
Abstract
The aim of this study was to evaluate middle-term clinical results of robot-assisted laparoscopic surgery (RALS) to treat aortoiliac occlusive disease (AIOD). Between 2002 and 2007, 28 consecutive patients received robot-assisted laparoscopic aortobifemoral bypass grafting (n = 24) or aortoiliac endarterectomy (n = 4). Patients were followed prospectively. RALS could be completed successfully in 24 patients; conversion to open surgery was necessary in four patients (14%). Median operative time was 350 min. Median aortic clamping time was 70 min. Median hospital stay was five days. One patient died within 30 days. Non-lethal complications occurred in four patients (14%). Clinical symptoms improved in all patients. Primary and secondary limb-based patencies at 36 months were 89% and 91%, respectively. In conclusion, RALS is a feasible and durable technique for patients with AIOD. Although operative times are long, RALS allows rapid postoperative recovery.
Introduction
Aortoiliac occlusive disease (AIOD) causing claudication or critical ischemia can be treated by either endovascular or conventional surgical techniques. According to the second TransAtlantic Inter-Society Consensus (TASC), surgery is the gold standard for the treatment of extensive AIOD. 1 Open aortoiliac reconstructive surgery provides a durable solution with a modest mortality risk, but with significant perioperative morbidity. 2–4 Laparoscopic aortic surgery has been developed to reduce operative trauma and to facilitate quicker ambulation. 5–11 Performing a vascular anastomosis using laparoscopic techniques is challenging, however, and successful performance of laparoscopic aortic surgery requires dedication and vast amounts of training. 7,8 Robot technology may help to overcome some of the limitations of traditional laparoscopic instruments, thus shortening the learning curve. 12 The robotic system eliminates tremor from the surgeon's hands, provides instruments with additional degrees of freedom, produces motion scaling and provides perfect three-dimensional visualization, thereby enhancing the precision of the surgery. A few authors have reported the feasibility of robot-assisted laparoscopic aortoiliac surgery, with short-term results comparable with ‘conventional’ laparoscopic techniques. 13–15 Reports on mid- and long-term results of laparoscopic and robot-assisted aortic surgery, however, are scarce. The purpose of this study was to evaluate our clinical experience and mid-term results of robot-assisted laparoscopic surgery (RALS) for AIOD.
Methods
RALS for AIOD has been performed at the VU University Medical Center since 2002, using the Zeus-Aesop (Computer Motion, Santa Barbara, CA, USA) and da Vinci robotic systems (Intuitive Surgical Inc, Sunnyvale, CA, USA). All operations were performed by the same surgical team, consisting of a vascular surgeon (WW) and a laparoscopic surgeon (MAC). A thorough preparation program was set up including multiple cadaver and animal studies before performing RALS. After first using a transabdominal approach with the apron technique 16 and a retroperitoneal approach, 17 a transabdominal approach with extreme patient-rotation as described by Diks et al. 12 and Coggia et al. 18 has been adopted. In short, after the exposition of both common femoral arteries the patient's abdomen is rotated 90° to the right using maximum rotation of the operating table and inflation of a pillow (Pelvic-Tilt; OR Comfort, LLC, Branchburg, NJ, USA) below the left flank. The surgeon stands at the right side of the patient, and after installation of a pneumoperitoneum, six 12-mm trocars are inserted. Using standard laparoscopic techniques, the left colon is dissected and together with the small bowel moved to the right. The aorta is exposed from the left renal vein to the level of the iliac bifurcation. For aortobifemoral bypass grafting, a bifurcated polytetrafluoroethylene (PTFE) (W L Gore and Associates, Flagstaff, AZ, USA) prosthesis is inserted into the abdomen. The graft limbs are tunneled to the groins, after which the da Vinci robotic system is installed into the operative field from the left side of the patient (see Figure 1 for operating room set-up). Using two robotic needle drivers (Endowrist Needle Drivers; Intuitive Surgical) an end-to-side anastomosis is made. Shortened CV-4 PTFE (W L Gore and Associates) stitches – previously knotted on felt pledgets – are used to perform two hemicircumferential running sutures and are tied intracorporally. Clamps are placed on the graft limbs in the groins and after unclamping the aorta the patient is returned to the dorsal decubitus position. Conventional end-to-side anastomoses are performed to the common femoral arteries. For aortoiliac endarterectomy, pots scissors and a robotic needle driver (Endowrist Pots Scissors, Endowrist Needle Drivers) are used to perform a thromboendarterectomy. The aorta and iliac arteries are subsequently closed with a CV-4 PTFE running suture without the use of a patch. Final inspection is performed to ensure hemostasis and viability of the left colon.
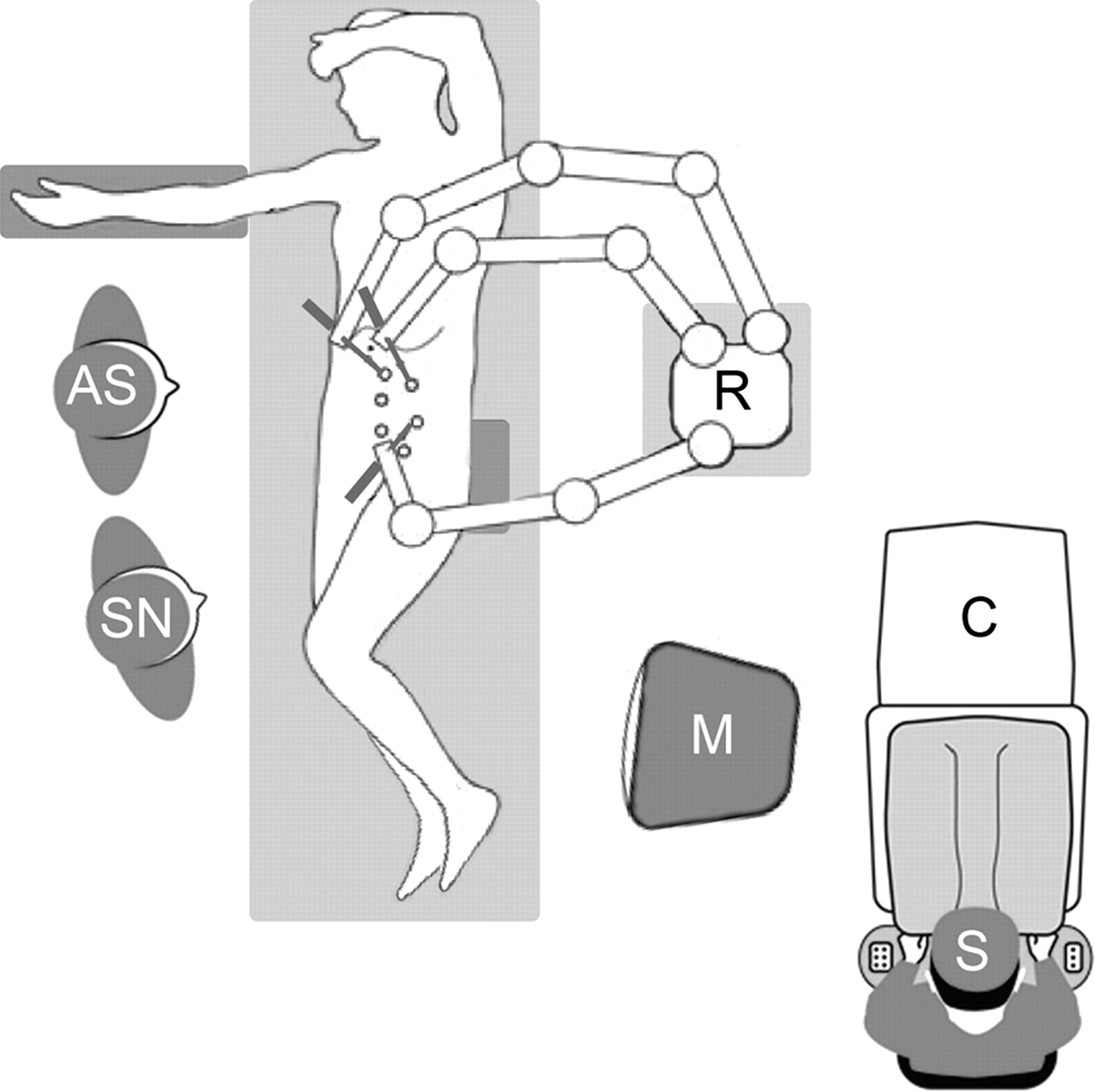
Set-up in the operating room. R, robotic cart; C, robotic console; M, monitor; S, surgeon; AS, assistant surgeon; SN, scrub nurse
Preoperative patient examinations included ankle-brachial index test, duplex scanning of the aorta and lower limbs, and computed tomography angiography or magnetic resonance angiography (MRA). Aortoiliac occlusive lesions were classified according to the TASC score. 1 Patients were preferably treated by means of endovascular techniques. Aortoiliac reconstructive surgery was reserved for patients deemed unsuitable for endovascular therapy or after unsuccessful endovascular therapy. All patients underwent preoperative cardiac and pulmonary evaluation. Co-morbid factors were classified in accordance with the American Society of Anesthesiologist (ASA) classification. Contraindications for robot-assisted surgery were ASA class V and significantly abnormal cardiac, hepatic and renal test results. Patients with extensive renal or visceral occlusive disease requiring suprarenal aortic cross clamping were excluded. Extensive aortoiliac calcification was not a contraindication for RALS. Mortality was defined as in-hospital or within 30 days following surgery.
Patient follow-up consisted of physical examination, duplex scanning and ankle-brachial index tests at two, six and 12 months, and yearly thereafter. Aortic clamping time represents the time from clamping the aorta to moving the clamps to the graft limbs after completion of the aortic anastomosis. Data obtained at follow-up included graft patency, presence of false aneurysms, walking distance and occurrence of adverse events, including incisional hernias. According to criteria postulated by Rutherford et al., 19 patency needed to be demonstrated by either vascular imaging (duplex scanning) or direct observation during re-operation. All data were collected prospectively. Prior to surgery, patient informed consent and approval from our institution's Ethical commission were received.
Limb-based primary and secondary patencies were summarized using Kaplan–Meier estimates. Estimates of patencies are shown at three years. Analysis was performed using SPSS 14.0.
Results
Between February 2002 and April 2007, 28 consecutive patients underwent RALS for AIOD at our institution. From February 2002 until February 2003, the first five patients received an aortobifemoral bypass using the Zeus-Aesop robotic system, which was on a temporary loan. From January 2004, patients were treated using the da Vinci robotic system. A total of 24 patients were treated by means of robot-assisted laparoscopic aortobifemoral bypass grafting (TASC C and D lesions). In two patients, a femoropopliteal bypass was performed during the same session. From November 2005, we also performed robot-assisted laparoscopic aortoiliac endarterectomies in four patients (TASC B and C lesions) after endovascular repair had failed or re-led to recurrence in relatively young patients. During the whole period, 45 surgical procedures were performed for AIOD. Fourteen patients received conventional open aortobifemoral bypasses for occlusive disease. Reasons for open surgery were severe ischemic rest pain or acute ischemia, requiring immediate surgery (n = 3), renal or visceral occlusive disease requiring suprarenal aortic cross clamping (n = 6), prior extensive abdominal surgery (n = 3) and redo surgery because of occluded prosthesis (n = 2). Three patients received open aortoiliac endarterectomy before we performed this procedure using RALS. Between February 2002 and April 2007, endovascular treatment of AIOD was performed in 223 patients. Eight patients received an axillofemoral bypass during this time interval, because of an infected aortic bypass (n = 4), infected aortic endoprosthesis or because of severe ischemic rest pain or acute ischemia, requiring immediate surgery in patients with extensive co-morbidities (n = 3).
The patient group consisted of 20 men and eight women, with a median age of 57 years (range 36–73). Detailed patient characteristics are described in Table 1. All patients suffered from invalidating intermittent claudication, rest pain or ulcers (Fontaine classification 2b or higher, Rutherford category 3 or higher). Median ankle-brachial index in rest was 0.50 (range 0.17–0.80). Revascularization with percutaneous transluminal angioplasty was previously attempted in 23 patients, including stent placement in 16 patients. A femorofemoral bypass had been performed previously in one patient. Aortoiliac lesions were classified TASC type B in three cases, type C in 12 cases and type D in 13 cases. Previous abdominal surgery was performed in three patients.
Patient demographics
TASC, TransAtlantic Inter-Society Consensus; BMI, body mass index; ASA, American Society of Anesthesiologist
RALS was feasible in 24 patients (86%). In four patients (14%), conversion to mini or full laparotomy was required. Three of these cases have been described previously. 11 Reasons for conversion were bleeding from a previously clipped lumbar artery, battery failure of the robotic system and continuous CO2 leakage from the pneumoretroperitoneum, causing the small bowel to migrate into the operative field, thus obstructing vision. The fourth conversion was required when during laparoscopic dissection no progression could be made because of extensive abdominal adhesions due to prior abdominal surgery.
One patient (3.6%) died on the third postoperative day due to a massive myocardial infarction, following normal early postoperative recovery from an uneventful robot-assisted laparoscopic aortobifemoral bypass. Postoperative non-lethal complications occurred in four patients (14%) (see Table 2). One patient had to undergo reoperation on the first postoperative day, due to bleeding from the prosthesis. A small puncture hole was found that had probably occurred during manipulation of the graft with the robotic system. A second patient required thrombectomy of both common femoral arteries on postoperative day 1 after aortoiliac endarterectomy because of thrombosis. One patient developed acute respiratory distress syndrome and pyelonephritis requiring prolonged respiratory support and temporary dialysis following conversion to open surgery due to severe bleeding. One patient developed a urinary tract infection that was successfully treated by oral antibiotics. Clinical symptoms improved in all patients. Median ankle-brachial index increased to 1.0 (range 0.57–1.15).
Early and late complications of robot-assisted laparoscopic surgery
The median operating time was 350 min (range 225–589), with a median clamp time of 70 min (range 25–205). Median clamping time was 65 min (range 25–205) for aortobifemoral bypass and 113 min (range 58–218) for aortoiliac endarterectomy. Median set-up time for the robotic system was nine minutes (range 6–14). Median blood loss was 1125 mL (range 100–5800), median intensive care unit stay was one day (range 1–16) and median hospital stay was five days (range 3–57). Patients resumed normal diet at a median of two days after surgery (range 2–14) and resumed ambulation at a median of two days (range 1–20) (see Table 3).
Operative and postoperative data
ICU, intensive care unit
Follow-up results for robot-assisted laparoscopic aortoiliac reconstructive surgery were retrieved for 27 patients. All except three patients were asymptomatic at the time of first follow-up visit. Three symptomatic patients had mild claudication (Rutherford class 1) and had improved at least two points on the Rutherford scale. Median follow-up was 36 months (range 12–68). Primary limb-based cumulative patency at 36 months was 89 ± 0.5%; secondary limb-based cumulative patency at 36 months was 91 ± 0.5% (see Figures 2 and 3).
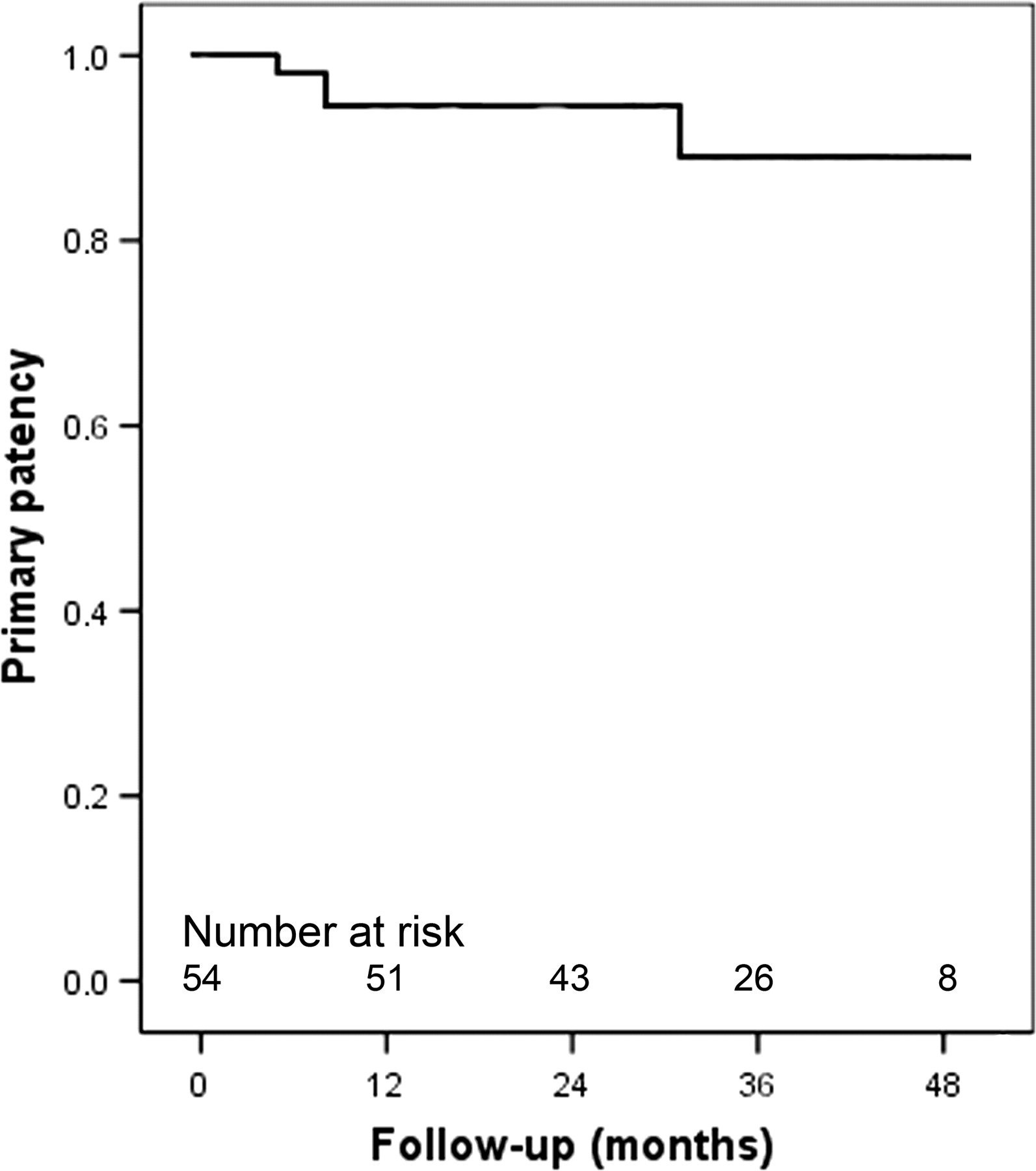
Kaplan–Meier curve estimates for primary cumulative limb-based patency for robot-assisted laparoscopic aortoiliac reconstructive surgery
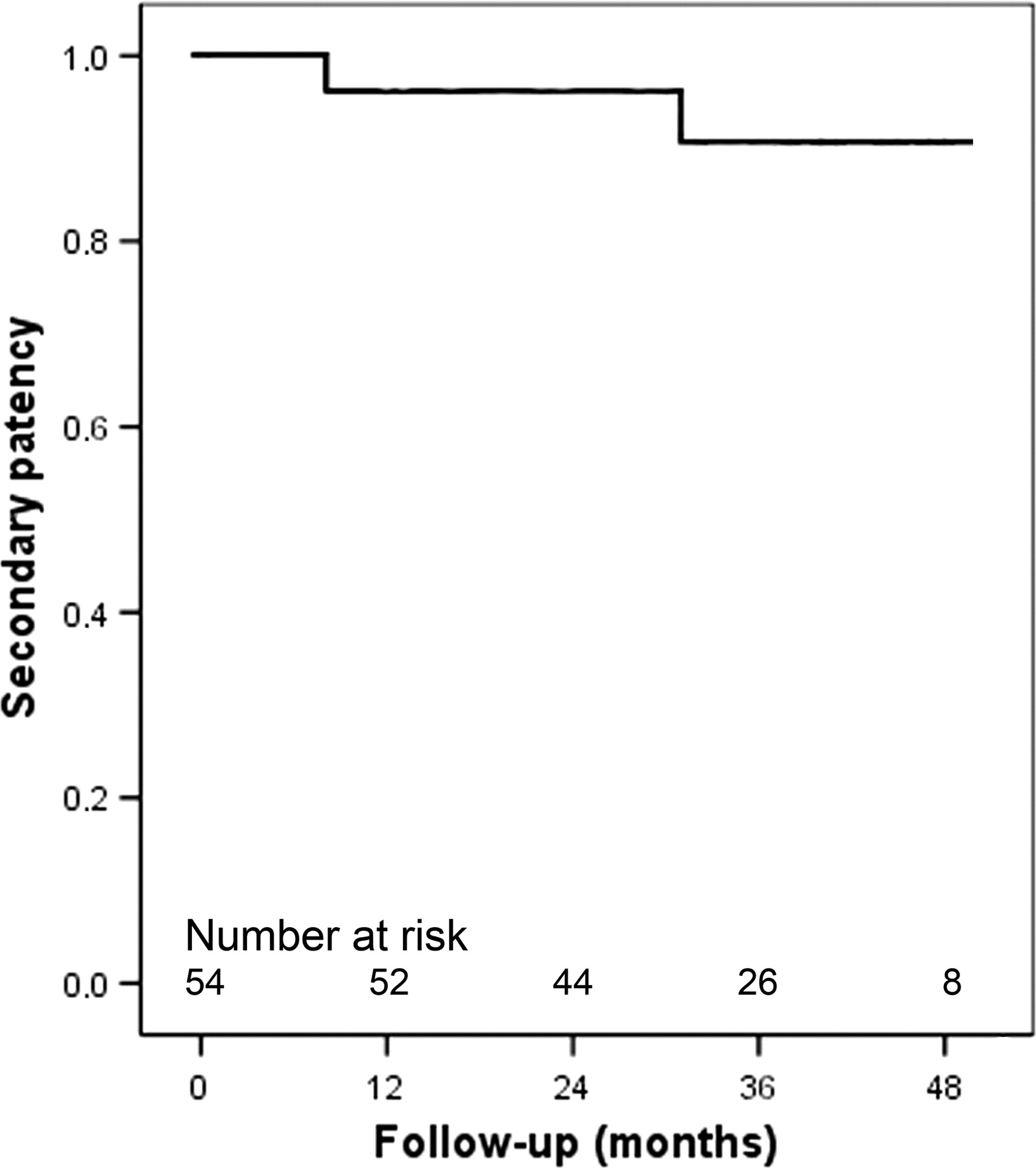
Kaplan–Meier curve estimates for secondary cumulative limb-based patency for robot-assisted laparoscopic aortoiliac reconstructive surgery
Four patients suffered late complications (15%) (Table 2). Bleeding from a false aneurysm of the left distal anastomosis five months after aortobifemoral bypass grafting required revision in one patient. Postoperatively, a fistula persisted in the left groin. Thrombosis of the left graft limb five months later was treated by revision of the graft limb and a simultaneous sartorius myoplasty. The patient was treated with oral antibiotics for eight weeks, after which she fully recovered. In one patient, a prosthetic femoropopliteal bypass was performed four months after aortobifemoral bypass grafting because of progressive arterial occlusive disease. Infection of the femoropopliteal prosthesis required revision after four months. Two weeks later, partial occlusion of the aortobifemoral bypass required revision. After a third femoropopliteal bypass and a consecutive thrombectomy of the superficial femoral artery, a below-the-knee amputation was inevitable. Extensive analysis by our vascular medicine department did not reveal any risk factors for the patient's extensive occlusive disease other than tobacco use, which was stopped prior to surgery, and hypertension, which was well regulated with antihypertensive medication. Patency was lost in a third patient after 31 months of follow-up, because of thrombosis inside the aortobifemoral prosthesis. Retrograde thrombectomy from the groin proved unsuccessful; therefore, revision of the prosthesis was performed through a conventional midline laparotomy. One incisional hernia occurred in a patient after conversion to a retroperitoneal approach. One patient died during follow-up because of non-small-cell lung carcinoma after 55 months of follow-up.
Discussion
Since the first laparoscopic aortic procedure by Dion et al., 20 laparoscopy-assisted, totally laparoscopic and robot-assisted procedures have been developed for both occlusive and aneurysmal disease of the aorta and iliac arteries. Although operative times are long, benefits to the patients in terms of decreased postoperative pain and earlier return to daily routines have been described. 21,22
In our group of 28 patients treated with RALS for AIOD, postoperative recovery was quick, with mortality and morbidity comparable with open surgery. Mid-term follow-up results were satisfactory, indicating the durability of RALS for AIOD. Comparable follow-up results have been reported after open surgery. Five-year primary and secondary patencies have been reported to be 85–91% and 93%, respectively. 2,4 Follow-up results after laparoscopic surgery for AIOD have been reported in two studies. After a mean follow-up of 25.2 ± 17.6 months, Di Centa et al. 23 reported three-year primary and secondary cumulative patency rates of 93% and 95.6%, respectively. Dion et al. 5 reported graft limb thrombosis in one patient (3.9%) after a mean follow-up of 31.6 months.
The da Vinci robotic system provides the surgeon with several advantages over traditional laparoscopy, facilitating complex laparoscopic procedures, such as performing an aortic anastomosis. 24 In our clinical experience robotic assistance proved helpful not only in creating the aortic anastomosis but also in controlling lumbar back bleeding and in performing extensive aortic endarterectomy. As a result, aortic clamping times were reduced considerably after the first patients, even without a weekly or monthly routine. 12
A disadvantage of laparoscopic surgery in general and laparoscopic aortic surgery in particular is the long operative times required. Reported total operative and aortic clamping times are shown in Table 4. Although robotic technology shortened the learning curve with regard to creation of the aortic anastomosis and thereby aortic clamping time, total operative times were considerable in our series. The greater part of the procedure consists of the laparoscopic dissection of the abdominal aorta, which is a challenging and time-consuming technique. Robotic assistance was not used for dissection of the aorta, because it does not involve complex laparoscopic maneuvers and standard laparoscopic instruments offer more flexibility during dissection of the left colon. Three different techniques have been used for this procedure. The apron technique, in which intrusion of bowel in the operative field is prevented by the use of an apron peritoneal layer, proved to be a tedious and time-consuming technique. The retroperitoneal approach offered a small operative space that collapsed easily with suction or CO2 leakage. The transabdominal route with extreme patient rotation offers a clear and stable field but laparoscopic dissection of the aorta is more challenging. In part because of our search towards the optimal surgical approach, we are yet to complete our learning curve for this part of the procedure before total operative times can be reduced. The modified transperitoneal approach described by Stadler et al. 15 may be a valuable alternative and deserves further investigation. This approach requires only minor changes in patient position during the operation and does not involve mobilization of the descending colon. Furthermore, the robotic system can be placed on the right side of the patient, thereby optimizing camera and instrument angles and avoiding interference with the shoulder and head of the patient.
Operative and aortic cross clamp times for (robot-assisted) laparoscopic aortic surgery
Conversion to open surgery was necessary in four patients. In one patient the battery of the robotic system was not recharged and it was considered unsafe to proceed without a backup energy source. A second conversion was required because of continuous CO2 leakage from the pneumoretroperitoneum causing loss of visibility using the retroperitoneal approach. Both conversions can be considered as part of our learning curve and can be avoided in future patients.
According to multidisciplinary guidelines, surgery is the preferred treatment for extensive AIOD (TASC C and D). 1 However, ongoing developments in endovascular technique have led to successful endovascular treatment of extensive AIOD (TASC C and D lesions) in some centers. 25,26 Although mid-term results (primary patency 69–74%; secondary patency 89–95% after 3 and 4 years) cannot yet compete with results obtained after surgery, re-interventions can often be performed percutaneously. At our center we prefer to treat patients by means of endovascular techniques, reserving surgery for patients unsuited for or after failed endovascular therapy. In these cases, RALS provides a minimal invasive alternative for open surgery while maintaining long-term durability.
Although RALS may be used for abdominal aortic aneurysm (AAA) repair as is shown by Stadler et al., 15 in our center, with a long endovascular tradition, we prefer endovascular AAA repair over open or robot-assisted surgery. Complex aneurysms (e.g. juxta- or suprarenal AAA) that are relatively unsuitable for endovascular repair, in our opinion, are currently not amenable for RALS and receive open repair.
Care has to be taken to avoid collision between the robotic arms and laparoscopic instruments. A potential complication is avulsion of the aortic clamp by collision with the robotic arms. Communication between the assistant surgeon at the table and the surgeon behind the console is of utmost importance. Quick, sudden moves of the instruments should be avoided. Furthermore, correct trocar positioning with enough space between robotic and laparoscopic instruments is important.
Despite several advantages over laparoscopic aortic surgery, RALS has not yet been performed by many vascular surgeons. Several hurdles may prevent the widespread use of RALS. Even with robotic assistance, laparoscopic aortic surgery remains technically demanding and requires practice and devotion before it can be implemented successfully. Training of surgeons with robotic and laparoscopic instruments and sutures is essential to reduce total operative and clamping times. The robotic system does not provide haptic feedback; therefore, care has to be taken in handling body tissue, sutures and prosthetic material. To assist during robotic surgery and to perform rapid conversion when necessary, two senior surgeons are required during RALS. Furthermore, costs for the robotic system, service contract and instruments have to be taken into account. However, many modern hospitals have already adopted robotic systems based on advantages in other fields of surgery, such as cardiac, gynecologic and urologic surgery, making robotic systems available to vascular surgeons. 27–29 The main obstacle for the widespread performance of RALS seems to be the limited number of patients amenable for this technique. Thanks to ongoing developments in endovascular surgery for both dilating and occlusive disease of the aorta and iliac arteries, only a minority of the patients will require surgery. These include patients with complex lesions (e.g. suprarenal disease), currently not suited for RALS. Despite this, surgical robots are still being developed and will become smaller, less expensive and more manageable in the future. Together with growing evidence concerning its efficacy, safety and durability and the ongoing demand for minimally invasive surgical techniques, this will potentially lead to a growing number of patients receiving robot-assisted laparoscopic aortic procedures.
Our results suggest that RALS is a feasible and durable technique for patients with AIOD. Robot-assisted laparoscopic aortic surgery potentially combines the advantages of minimal invasive surgery with the durability of open aortoiliac reconstructive surgery.
Footnotes
Acknowledgments
There are no contributions that need to be acknowledged. The authors did not receive any form of financial or material support for this work. None of the authors has any conflict of interest.