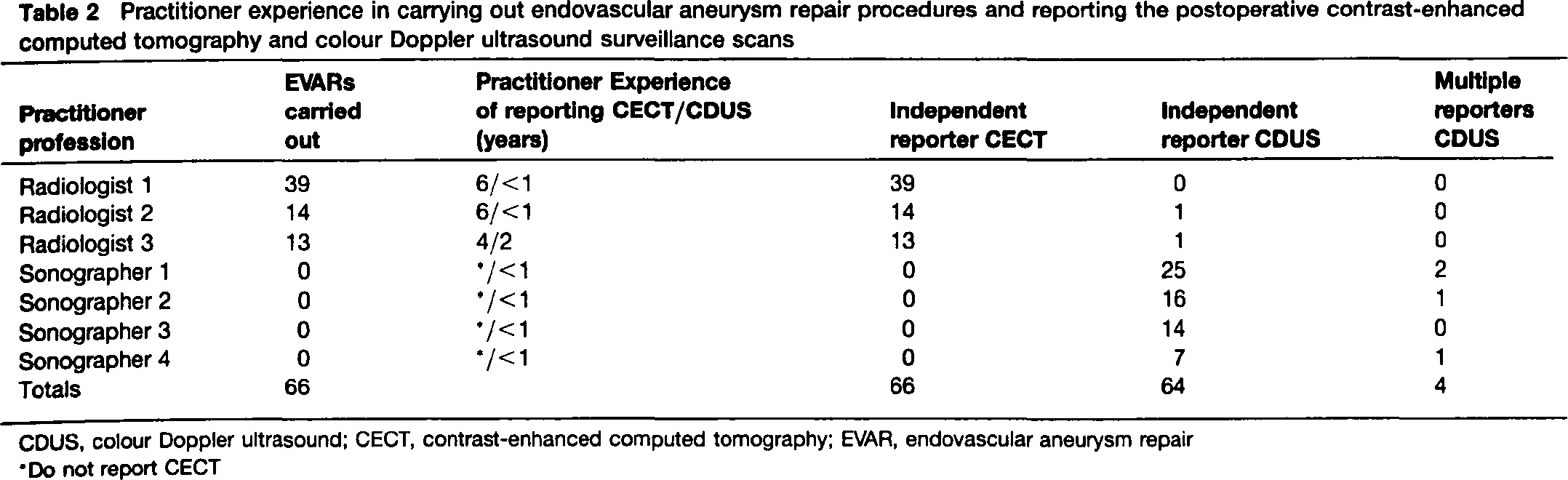
CDUS, colour Doppler ultrasound; CECT, contrast-enhanced computed tomography; EVAR, endovascular aneurysm repair
Do not report CECT
All CECT scans were carried out using the Siemens Somatom Sensation 16 (Siemens AG, Munich, Germany) with collimation and slice thickness of 16 × 0.75 mm and 300 mg Iodine/mL of Iopromide (Ultravist, Schering AG. Berlin, Germany). CECT multiplanar reformatting was performed with various third party software packages. All CDUS scans were carried out using the Philips iU22 xMATRIX with a 4 MHz ///broadbandwidth curvilinear transducer (Koninklijke Philips Electronics NV, Amsterdam, Netherlands). A standardized protocol12-16 and equipment pre-set were used. The B-mode pre-set included compound and harmonic imaging to improve image quality, which aids in the visualization of the endpoints, when measuring aortic diameters. To detect low flow velocity endoleaks, the wall filter was set to the minimum level and the colour Doppler velocity scale was set at 10 cm s−1 and reduced if further image optimization was required.
Both modalities were used to determine: the maximal outer to outer antero-posterior and transverse diameter of the aneurysm sac, the presence or absence of endoleaks, stent-graft deformations 18 , and the classification of the type of endoleak (Table 1).3-5
Data collection
Patient demographics, modality reports and patient outcome data were stored in an anonymized database; individual informed consent was not required as these were retrospective data. The authors sought and obtained local clinical governance approval (Project no. 1589) for carrying out and presenting the data as an audit.
All CECT and CDUS scans were technically satisfactory to enable diagnosis. Where there was no discussion in the RIS report regarding endoleaks, it was deemed that no endoleaks had been identified. MJN reviewed the images on the Picture Archiving and Communication system to determine reasons for disagreement between modalities.
Data analysis
Data were analysed using descriptive, median (range) and contingency tables to determine sensitivity and specificity for CDUS.
A benchmark sensitivity of 90% was set to determine the acceptability of CDUS against the gold standard CECT. This was chosen as several studies, which recommend the use of CDUS, have suggested sensitivities of CDUS endoleak detection in excess of 90%.13-15
Results
Radiology reports for 88 patients, enrolled in a post-EVAR surveillance programme, were reviewed. Of 88 patients, 23 (26.1%) were excluded, 12 (13.6%) because they died before CDUS was incorporated into the surveillance programme and 11 (12.5%) because they did not have a same-day CDUS and CECT scan. This was for a variety of reasons, such as missed appointments and scheduling conflicts. Of the 88 patients, 64 (72.7%) had one same-day scan and one patient (patient 8, Table 3) (1.1%) had two same-day scans, giving 66 paired scans to compare. In 26 (39.4%) of the 66 cases, CDUS was done first and CECT second. In 40 (60.6%) of the 66 cases, CECT scans were done before the CDUS scans.
Endoleaks detected by contrast-enhanced computed tomography and/or colour Doppler ultrasound

CDUS, colour Doppler ultrasound; CECT, contrast-enhanced computed tomography
CDUS and CECT were unable to comment on whether there was an increase in sac size, as this was the one month baseline postoperative endovascular aneurysm repair scan
Fifty-nine (90.8%) of the 65 patients, with at least one paired same-day scan, were men and six (9.2%) were women. The median age of all patients at the time of their EVAR was 77 years (range 58–89). Median age at time of surveillance for all patients was 79 years (range 62–91).
Reporting practitioners
Of the 66 CECT examinations, carried out on the same-day as their paired CDUS scan, Radiologist 1 reported 39 (59%) of 66, Radiologist 2 reported 14 (21%) of 66 and Radiologist 3 reported 13 (20%) of 66 (Table 2). All 66 CDUS results were known by the radiologist reporting the CECT. The 66 CDUS examinations, carried out on the same-day as their paired CECT scan, were independently reported by sonographers or radiologists in 64 (97%) of 66 cases. Two (3%) of 66 were reported by multiple practitioners (Tables 2 and 3).
Detection and classification of the type of endoleaks
All patients diagnosed with endoleaks by CECT or CDUS were men with a median age at time of surveillance of 81 years (range 69–91). Median surveillance time since their EVAR was nine months (range 1–24).
The agreement and disagreement of CECT and CDUS for the detection of endoleaks is shown in Tables 3 and 4. Endoleaks were detected by CECT in 10 (15.5%) of 66 scans and in six (9%) of 66 CDUS scans. The two modalities agreed in 58 (87.9%) of 66 cases; in four cases they both agreed on the presence of an endoleak and in 54 cases they both agreed on the absence of an endoleak. They disagreed in eight (12.1%) of 66 cases; an endoleak was identified by CECT but not CDUS in six cases, whereas in two cases an endoleak was detected by CDUS but not identified by CECT. CDUS had a sensitivity of 40% and a specificity of 96%. The low sensitivity of ultrasound was attributed to sonographers 1 and 4, as they missed all six endoleaks (Table 3). The two false-positive findings were detected by Sonographer 2.
Two by two contingency table to show the endoleak detection rate for contrast-enhanced computed tomography and colour Doppler ultrasound

Ten endoleaks were detected by the gold standard CECT: eight type II (80.0%), one type I (10.0%) and one type III (10.0%). CDUS detected six endoleaks: three type I leaks (50.0%), two type II (33.3%) and one type III (16.7%). Both CECT and CDUS concurred on the presence of endoleaks on four (33.3%) of 12 occasions and agreed on the type of leak in one (25%) of four cases (Tables 3 and 4).
Discussion
The implementation of our new postoperative EVAR surveillance service, incorporating CDUS with CECT, raises several issues that are relevant to translating research into clinical practice. 19 These include: incidence of endoleaks, detection rate and the classification of the type of endoleaks identified using different modalities, experience of the practitioner performing the examination and reproducibility of the findings between practitioners.
Detection and classification of the type of endoleaks
In this audit, 10 endoleaks in 66 CECT scans were identified, an incidence of 15%, which is comparable to the range of 11–20%, reported by previous studies.7, 20-22 Other studies gave a much higher incidence, such as 39–44%.23, 24 The audit's low sensitivity of 40%, when using solely CDUS, compared with the benchmark sensitivity of 90%,13-15 suggests our sonographer-led service was not an effective means of endoleak detection. This is not unique and mirrors previous studies, reported by vascular sonographers/technologists, with low CDUS sensitivities of 12–56%.6, 25-27 Several studies found ultrasound was very sensitive, greater than 90%, for endoleak detection, compared with the gold standard CECT.13-15 Two systematic reviews, which evaluated CDUS and duplex ultrasound techniques, concluded that non-contrast ultrasound does not have sufficient diagnostic accuracy for sole use in endoleak detection. 28
In this study, where CDUS and CECT concurred on the presence of an endoleak (Table 3), the agreement on the classification of the type was weak (1 of 4 cases [patient 3]). The CDUS and CECT images for the four patients were reviewed by MJN, and further discussed with the vascular surgeon due to the endoleaks discrepancy (Table 5). Failure to correctly identify the type of leak may result in the incorrect re-intervention. 3 The learning points are that type II leaks can masquerade as either type lb or III on CDUS but this can usually be resolved by CECT. If the sac is small, as in patient 2, on ultrasound, flow in a vessel travelling close to the sac can be mistaken for flow within the sac.
Imaging findings, outcome and current status of patients with endoleak present on both modalities
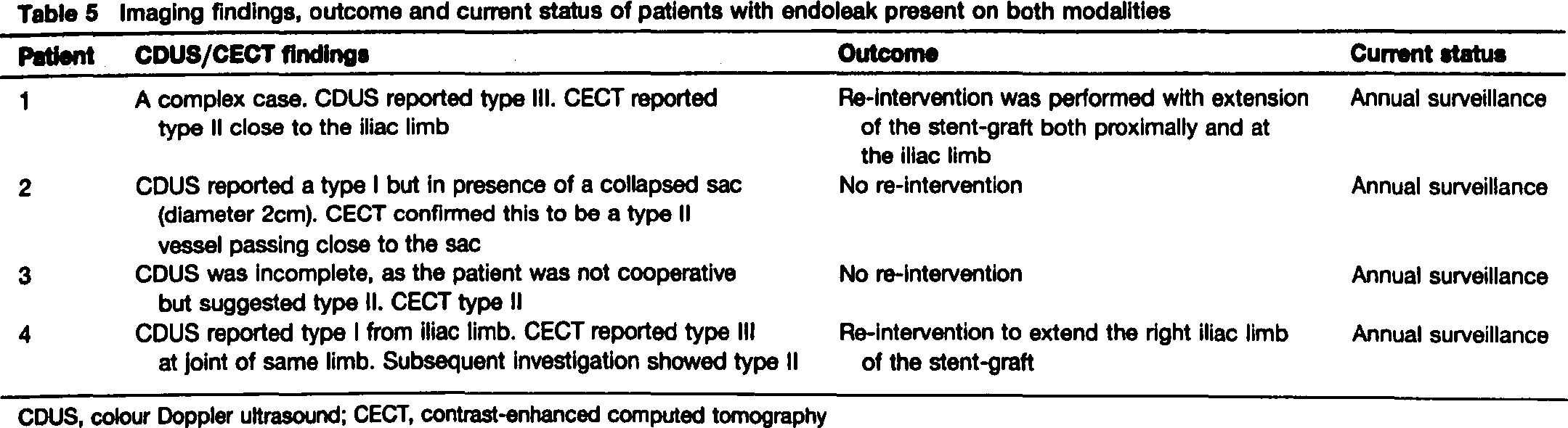
CDUS, colour Doppler ultrasound; CECT, contrast-enhanced computed tomography
CDUS missed six endoleaks, one type I and five type II. The type I leak missed was significant; patient 10 underwent re-intervention, despite neither modality recording sac expansion. Type II endoleaks are the most common type, occurring in 10–25% of EVARs (Table 3). 4 The latter significantly affected the overall sensitivity. None of the patients with missed type II leaks had sac expansion and they were scheduled for routine surveillance. Two other studies found a similar pattern of outcomes for type II endoleaks.6, 17 Endoleaks have an unpredictable behaviour and can spontaneously seal and re-occur. 23 While 30–100% of type II endoleaks will resolve spontaneously, 4 when they become problematic, they are associated with an increase in the diameter of the aneurysm sac, which CDUS is effective at identifying. 8 In the absence of sac expansion, type II leaks may be viewed as clinically insignificant, and no cause for concern.6, 27
If CDUS shows sac expansion in the absence of an endo-leak, a contrast-enhanced ultrasound (CELTS) 27, 28 or CECT scan should be done to locate the source of blood flow to the sac and evaluate the need for re-intervention. 16 The two CDUS false-positives were not noted to experience sac enlargement or require any re-intervention.
Although an agreed CDUS technique12-16 was followed to ensure a standardized EVAR assessment, the technique may have differed between examinations due to practitioner experience and patient dependency, 1 which can result in long scan times compared with the fast acquisition of CECT. 7 A challenging body habitus and over-lying bowel gas are well known to lead to suboptimal examinations and can compromise results. 29 Patients with a large body mass and over-lying bowel gas may benefit from sole CECT imaging to prevent CDUS missing endoleaks, as CECT is less influenced by body habitus and the presence of gas. 23
This audit and previous research has shown heterogeneity in the incidence, detection rate and classification of the type of endoleak, 30 which may be due to differences in postoperative EVAR surveillance timing, the modality used, the technical capabilities of the chosen modality and the level of training and experience of the reporting practitioner.3, 30, 31 In the context of hospital-based detection of abdominal aortic aneurysms (AAA) and the implementation of national AAA screening programmes,32, 33 the differences in postoperative EVAR surveillance practice may have international implications. It may lead to differences in cost-effectiveness, patient satisfaction and overall outcomes after EVAR.34, 35
Strengths and limitations
The strength of this audit, compared with previous studies, was the carrying out of CDUS and CECT on the same day.15, 23 Despite the same-day scanning, CDUS still had a low sensitivity, which cannot be attributed to a time lapse between CDUS and CECT scans.
A limitation of this study was the number of inexperienced reporters and the variation in the number of examinations carried out by each sonographer and Radiologist 3, the mentor for the other practitioners (Table 2). This may explain why sonographer 4 missed four of the six undetected endoleaks and sonographer 2 overcalled (potentially) both false-positive scans (Table 3). Due to the small subset of patients, it is not possible to determine the statistical significance of these findings. It is also possible the endoleaks may have been missed if they had been allocated to a different sonographer's list. Ideally, all the examinations and reports would be completed by one consultant radiologist with the most experience in interpreting CECT and CDUS examinations, as sonographers do not report CECT EVAR examinations. This would make the comparison of CDUS against CECT consistent and eliminate inter-observer variability.14, 18, 36 This is not appropriate within imaging departments, where consultant radiologists have other duties and most vascular sonographers/technologists carry out and report the majority of their own ultrasound examinations.
A potential limitation of the study was that CDUS and CECT reporters were not always blind to the images and results of the other modality. Sonographers were blind to all CECT reports, as they reported the CDUS on the same-day and the CECT was not reported until several days after the scan. In the 40 cases, where CECT was done before the CDUS, the sonographers did not review the CECT images. Radiologists reporting the CECT were able to refer to all CDUS static images and the report. This may have potentially influenced the CECT reporters’ decision to agree with the other modality (Table 3). Radiologists would have considered CECT as the ‘gold standard’ and would not under (or over) report a leak based on the CDUS report. If the methodology of this study was repeated, blinding the results would remove potential influence and bias. 16
Although CECT is the agreed gold standard, we cannot exclude the possibility that the two CDUS false-positives were actually endoleaks missed by CECT. 3
Recommendations for practice
Vascular services, who are considering introducing or developing an ultrasound EVAR surveillance programme, should consider organizing for radiologists and sonographers to visit and receive training and education in units, which have substantial experience of CECT, CDUS and CEUS EVAR surveillance. This, as well as in house training, may improve diagnostic accuracy and reproducibility.
To maximize experience in CDUS and CEUS EVAR surveillance, it would be sensible to: (i) implement the service with two experienced vascular sonographers/technologists carrying out and reporting CDUS and CEUS and two radiologists reporting the CECT and (ii) have a minimum number of supervised scans, by an experienced practitioner, before independent reporting of the CDUS and CEUS studies. 37
As some endoleaks are more serious than others and require re-intervention, continued learning for health-care practitioners and regular multidisciplinary meetings, to increase endoleak detection rate and improve the agreement of classification of the type of endoleaks, is needed. In departments where sonographer-led CDUS for EVAR surveillance is in its infancy, diagnostic accuracy should be audited again after two years. Sonographers will become more experienced and confident at identifying endoleaks over this duration. This may lead to increased diagnostic accuracy.
International consensus on a standardized patient pathway for postoperative EVAR surveillance is required. A suggested pathway may be as in Figure 1, with the initial imaging being US and a plain abdominal radiograph (AXR). 38 The surveillance interval needs to be determined.

A suggested patient pathway for postoperative endovascular aneurysm repair surveillance. AXR, plain abdominal radiograph; CDUS, colour Doppler ultrasound; CECT, contrast-enhanced computed tomography; CEUS, contrast-enhanced ultrasound
Recommendation for research
Research, with a realistic evaluation design, is required to evaluate effective and efficient postoperative EVAR surveillance in terms of timing, the modality to use (Doppler ultrasound, CEUS, AXR, CECT or magnetic resonance angiography) and the type of training and experience required for the reporting practitioner.
Conclusion
This study has an excellent specificity. Our low sensitivity, using CDUS, for the detection of EVAR endoleaks, shows we could not reproduce the favourable results of other centres. We agree that CDUS cannot effectively replace CECT as the sole imaging modality, but may be used as an initial radiation-free tool in patients with stable sac diameters, as most problematic endoleaks are associated with sac expansion. 8
The search for a sensitive, safe and cost-effective means of postoperative EVAR surveillance continues and many studies have compared the success of different modalities. CECT remains the gold standard postoperative EVAR surveillance modality despite its disadvantages.6, 7, 12 Research to determine an international consensus for an effective and efficient postoperative EVAR surveillance patient pathway is required.
Declarations
Footnotes
Acknowledgements
We are grateful to all of the sonographers and radiologists from York Teaching Hospital, for carrying out the radiology examinations in this study.