
Abstract
This study compares outcomes of basilic and cephalic vein fistulas for hemodialysis. A retrospective review of arteriovenous fistulas in a university hospital system was performed using charts and hemodialysis records. Patency and demographic data were assessed with life table analysis. One hundred fifty-six patients (88 males; 68 females) underwent creation of 172 autogenous fistulas (mean age 61 years; mean follow-up 78 weeks). There were 101 basilic vein transpositions and 71 cephalic vein fistulas. Primary patency did not differ significantly, while assisted primary patency was significantly better for basilic vein fistulas at one year (73% versus 53%: P = 0.024). Secondary patency was significantly better for basilic fistulas through three years (58% versus 52%; P = 0.027). Primary failure (thrombosis before access or failed maturation) was significantly higher for cephalic than basilic fistulas (28% versus 13%; P = 0.01). Maturation time, usage time and complications were not significantly significant. Thirty-three (33%) basilic vein-based fistulas and 12 (17%) cephalic vein fistulas required revision during follow-up. Basilic vein-based fistulas perform as well as or better than cephalic vein-based fistulas in terms of patency, maturation time, and usage time and complication rates, though requiring more re-interventions.
Introduction
The incidence of end-stage renal disease is increasing and its prevalence in the USA is predicted to continue increasing. 1 With increasing longevity and an aging population, more patients will be hemodialysis-dependent for longer periods and at an older age. Creation and maintenance of hemodialysis access is an important public health concern.
The upper arm basilic vein to brachial artery fistula was first described by Dagher et al. in 1976. 2 Due to its deep location in the arm the basilic vein requires surgical transposition to a superficial location so that it can be more easily cannulated with hemodialysis needles. Surgical transposition of the basilic vein is more complicated and often requires more time when compared with surgical creation of a radiocephalic or brachiocephalic fistula. There have been many previously published studies that have reported excellent results with brachiobasilic fistulas. 3–9 However, some of these studies suggest that basilic vein-based fistulas have higher rates of complications including: (a) delayed or failure of maturation; (b) steal syndrome; (c) forearm edema; and (d) bleeding. 10–12 The 2000 National Kidney Foundation Dialysis Outcome Quality Initiative (DOQI) guidelines relegate upper arm basilic fistulas to second tier, along with prosthetic grafts and below brachiocephalic fistulas. 13 Although the 2006 K/DOQI Guidelines separate the basilic vein transpositions from prosthetic grafts, there is a clear bias towards the cephalic vein fistulas. 14
The purpose of the present study was to compare the outcomes of the basilic vein-based fistulas and cephalic vein-based fistulas in terms of patency, usage and complications. We expected to find that basilic vein-based fistulas had similar patency rates as compared with cephalic vein-based fistulas.
Materials and methods
Methods of data acquisition and inclusion/exclusion criteria
A retrospective review of charts and hemodialysis records was conducted of patients who underwent creation of autogenous fistulas for hemodialysis in a university health system between January 2001 and July 2005 and who underwent hemodialysis in the affiliated dialysis unit. Institutional Review Board permission was obtained for the study. All available data, including computerized patient records, clinic files and hemodialysis access data were reviewed using a paper-based data collection form. Demographic data, co-morbidities, patency and usage information were collected.
All patients who had autogenous fistulas created during this period for which follow-up data could be obtained were included. Patients undergoing creation of prosthetic grafts were excluded from this study. Patients who were lost to follow-up from the dialysis centers, due to relocation, were excluded. Records were obtained through hospital medical records, physician office billing records and dialysis center records.
Patient demographics
One hundred fifty-six patients underwent creation of 172 autogenous fistulas. One patient had four procedures, two patients had three fistulas and nine patients had two fistulas. There were 101 fistulas including 99 brachiobasilic and two ulnar basilic fistulas, and 71 cephalic vein-based fistulas, including 47 brachiocephalic fistulas and 24 radiocephalic fistulas in the cohort. All of the brachiobasilic vein fistulas were upper arm transposition fistulas. Eighty-eight men had 92 operations while 68 women had 80 operations. The cohort was comprised of 94 (60%) Caucasians, 57 (36%) African-Americans and five (3%) Native Americans. The mean age at the time of operation was 61 ± 16 years (range 14–92).
Preoperative evaluation
Physical exam
The preoperative arterial exam always consisted of bilateral upper extremity blood pressures, and an Allen test. Duplex ultrasound evaluation of the patient's upper extremity was routinely performed to determine the optimal conduit when the superficial veins were not clearly visible.
Ultrasound imaging
The choice of vein for fistula creation was based on preoperative duplex ultrasound in 145 patients (84%). Duplex ultrasound imaging was performed in Intersocietal Commission for the Accreditation of Vascular Laboratories accredited vascular laboratories, but due to different protocols between labs as to the use of tourniquet, statistical analysis of vein size was deemed unreliable. All superficial veins in both upper extremities were imaged to determine the most suitable vein for access. Arterial studies were done in the vascular lab when the surgeon had an equivocal Allen test. Table 1 depicts the site of the autogenous fistula.
Types of fistulas
Surgical procedure
The choice of autogenous fistula was surgeon-dependent and was based on preoperative clinical examination, duplex imaging and intraoperative findings of vein caliber and patency. When feasible, the cephalic vein at the wrist was always used preferentially. At the antecubital level, the vein preference was based on surgeon determination of the better vein.
All brachiobasilic fistulas were constructed in a single stage procedure with transposition of the vein, as described by Dagher et al. 2 Basilic vein fistula creation required either regional arm block or general anesthesia, while cephalic vein fistulas were usually performed with local anesthesia only with sedation, with rare use of regional arm block or general anesthesia dependent on patient cooperation. There were no delayed fistula elevation procedures in either the cephalic vein fistula or basilic vein fistula groups.
Follow-up methods
Follow-up was obtained through dialysis center records and a review of all hospital procedures for access during the study time period. All patients also followed up with the operating surgeon during the first month after access creation as well as at 2–3 months for determination of adequacy of the fistula for cannulation. The decision to begin needle cannulation of the fistula was made by the attending surgeon based on vein thickness and size, as well as presence of a thrill. Vein wall thickness was determined by duplex ultrasound in patients with failure to mature. Underdeveloped fistulas were further followed up at four weekly intervals to monitor maturation, and underwent duplex or angiographic imaging when appropriate. Failing accesses were determined by high venous pressures, cannulation problems or inability to achieve adequate dialysis. Patients with failing access underwent fistulograms for both diagnosis and intervention.
Statistical analysis and definitions
Definition of terms
Recommended standards for reports dealing with arteriovenous hemodialysis accesses were used. 15 Usage time was documented as time from first successful cannulation to most recent successful cannulation. Usage times were dependent on time after creation to first cannulation and patency. Since functional patency is dependent upon quantitative measurements of fistula flow and adequacy of dialysis by definition, 15 the term usage time was adopted for this retrospective study. Primary patency (PP), assisted primary patency (APP) and secondary patency (SP) rates were calculated in accordance with recommended reporting standards. 15 APP was achieved with angioplasty of stenotic lesions. SP was achieved either through endovascular mechanical thrombectomy, lysis and angioplasty or stenting of lesions, or open surgical thrombectomy, with intraoperative angiography, patching of anastomotic stenoses or angioplasty/stenting of more distal lesions. Patient survival, time to first use and usage times was also derived. Intervention-free patency rates were calculated taking into account all interventions, including those not aimed at prolonging fistula patency (i.e. banding for steal). These are not included in PP determination according to the reporting standards, which include only procedures aimed at prolonging patency.
Utilization rate was the percentage of fistulas that were eventually used for hemodialysis.
Failure rate was the percentage of fistulas that were abandoned without successful cannulation. These include those fistulas that thrombosed before successful cannulation and those that were abandoned due to failure to mature, even if they were patent. This is expressed as a percentage, independent of time variable, whereas maturation rates are expressed as a time-dependent percentage. In order to be classified as a failure to mature, a fistula will have to be abandoned with no further endeavors at achieving maturation.
Statistical methods for analysis
Analysis was by life table (SPSS, Chicago, IL, USA) with the Wilcoxon (Gehan) test for overall tendencies at one, two and three years. Analysis was on an intent-to-treat basis. Demographic data were compared using the Pearson chi-square test. Data are expressed as a mean with standard deviation. A P value of <0.05 was considered significant.
Results
In this study we retrospectively evaluated the long-term results of 172 autogenous fistulas that were created in 156 chronic hemodialysis patients. The study group included 101 basilic vein-based fistulas and 71 cephalic vein-based fistulas.
Mean follow-up was 78 ± 56 weeks (range 1–260). Fifty-one (31%) of the 156 patients died during follow-up. Fifty-six (33%) of the 172 fistulas thrombosed or were abandoned due to failure during follow-up. Patient survival rates at three years were not significantly different (basilic vein-based fistulas: 58%; cephalic vein-based fistulas: 67%, P = 0.73). The mean age at the time of fistula creation was not significantly different between basilic vein-based fistulas (60 ± 16) and cephalic vein-based fistulas (63 ± 16, P = 0.18). In patients with more than one fistula involving the same vein, co-morbidities were counted only once. Table 2 summarizes patient demographics by fistula type. Co-morbidities were similar with the exception of coronary artery disease and congestive heart failure, which were more prevalent in patients undergoing creation of a cephalic vein-based fistula.
Patient demographics
CHF, congestive heart failure; PVD, peripheral vascular disease; CAD, coronary artery disease
Patency
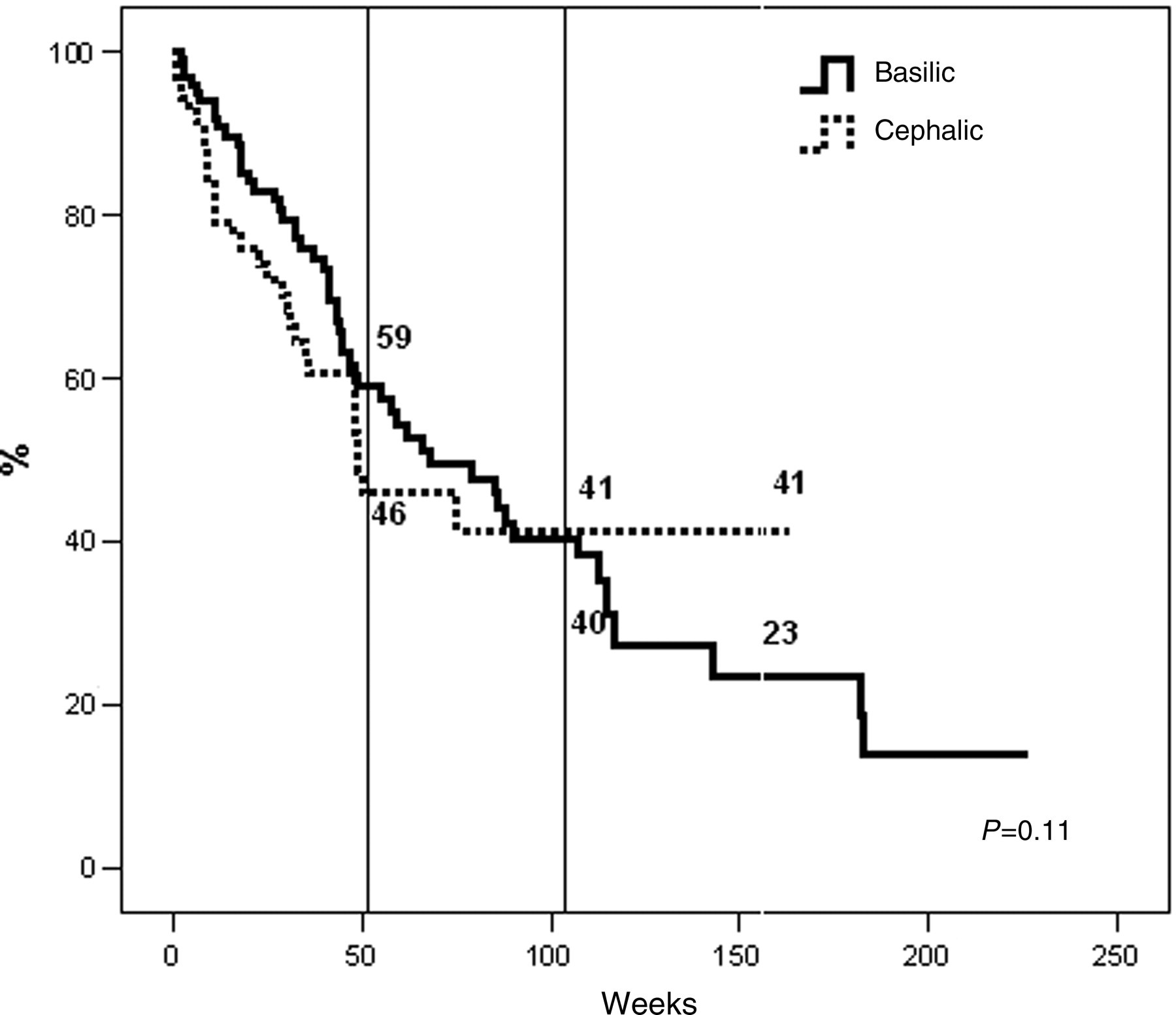
The one, two and three-year PP (Figure 1) was 61%, 42% and 24% for basilic vein-based fistulas, and 48%, 43% and 43% for cephalic vein-based fistulas, respectively (P = 0.11). The APP was significantly better for basilic vein-based fistulas at one year (73% versus 53%; P = 0.024). The rates were equivalent at two years and worse for basilic vein-based fistulas at three years (40% versus 49%; P = 0.042 overall, Figure 2). The SP was significantly better for basilic vein-based fistulas at one, two and three years, respectively (78% versus 56%; 61% versus 52%; and 58% versus 52%; P = 0.027 overall) (Figure 3).

Primary patency
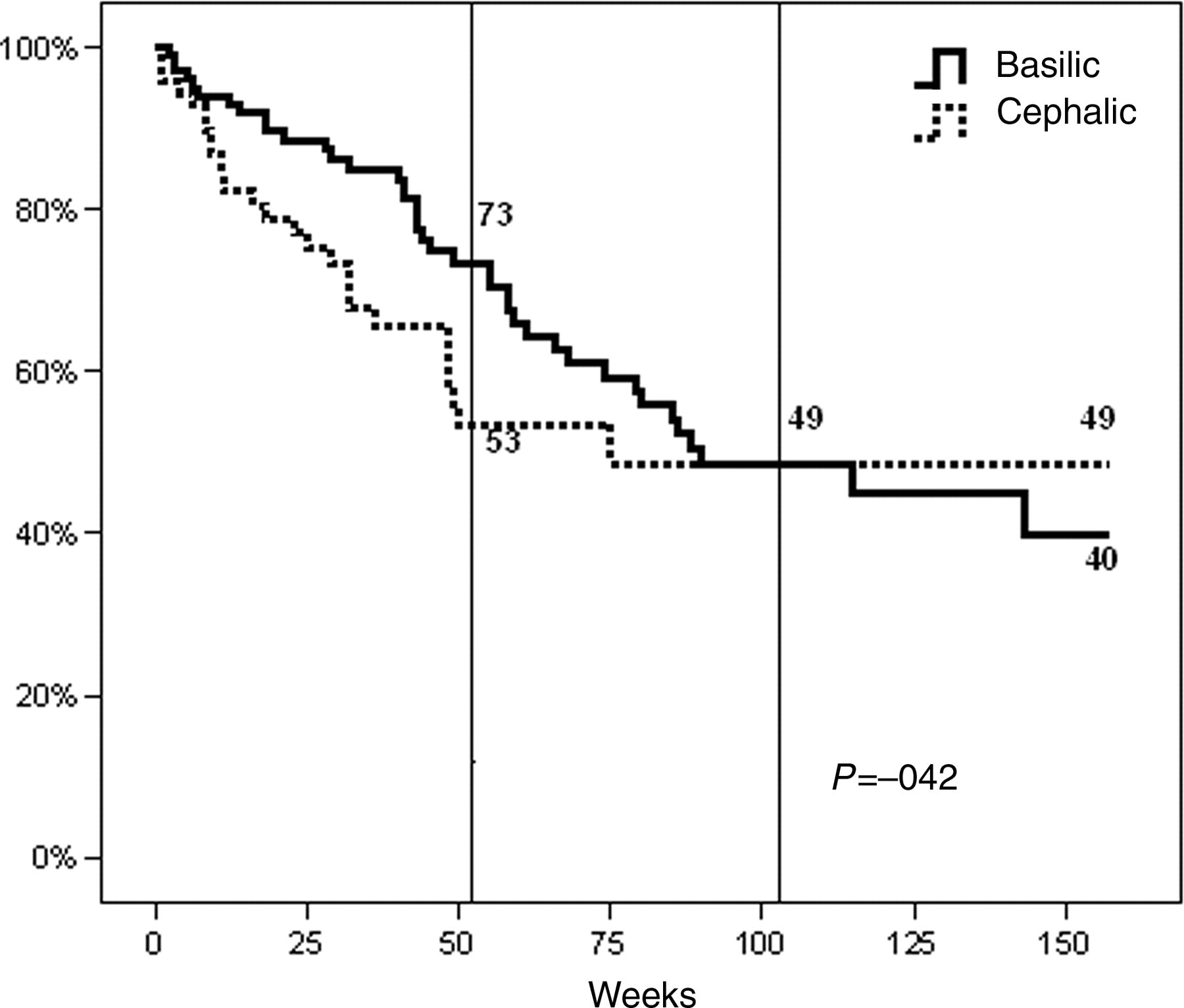
Assisted primary patency
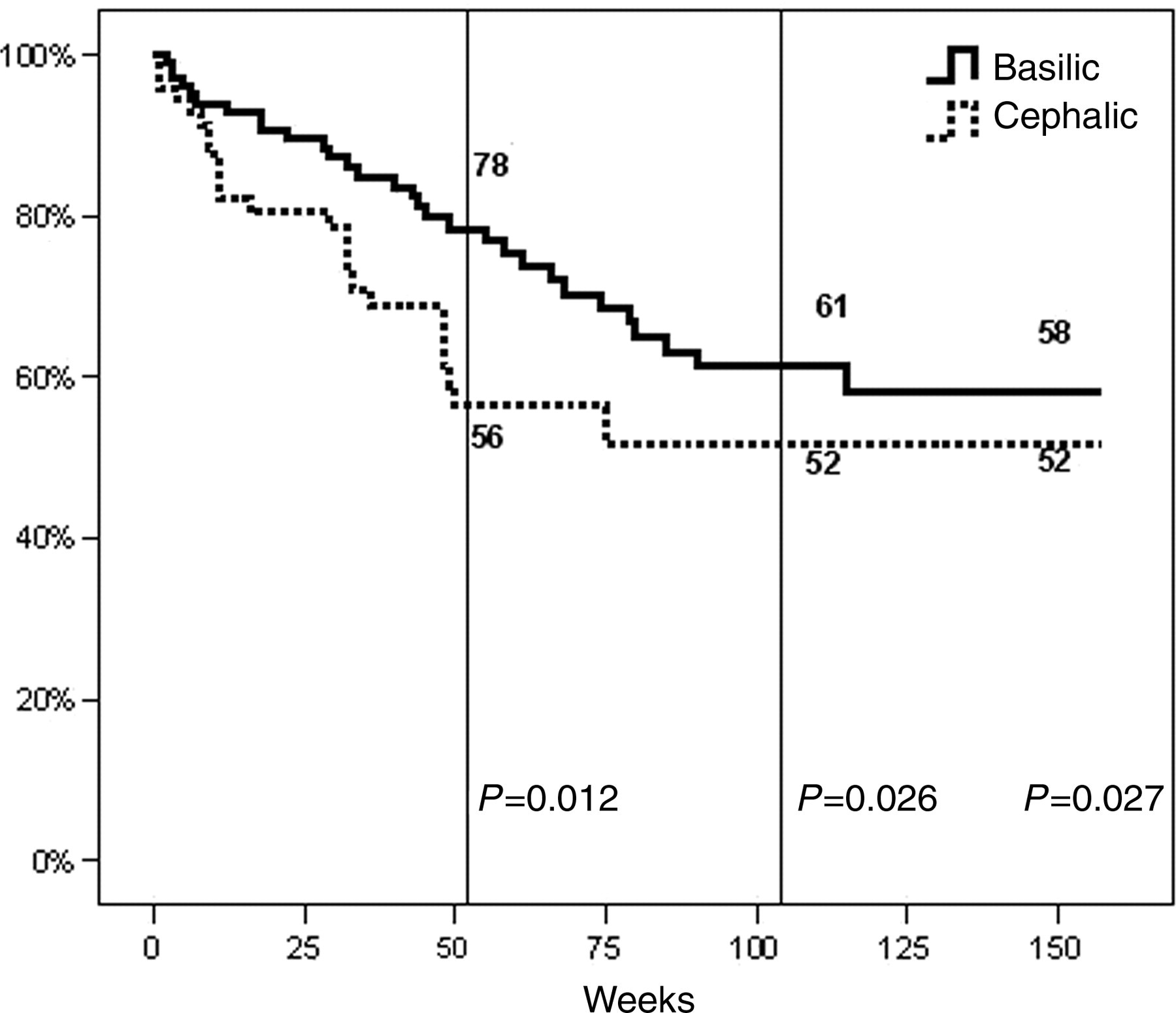
Secondary patency
It is important to note that when upper arm fistulas alone were compared, brachiobasilic (n = 99) and brachiocephalic (n = 47) showed equivalent PP, APP and SP at all time periods evaluated. PP for brachiobasilic fistulas versus brachiocephalic at one, two and three years was 61% versus 46%, 42% versus 35%, and 24% versus 35%, overall P = 0.40 (SE = 0.12 for brachiocephalic fistulas). The respective APP for brachiobasilic and brachiocephalic fistulas were 73% versus 57%, 49% versus 45% and 40% versus 45%; overall P = 0.28 (SE = 0.13 for brachiocephalic fistulas). SP for brachiobasilic and brachiocephalic fistulas were 78% versus 62%, 61% versus 51% and 58% versus 51%, P = 0.36 (SE = 0.12 for brachiocephalic fistulas) at one, two and three years.
Utilization
Basilic vein-based fistulas achieved a 77% utilization rate while only 58% of cephalic vein-based fistulas were utilized (P = 0.006). Reasons for non-utilization are listed in Table 3. Failure to mature for the cohort was 19%. The rate was significantly higher for cephalic vein-based fistulas at 28% when compared with basilic vein-based fistulas at 13% (P = 0.01). All veins utilized appeared to be of significant caliber for fistula creation. Veins of marginal size were not utilized for either cephalic or basilic vein fistulas. Excluding the patients who did not require hemodialysis and those who died or were lost to follow-up before the fistulas could be used, cumulative percent of fistulas that had been used at six months from surgery were 81% for basilic vein-based fistulas (n = 91) and 66% (n = 61) for cephalic vein-based fistulas (P = 0.60) (Figure 4). Mean time to first cannulation was not significantly different between basilic vein-based fistulas and cephalic vein-based fistulas (16 ± 13 weeks versus 17 ± 21 weeks, P = 0.6) when failure to mature and those not accessed were eliminated.
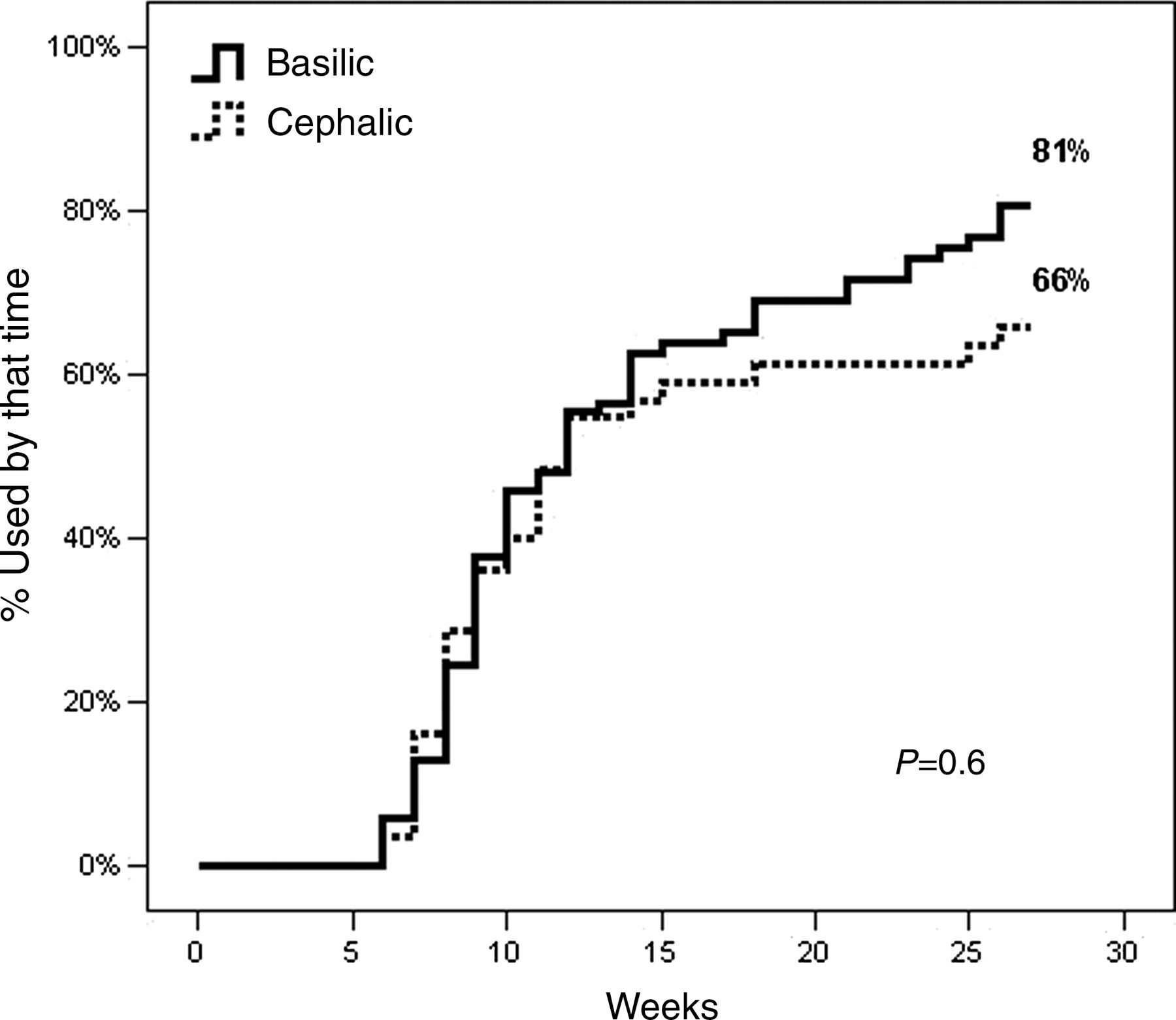
Time to use
Reasons for non-utilization
Figure 5 depicts the usage time. There was no significant difference between basilic vein-based fistulas and cephalic vein-based fistulas at one, two and three years of usage (P = 0.81). Fifty-six fistulas were lost during the follow-up. Of these, 33 were failures; 17 autogenous fistulas were lost in the first year of use and only five in the subsequent years. One autogenous fistula failed after nearly a year in a patient who did not require hemodialysis.
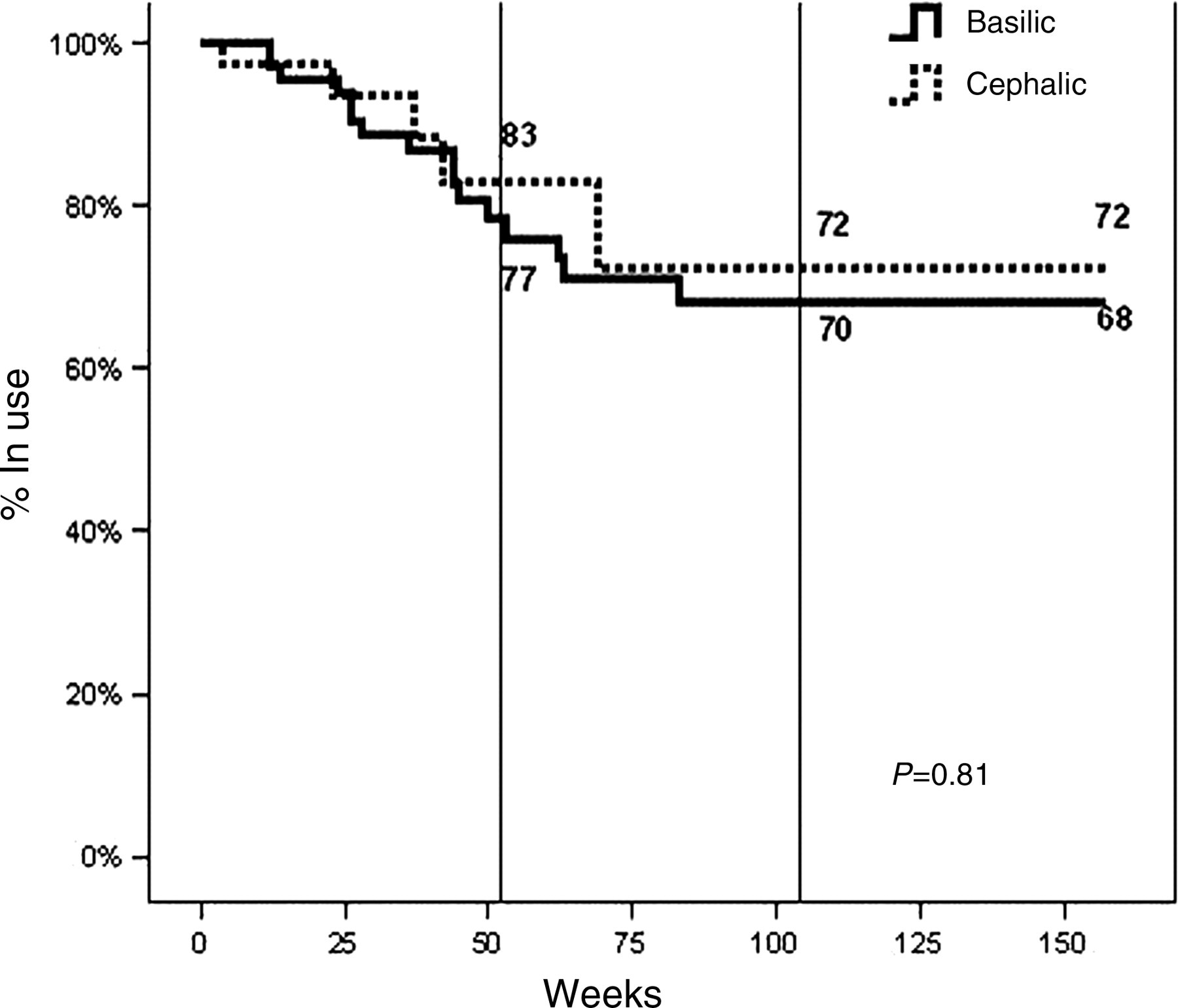
Time in use
Re-intervention
Thirty-three (33%) basilic vein-based fistulas and 12 (17%) cephalic vein-based fistulas required interventions during the follow-up period (P = 0.02), giving an overall re-intervention rate of 26%. Figure 6 illustrates the cumulative intervention-free survival of the access. Differences between PP and intervention-free patency are related to interventions for problems not associated with access patency, such as steal, pseudoaneurysms, etc. The respective re-intervention rates for basilic vein-based fistulas and cephalic vein-based fistulas were 59% versus 46% at one year and 23% versus 41% at three years (P = 0.11). When fistulas required interventions, mean time to the first procedure was 53 ± 41 weeks for basilic vein-based fistulas and 22 ± 14 weeks for cephalic vein-based fistulas (P = 0.15). Again, the time to first procedure is different slightly from PP numbers due to the need for procedures unrelated to access patency issues. The likelihood of a second intervention was 39% for basilic vein-based fistulas and 25% for cephalic vein-based fistulas (P = 0.30). The main site for the first intervention was the artery in one case each of basilic vein and cephalic vein-based fistulas (3.0% and 8.3%, respectively); anastomosis in 17 (52%) of basilic vein-based fistulas and six (50%) of cephalic vein-based fistulas; and the vein in 15 (46%) of basilic vein-based fistulas and five (42%) of cephalic vein-based fistulas.
Intervention-free patency
Table 4 tabulates the complications by fistula type. There was no statistically significant difference between the two fistula types in terms of complications.
Complications
Discussion
Hemodialysis access issues affect patient survival and quality of life. The goal of access surgery is to provide a suitable conduit with adequate flow, and good long-term patency with minimal need for additional procedures. Unfortunately, forearm veins are frequently used for intravenous access and blood draws prior to referral for access creation. K/DOQI guidelines, in an attempt to decrease the need for re-intervention and to increase access longevity, recommend a fistula first pathway for access creation. However, the guidelines place upper arm basilic vein fistulas at a level just above prosthetic grafts. When dealing with selection of permanent vascular access (Guideline 3), the DOQI guidelines of 2000 13 quote the same references as the 1997 version, 16 the latest of which was published in 1995, rather than referencing some of the newer available studies. This has been somewhat rectified in the latest guidelines. 14
In this study we compared the patency, utilization, maturation and usage rates, as well as re-intervention and complication rates, between basilic vein-based and cephalic vein-based fistulas. Our study presents a comparison of the two types of fistulas done by the same group of surgeons. Even though both brachiobasilic and brachiocephalic fistulas had superior outcomes to radiocephalic fistulas for APP and SP, we do not challenge the conventional wisdom of using the distal most suitable vein.
We found equivalent PP for brachiobasilic fistulas when compared with brachiocephalic vein fistulas. The APP and SP up to three years were also similar when comparing upper arm fistulas.
Results from brachiobasilic fistulas have varied widely between authors. The single stage basilic vein fistula is very operator-dependent, with partial torsion of the vein putting the vein at risk for failure. Wolford et al. 17 found a low rate of PP for brachiobasilic fistulas, 23% at one year and 11% at two years, with 44% of the problems secondary to stenosis within the body of the basilic vein graft, and suggests conservative use of this vein. However, they had a very aggressive policy for autogenous fistulas, utilizing veins as small as 1.7 mm in size, which may have impacted their results. Woo et al. 8 found excellent results for brachiobasilic fistulas, with 71% one-year and 52% five-year PP, similar to their cephalic vein fistulas at 56% and 40%. Papanikolaou et al. 18 also had excellent results with brachiobasilic fistulas in their review of 2422 patients; however, they had relatively few brachiobasilic fistulas as this was relegated to primarily third choice procedures, below prosthetic grafts. They found a longer patency with brachiobasilic fistulas, but do not compare these with brachiocephalic fistulas statistically. One-year PP for brachiobasilic fistulas in their series was 79% compared with 74% for brachiocephalic fistulas, with more than 50% of all brachiobasilic fistulas patent at four years. They also only performed intervention for access salvage for radiocephalic fistulas; therefore, we are unable to compare secondary and primary assisted patency with their analysis.
The lesser dissection necessary for a direct anastomosis rather than a transposition clearly makes the cephalic vein an attractive option when both veins are equivalent. Each center should carefully evaluate their patency rates when looking at vein transposition to ensure reasonable patency of the access. Our results show that brachiobasilic fistulas can be created with at least an equivalent rate of success to that of its cephalic counterpart. We believe that the better of the two veins based on clinical, imaging and intraoperative findings should be used, rather than a protocol-driven cephalic vein first approach.
Our overall patency rates were comparable to other published data for AV fistulas. 3–12,17,19–23 We were also able to achieve SP rates comparable to historical data. A recent systematic review and meta-analysis found that autogenous fistulas have significantly better PP and SP at 12 and 36 months, as well as reduced complication rates. 24 However, the Clinical Guidelines of the Society for Vascular Surgery are equivocal on the preference and sequence between forearm loop prosthetic access and upper arm autogenous access. 25
Late re-intervention rates were higher in basilic transposition fistulas, confirming findings of previous authors. 6,21 Though basilic vein-based fistulas and cephalic vein-based fistulas had no statistically significant difference in re-intervention-free patency, the trajectory of the lines cross around two years and basilic vein fistula continue to require re-intervention, while cephalic vein fistula requires more frequent intervention shortly after creation. When only fistulas requiring additional interventions were considered, the average time to first intervention was twice as long for basilic vein fistulas. Thus, if both veins are equivalent, the superficial cephalic vein is preferable, due to a more limited initial procedure, and the likelihood of better late patency. However, with marginal cephalic veins, we would recommend consideration of basilic vein fistulas in preference to use of suboptimal cephalic veins. Early failures will also be higher with cephalic vein-based than with basilic vein-based fistulas.
Some authors advocate the use of a two-stage procedure for brachiobasilic fistula creation. We do not believe that staging adversely affects the patency, but have found that with meticulous surgical care, excellent outcomes can be achieved with a single surgery. Hossny's study confirms similar patency with one-stage elevated, one-stage transposed and two-stage transposed brachiobasilic fistulas as well. 26
Early referral does increase the feasibility of autogenous access creation but also results in a proportion of fistulas that are never accessed, due to early thrombosis or improvement in renal function. This may have affected the utilization rate and the time to use. Non-utilization rates have varied between series. 6,10,27 We found a better rate of utilization for basilic vein-based fistulas in our series. This is primarily due to the higher primary failure rate for cephalic vein-based fistulas compared with basilic vein-based fistulas. Our primary failure rate of 19% is similar to reported rates which range from 0% to 38%. 5,6,11,20,22,28,29 This wide range probably reflects a difference in the definition of failure. Bender et al. 28 considered only primary thromboses, and excluded those that failed to mature. Studies based on incident hemodialysis patients identified by Medicare payment codes also may miss early access failures, due to inclusion of only those patients who were patent at 30 days after access creation. 29
There was no difference in the time to first use or maturation between the two fistulas. Balloon maturation techniques were not used in this study population. Usage time was also the same for basilic vein fistulas and cephalic vein fistulas. Most fistula loss occurred in the period before use or during the first year. This suggests that the basilic vein is resilient enough to withstand repeated puncture for long periods. Functional patency as defined by the reporting guidelines requires quantitative measurements of fistula flow rates and was not possible to elucidate in this retrospective study. Therefore we adopted the term usage time.
We did not find any difference between the two types of fistulas for any complications. Our rates of thrombosis are in the range found in the literature of 6–32%. 4,10,12,19,22,30 Thrombosis rates will depend on duration of follow-up.
Shortcomings
This was a retrospective, non-randomized study, so the results may reflect surgeon bias and the groups may not be entirely comparable, as is the case in all retrospective reviews. However, co-morbidities were similar between groups. The vein mapping was done in different laboratories and with different protocols. Therefore it was not possible to obtain reliable comparable data on the sizes of veins.
Conclusions
The results of this study showed that basilic vein-based fistulas have significantly lower primary failure rates and equivalent patency rates to cephalic vein-based fistulas, although they require significantly more interventions at a later stage. However, upper arm cephalic and basilic vein fistulas were found to have equivalent patency rates. There is no difference in the maturation time, usage time or complication rates between basilic and cephalic vein-based fistulas. We believe that the transposed brachiobasilic fistula should be recognized as a primary access option when a radiocephalic or other forearm fistula is not feasible, and the basilic vein is superior in quality to the cephalic vein at the antecubital fossa.
Footnotes
Acknowledgments
Financial disclosure of authors and reviewers: none reported.