
Abstract
Streptococcus equi is a common equine infectious disease, but transmission to man is rare and confined to those who commonly come into close contact with horses. Similarly, prosthetic stent graft infection is a rare complication of endovascular aortic aneurysm repair. We describe the first reported case of aortic stent graft with S. equi occurring in a professional racehorse trainer. Clinical presentation, investigations, imaging and management of this case are described. In conclusion, clinicians should consider infection with rare organisms in patients with prosthetic implants who regularly come into contact with horses and other ruminants.
Introduction
Stent graft infection following endovascular aortic aneurysm repair (EVAR) is a rare complication and the exact incidence is unclear as long-term follow-up continues. The available literature reports suggest an aortic stent graft infection rate of 0.43–0.50%.1,2 Aortic stent graft infection is associated with significant morbidity and high mortality. We describe the first reported case of an aortic stent graft infection caused by an extremely rare pathogen, Streptococcus equi (S. equi), in a professional racehorse trainer. Advanced imaging studies are described and currently available literature is reviewed.
Case report
A 69-year-old male patient was admitted with a six-month history of intermittent pyrexia, rigors, feeling generally unwell with lethargy, myalgia and night sweats. Recent history included two weeks of a cough with white sputum. He had received intermittent courses of amoxicillin from his general practitioner with only partial resolution of the pyrexia over the last six months. Past medical history included pulmonary tuberculosis as a child. His occupation was a racehorse trainer and he was a frequent traveler to Zambia for charity work. He took no anti-infective prophylactic treatment against common tropical diseases during these trips. There was no history of blood transfusions, insect bites or tropical illness while in Zambia. Two years prior to this episode, he underwent an EVAR with a Zenith Trifab aortic stent (Zenith, Cook Europe, Bjaeverskov, Denmark) for a symptomatic enlarged abdominal aortic aneurysm (size 5.6 cm). The original implantation procedure was a standard bifurcated EVAR via small vertical groin incisions under general anesthesia without central line insertion or arterial lines.
The procedure was uneventful and there were no early postoperative complications and a computed tomography (CT) scan performed at six months showed a good technical result, i.e. the stent graft was in a good position with no migration or endoleaks (Figure 1a). During the current hospital admission, clinical examination was unremarkable except for high-grade pyrexia. Initial investigations showed raised inflammatory markers (total white cell count 17.8 × 10
9
/L and C-reactive protein >250 mg/L). Initial septic screen for common bacterial, parasitic and viral infections were negative. Repeated cultures of blood, urine, sputum, stool and cerebrospinal fluid failed to identify the causative organism. Serological tests for mycoplasma, brucella and bartonella, and tests for HIV, hepatitis B, hepatitis C, influenza A, influenza B and adenovirus were also negative.
Axial contrast enhanced computed tomography images: (a) 6 months post-endovascular aortic aneurysm repair (EVAR) and (b) 2 years post-EVAR. (a) Normal post-stent appearance at six months with both limbs visible in the aneurysm sac. At two years (b), there is abnormal thickening and enhancement of the wall of the aneurysm sac with ill-defined stranding in the peri-aortic fat (a) Coronal planar image of an indium-labeled white cell study at 22 h showing focal increased white cell activity to the left of the midline in the lumbar region at the site of the aortic aneurysm sac (black arrow). (b) 18-F FDG PET-CT coronal reformatted image demonstrating corresponding abnormal increased FDG uptake in the walls and sac of the abdominal aortic aneurysm (black arrow). Note normal physiological activity in the bladder, heart and brain. FDG, fluorodeoxyglucose; PET-CT, positron emission tomography computed tomography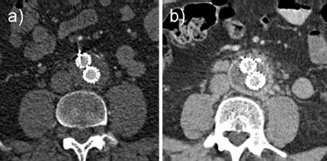
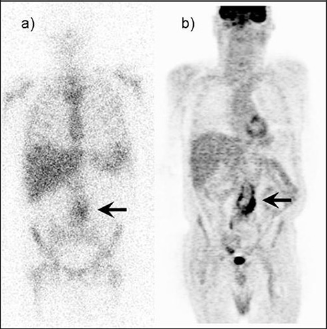
A CT scan of the chest was normal, but a CT scan of the abdomen revealed abnormal thickening and enhancement of the wall of the aneurysm sac with ill-defined stranding in the peri-aortic fat suggestive of a possible aortic stent infection (Figure 1b). An indium-labeled white cell study revealed focal increased white cell activity in the midline of the lumbar region at the site of the aortic aneurysm sac (Figure 2a). Corresponding abnormal fluorodeoxyglucose (FDG) uptake was demonstrated in the walls and sac of the aneurysm on a FDG positron emission tomography CT (PET-CT) scan (Figure 2b). Initial management consisted of antimicrobial therapy with vancomycin, gentamicin and rifampicin due to the high morbidity and mortality associated with surgical removal of the stent graft. Despite treatment, the patient developed new onset severe back pain, persistent pyrexia and worsening of his inflammatory markers. To maximize the chances of infection eradication and to provide further tissue for diagnostic purposes, it was decided to surgically remove the stent graft. A conservative estimate of 20–30% risk of mortality was given for this procedure, based on a general estimate for mortality of removing infected grafts as well as based on previous literature. 2 With the aorta clamped at the level of the diaphragm and the iliac arteries controlled, the aneurysm sac was incised to expose the stent graft. Pus was found within the aneurysm sac surrounding the stent graft. A finger was placed between the graft and the inside of the suprarenal aorta to disengage each stent graft spike in turn. Once all spikes had been freed, caudal traction was applied to remove the stent. The iliac limbs of the graft were removed without difficulty and the aortic stumps were oversewn with a double layer of 2/0 Prolene sutures. Anatomic reconstruction with harvested femoral vein or rifampicin-bonded grafts were considered, but rejected on account of the unknown nature of the infectious agent we were dealing with and therefore its effect on an in situ graft could not be predicted. Also, the poor clinical condition of the patient indicated that a relatively quick procedure with a low risk of complications would give the best chance of survival. Therefore, an extra-anatomical bypass was performed in the form of an axillobifemoral bypass using a polytetrafluoroethylene (PTFE) graft. The stent graft was sent for microbiological examination. Perioperatively, the patient was treated with vancomycin and meropenem (a β-lactam antibiotic: carbapenem). Culture of the material removed at operation was negative, but polymerase chain reaction (PCR) of the 16S ribosomal deoxyribonucleic acid (rDNA) subunit performed at Great Ormond Street Hospital, London identified the causative organism as S. equi. 3 The main reason as to why the 16S rDNA PCR was used is that the patient received antibiotics, and so bacterial culture was negative (i.e. no viable organism present), but we were able to make the diagnosis by amplification of the remaining DNA. Intravenous teicoplanin was continued for a further six weeks and subsequently changed to oral amoxicillin for two years. He made a good recovery, incisions healed well, limbs were well perfused and there were no abdominal complications. The patient returned to normal functioning quickly, was discharged from hospital two weeks after surgery and returned to normal function within three months. A CT scan six months post-operation showed no signs of residual intra-abdominal sepsis. Two years post-surgery, he remains in excellent health.
Discussion
Following EVAR, aortic stent graft infection is rare. Literature in this area is still developing. Graft infection following open aneurysm repair, however, is well described. The causative organism in over 50% of cases is Staphylococcus species. 4 Human infection with S. equi is rare, and to our knowledge, aortic stent graft infection with S. equi has not been previously described.
S. equi is a Gram-positive bacterium, and is the causative agent of strangles, a common infectious disease of horses. S. equi belongs to the pyogenic group of streptococci and to group C of the Lancefield classification. It consists of three subspecies (subsp.) of zoonotic agents rarely reported as human pathogens:5,6 S. equi subsp. equi, S. equi subsp. zooepidemicus and S. equi subsp. ruminatorum. S. equi subsp. equi and S. equi subsp. zooepidemicus are zoonotic agents implicated in diverse animal infections such as strangles, mastitis, abscesses, wounds, and respiratory and uterine infections. Human infection with this organism is very rare and the clinical presentation may vary according to subspecies of the organism. Therefore, there is no typical presentation of this infection in humans. There are few reports in the literature for human infections caused by S. equi subsp. equi, and S. equi subsp. zooepidemicus. The human infections include outbreaks of food-borne diseases, 7 meningitis, septicemia, arthritis, pneumonia, glomerulonephritis and streptococcal toxic shock syndrome. These infections can occur in both immunocompromised and immunocompetent patients.5,6,8,9
Aortic stent graft infection almost always requires removal of infected stent graft and extra-anatomic bypass. One of the main difficulties in removing this type of stent graft is its suprarenal fixation with metal spikes of uncovered stent, which penetrate the aortic wall above the level of the renal arteries. Removal of this stent graft could potentially cause aortic wall rupture and catastrophic hemorrhage. Manual removal by hand as well as re-sheathing with a modified 20 mL syringe has been described and the hand method was the technique employed here. 10 As the number of EVARs performed increases, the occurrence of this type of infective complication may also increase, thus providing challenging management decisions.
In conclusion, removal of an infected aortic stent graft with suprarenal fixation is a technically demanding procedure but can be performed successfully. Clinicians should consider infection with rare organisms in patients with prosthetic implants who come into close contact with horses and other ruminants. Molecular techniques should be considered when conventional culture methods have failed to identify the infective agent.