
Abstract
The purpose of this study is to compare infection, pseudoaneurysm formation and patency rates during long-term follow-up of polyurethane and polytetrafluoroethylene (PTFE) vascular access grafts maintained with contemporary endovascular methods. During a 34-month period, 239 polyurethane and 125 carbon-impregnated PTFE vascular access grafts were placed in 324 consecutive patients. Thirty-six patients (9.9%) developed a pseudoaneurysm (anastomotic, n = 6 or at the needle-stick site, n = 30). An additional 19 patients (5.2%) required graft excision for infection. Three-year graft infection and pseudoaneurysm formation (at needle-stick site) rates were similar in polyurethane and PTFE grafts (11% versus 8%, P = 0.61, and 17% versus 23%, P = 0.72, respectively). Three-year secondary patency was better in polyurethane than PTFE grafts (69% versus 57%, respectively, P = 0.012). Straight upper arm polyurethane grafts had the best secondary patency (P = 0.001). Contemporary long-term secondary patency of vascular access grafts is satisfactory. Further follow-up is necessary to compare late infection and pseudoaneurysm formation rates.
Introduction
Although prosthetic vascular access grafts are the second access of choice following native fistulas, a significant proportion of patients who lack superficial veins suitable to create a fistula rely on the former to receive renal replacement treatment. Compared with native fistulas, primary patency of prosthetic grafts is inferior; however, graft patency is increased with routine graft surveillance using clinical and hemodynamic parameters, 1–3 and aggressive management, so that prolonged long-term secondary patency can be achieved. 4–6 As a result of improved graft longevity, long-term complications, including infection and pseudoaneurysm formation, are more likely to develop before graft abandonment; however, available information on this subject is limited, particularly for the most recently introduced graft types. Our group has reported on a polyurethane vascular access graft with self-sealing properties, specially designed to provide early access and rapid hemostasis (Vectra® Vascular Access Graft, C R Bard, Inc, Murray Hill, NJ, USA), which, however, might be susceptible to infection according to a recent study. 7 On the other hand, it is likely that polyurethane grafts develop pseudoaneurysms less frequently, because of their unique wall characteristics.
The aim of the present study was to compare infection, pseudoaneurysm formation (anastomotic and at the needle-stick site) and patency rates (using an aggressive graft surveillance and endovascular treatment protocol) during long-term follow-up of polyurethane vascular access grafts (Vectra® Vascular Access Graft) and polytetrafluoroethylene (PTFE) carbon-impregnated IMPRA® Carboflo® Vascular Grafts (C R Bard, Inc).
Material and methods
During a 34-month period (between March 2004 and December 2006 inclusive), 239 polyurethane Vectra Vascular Access Grafts (C R Bard, Inc) and 125 PTFE carbon-impregnated IMPRA Carboflo Vascular Grafts (C R Bard, Inc) were placed in 324 consecutive patients, 167 women and 157 men. The graft-type implanted was an individual surgeon's preference in this case-controlled prospective study. The median (interquartile range) age was 63 (53–75) years. There were 96 forearm, 261 upper arm (configuration: straight, n = 244 or loop, n = 17) and seven thigh loop grafts. The left arm was selected in most cases (n = 245, 67%), the right one (n = 119) being a second choice when the left (non-dominant side for the majority of patients) arm and forearm had been used. The patient demographics in relation to each study group are summarized in Table 1. All patients received one dose of cefazolin (1 g intravenous) preoperatively or in the case of allergy to penicillin, clindamycin (600 mg intravenous) or vancomycin (500 mg or 1 g, intravenous, depending on body weight).
Demographics of the two study groups (Vectra and PTFE grafts)
PTFE, polytetrafluoroethylene; IQR, interquartile range
Description of graft material, surveillance, monitoring and endovascular treatment protocol
Vectra® Vascular Access Graft is a tri-layered graft, composed of Thoralon®, a proprietary blend of segmented polyetherurethaneurea and a siloxane containing a surface-modifying additive. Vectra has self-sealing properties allowing early cannulation because its solid middle layer has self-sealing graft properties. The PTFE carbon-impregnated IMPRA Carboflo Vascular Graft is made from modified ePTFE material. Carbon particles are permanently integrated into the ePTFE material and are uniformly distributed through 25% of the wall. Animal studies have demonstrated that compared with standard PTFE grafts, carbon lining significantly decreases platelet accumulation, 8 and deposition by a factor of six. 9
Graft surveillance and monitoring was performed by using clinical and hemodialysis criteria, respectively, to detect a failing/failed graft. 3 Endovascular treatment was performed as an outpatient procedure, as previously described. 1,3 Rheolytic thrombectomy using the AngioJet device (Possis Medical Inc, Minneapolis, MN, USA) and a specially designed catheter (AVX or DVX) was performed for graft occlusion followed by angioplasty (±stenting) of the anatomical lesion (arterial anastomosis, graft, venous outflow, draining or central veins) responsible for the thrombotic event. 8,9 Isolated angioplasty (±stenting) of the anatomical lesion (arterial anastomotis, intragraft, venous outflow, draining or central veins) was performed for failing grafts.
All patients were followed up to the end of secondary patency (final thrombotic event), graft removal (because of infection) or ligation (for steal syndrome or venous hypertension) or death. The study was approved by the hospital IRB. All grafts had a minimum follow-up of 15 months.
Outcome definition
Graft patency was defined according to the Reporting Standards for Arterio-Venous Accesses of the Society for Vascular Surgery and the American Association for Vascular Surgery. 10 Graft pseudoaneurysm (infected or non-infected) was defined as a vascular abnormality that resembles an aneurysm, but the outpouching is not limited by a true vessel wall, rather by external fibrous tissue. 11 Mechanical or infectious anastomotic pseudoaneurysms were distinguished from mid-graft pseudoaneurysms at the needle-stick site. 10 Diagnosis was made on physical examination and usually confirmed by angiogram or occasionally by ultrasound. Graft infection was defined as soft-tissue infection along the path of the graft due to involvement of the prosthetic material, including cases of skin erosion and graft exposure.
Statistics
All data were entered into a Microsoft Office Access database (Microsoft Inc, Redmond, WA, USA) and analyzed with SPSS 14.0 for Windows (SPSS Inc, Chicago, IL, USA).
Graft patency rates were calculated with the Kaplan–Meier method and compared with the log-rank (Mantel–Cox) test. Multivariate analysis of the effect of clinical parameters on patency rates was performed with the Cox regression method (Forward and Backward Wald models). Categorical data were analyzed with the chi-square or Fisher's exact test where appropriate.
Results
Twenty-nine grafts developed early postoperative complications including non-salvageable perioperative thrombosis in 19 (5.2%) patients and venous hypertension, steal syndrome or infection in the remaining 10 (2.7%) patients necessitating graft ligation or removal. Five additional patients (1.4%) moved out of the area or died, before graft use. Finally, 330 grafts (90.7%) were released for use. A flow chart of patients entered into the study is shown in Figure 1. The usage rate of Vectra grafts (94%) was higher than PTFE grafts (84%, P = 0.002, odds ratio 3.1).
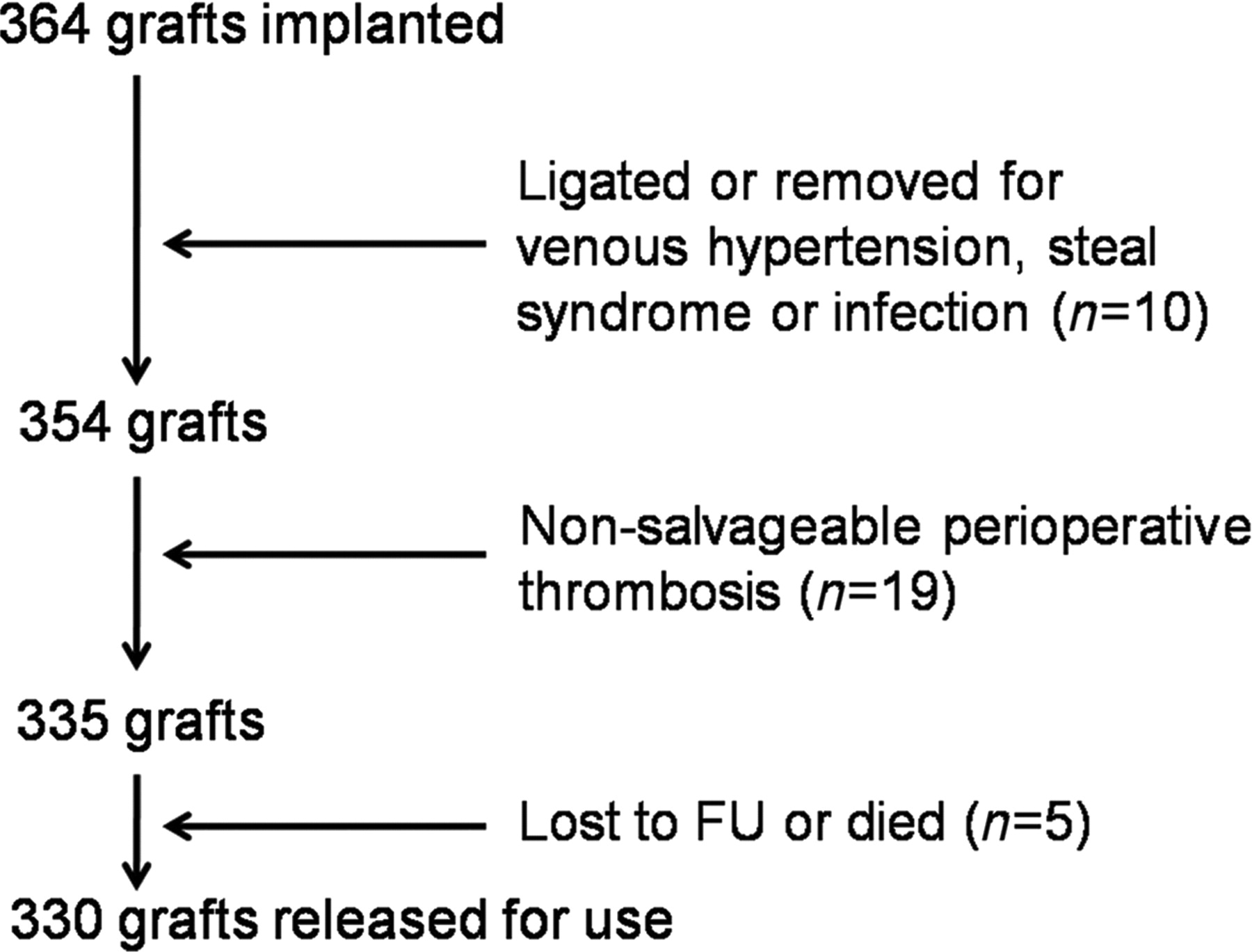
Flow chart of patients entered into the study
During follow-up, 36 patients (9.9%) developed a pseudoaneurysm, either anastomotic (1.6%: infected, n = 4, non-infected, n = 2) or at the needle-stick site (7.1%: infected, n = 4, non-infected, n = 26). An example of the latter type is shown in Figure 2. Nineteen additional patients (5.2%) developed graft infection requiring excision. Infected graft salvage was possible only in two patients (7%). Cumulative graft infection and pseudoaneurysm formation (at needle-stick site) rates at three years were not significantly different between Vectra and PTFE Carboflo grafts (11% versus 8%, P = 0.61, Figure 3 and 17% versus 23%, P = 0.72, Figure 4, respectively); only two infected grafts could be salvaged. Both non-infected anastomotic aneurysms were surgically managed; one of them required graft ligation following unsuccessful management with a stent graft, while the second one was salvaged. Non-infected pseudoaneurysms at the needle-stick site (n = 26) were mostly managed conservatively. In five cases (three Vectra and two PTFE Carboflo grafts), a stent graft (Fluency, C R Bard, Inc) was placed. One of them was complicated by endoleak treated with placement of an additional stent graft, both removed later because of infection. Another one was complicated by early occlusion. One pseudoaneurysm was seen in association with occlusion of the graft that was abandoned. The remaining 20 pseudoaneurysms were managed expectantly.
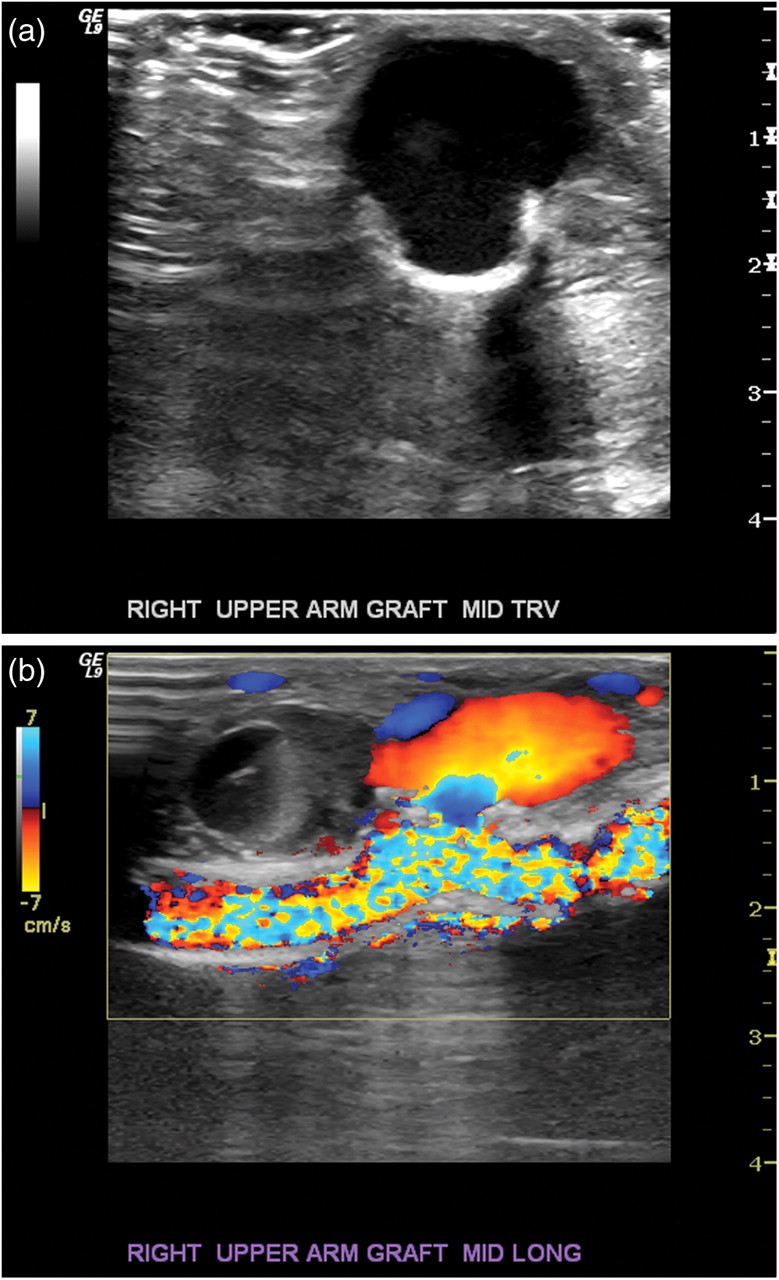
Sonogram of a pseudoaneurysm (at the needle-stick side) of a Vectra graft in transverse section and B-mode testing (a) and longitudinal section and color duplex (b)
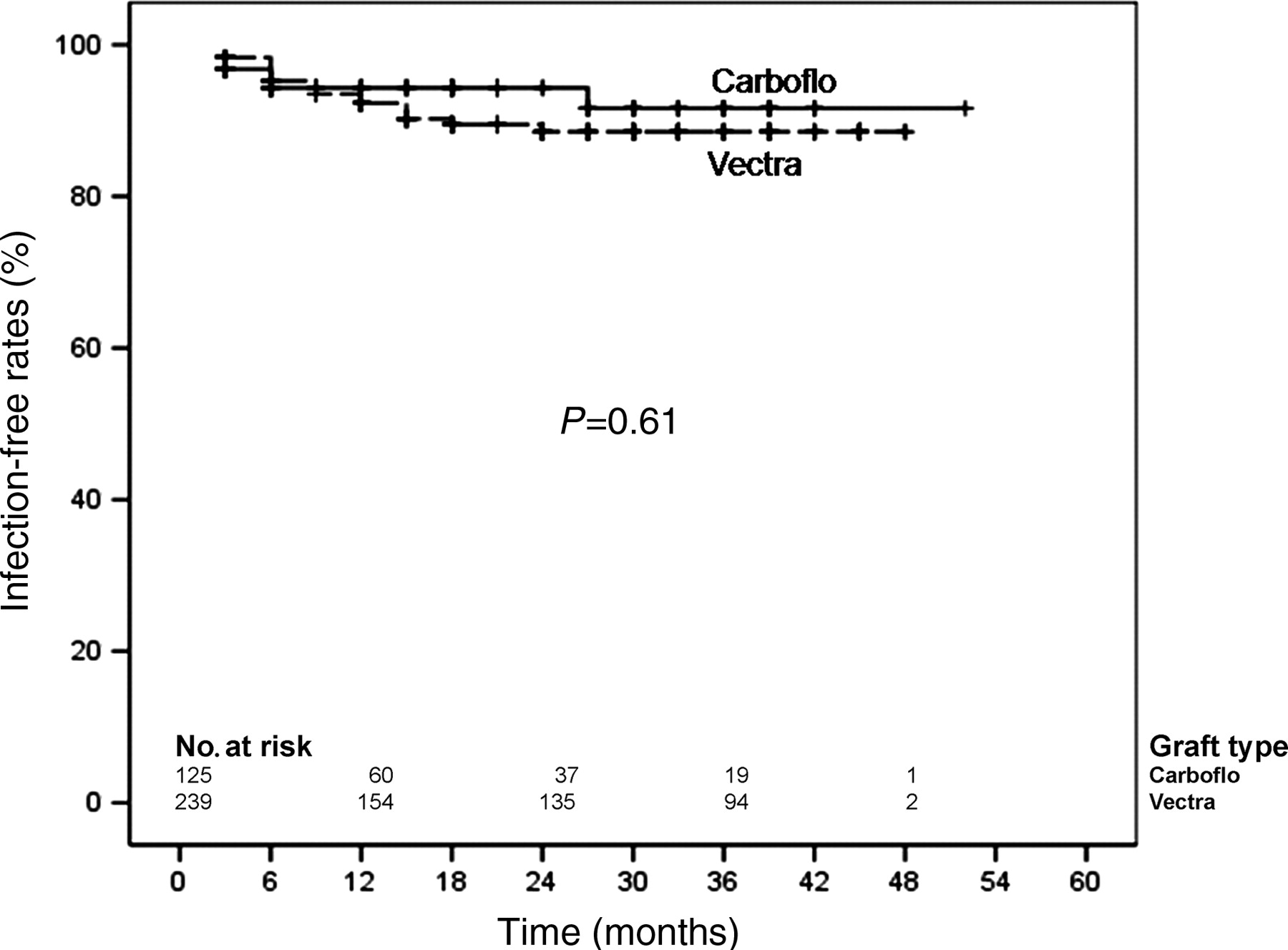
Cumulative graft infection rates at three years of Vectra and PTFE Carboflo grafts. The two groups were comparable. PTFE, polytetrafluoroethylene

Cumulative pseudoaneurysm formation (at needle-stick site) rates at three years of Vectra and PTFE Carboflo grafts. The two groups were comparable. PTFE, polytetrafluoroethylene
Patency was significantly better for the Vectra grafts (Table 2). There was a significant trend for better primary patency of Vectra compared with PTFE Carboflo grafts (15% versus 11%, respectively, at 3 years, P = 0.004, Figure 5a). This difference in patency was 12% for primary assisted patency (39% versus 27%, respectively, at 3 years, P <0.001, Figure 5b) and secondary patency (69% versus 57%, respectively, at 3 years, P = 0.012, Figure 5c) and 15% for functional secondary patency (61% versus 46%, respectively, at 3 years, P = 0.002, Figure 5d).
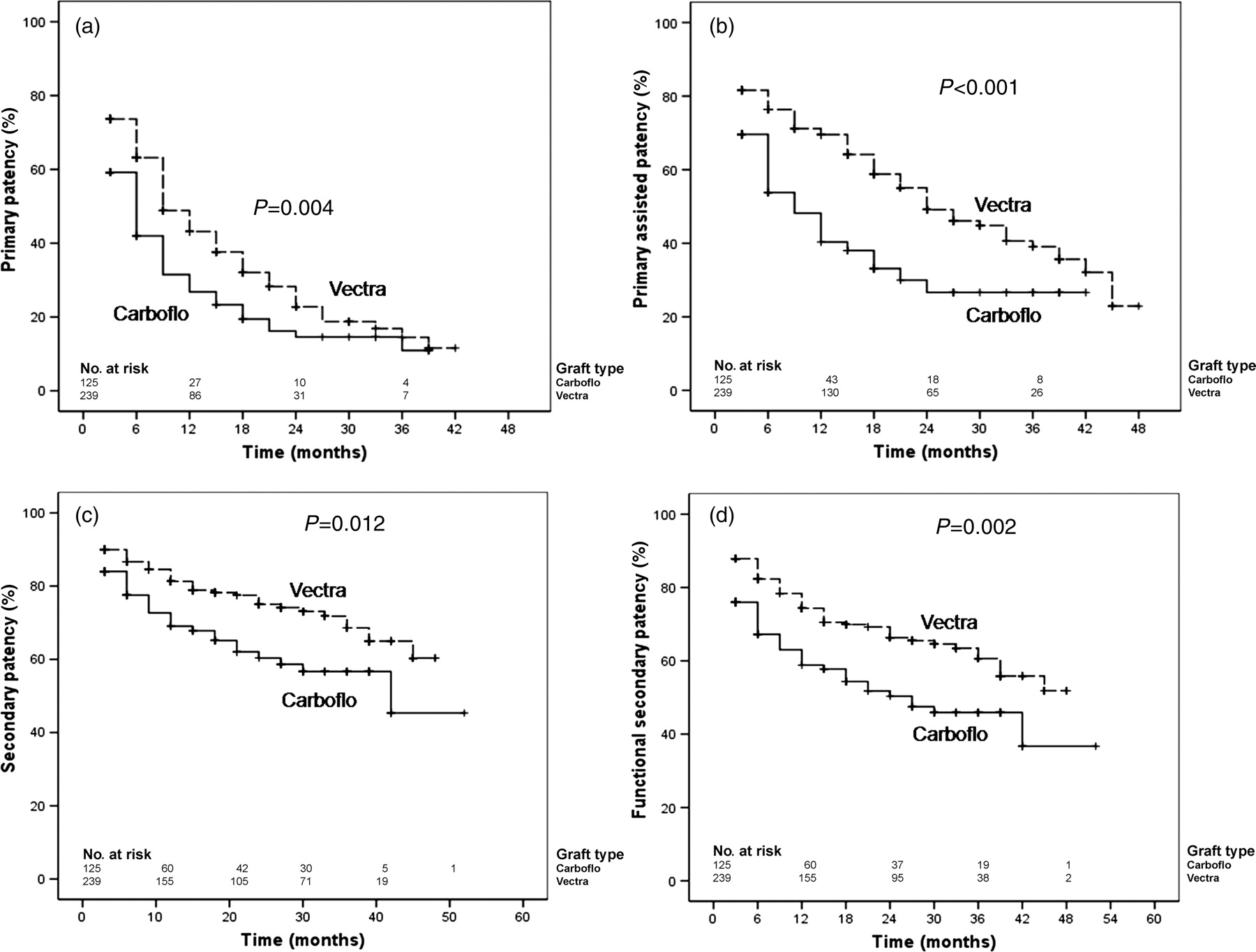
This figure shows long-term patency rates of Vectra and PTFE Carboflo grafts. (a) Comparison of primary patency of Vectra and PTFE Carboflo grafts; there was a significant trend in favor of the former group (15% versus 11%, respectively, at 3 years, P = 0.004). (b) Comparison of primary assisted patency of Vectra and PTFE Carboflo grafts; there was a significant trend in favor of the former group (39% versus 27%, respectively, at 3 years, P < 0.001). (c) Comparison of secondary patency of Vectra and PTFE Carboflo grafts; there was a significant trend in favor of the former group (69% versus 57%, respectively, at 3 years, P = 0.012). (d) Comparison of functional secondary patency of Vectra and PTFE Carboflo grafts; there was a significant trend in favor of the former group (61% versus 47%, respectively, at 3 years, P = 0.002). PTFE, polytetrafluoroethylene
Patency rates of Vectra and PTFE grafts at three years
PTFE, polytetrafluoroethylene
Straight upper arm Vectra grafts had the best secondary patency compared with their PTFE counterparts and loop (Vectra and PTFE) grafts (P = 0.001, Figure 6); however, loop configuration was the single predictor of worse secondary patency on multivariate analysis (P = 0.009, RR 1.7).
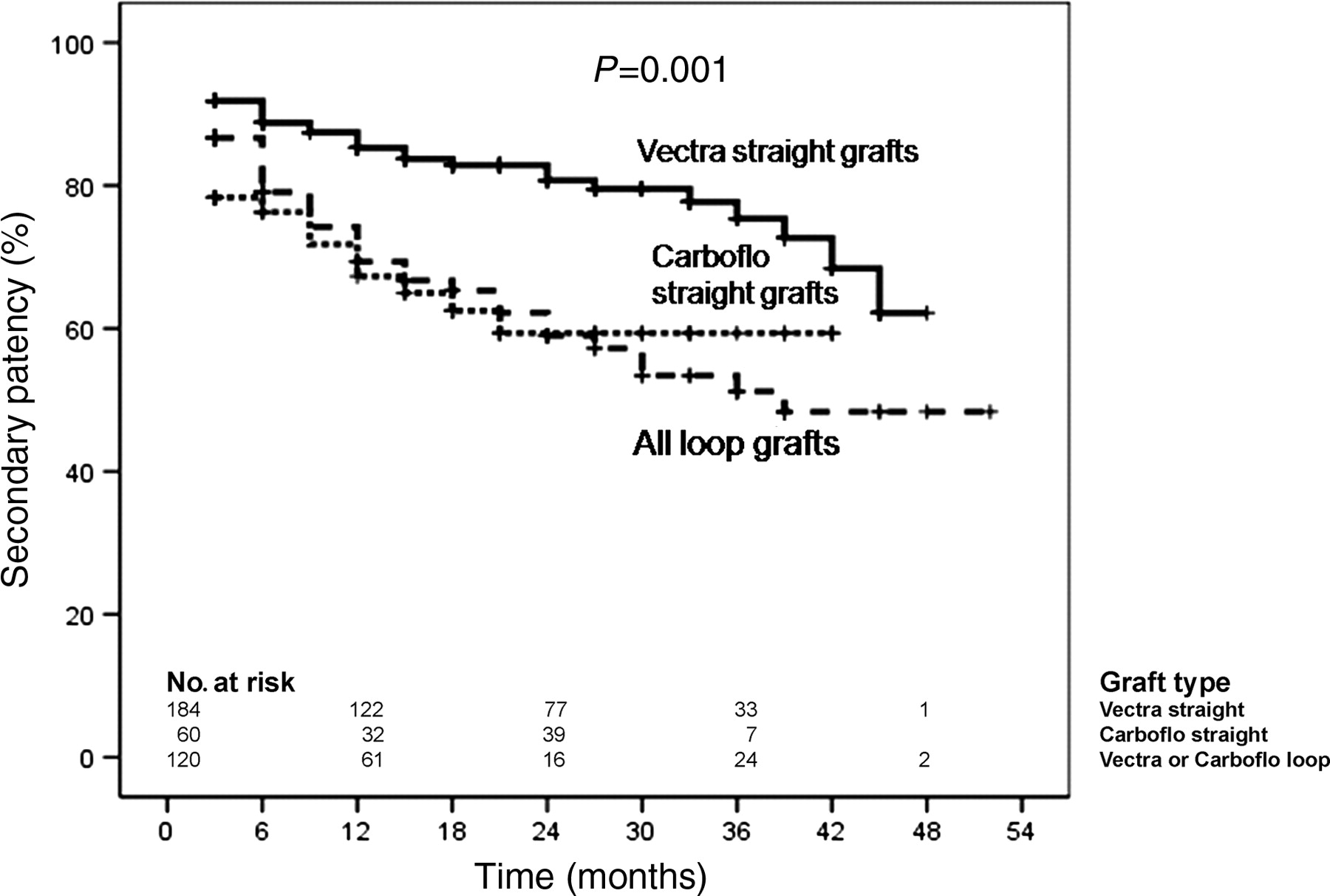
Secondary patency of straight upper arm Vectra, PTFE and loop (Vectra and PTFE) grafts. Results were significantly better for straight upper arm Vectra grafts (P = 0.001). PTFE, polytetrafluoroethylene
Discussion
In the present study we demonstrated satisfactory long-term secondary patency of vascular access grafts, maintained with contemporary endovascular methods. These patency rates were significantly better for Vectra than Carboflo PTFE grafts, in the subgroup of grafts placed in the upper arm. Late infection and pseudoaneurysm formation rates, however, were equivalent, being approximately 10% and 20%, respectively, at three years. Complications of vascular access are known to occur frequently, 12 and the vascular surgeon should be prepared to handle those.
Two prospective studies have demonstrated equivalent secondary patency of Vectra and PTFE grafts, approximately 80% at one year. 13,14 In one of these two studies, however, there was a trend for a better two-year secondary patency for the Vectra compared with PTFE grafts (79% versus 69%), although this 10% difference was non-significant. 14 In our study a 12% difference at three years (Table 2) was statistically significant and the prolonged follow-up might have been responsible for this.
Long-term secondary patency rates of PTFE grafts have been reported to be on average 55% at two years, according to a review on this subject, 15 but corresponding data for the Vectra graft are largely missing. The number of surgical revisions performed to maintain graft patency is unclear in most series, particularly in the older ones. In our study, dysfunction of both graft types have been exclusively managed with endovascular means. The cause of this improved patency might be bias due to patient selection and the cross-sectional nature of our study, but a true difference might exist. In the US Vectra study, kinking occurred in 8.5% of the 71 implanted Vectra grafts but in none of the PTFE grafts (P = 0.028, Fisher's exact test) and this might explain the reported equivalent patency of the two graft types. 13 Improved implantation techniques, 16 recommended also by the manufacturer, have been meticulously followed in our series and might explain some of the observed differences, in favor of the Vectra graft. An additional reason might have been the more frequent development of intragraft stenoses in PTFE grafts, 13,17 as a result of frequent graft puncture. 18 Because Vectra grafts are very compliant, 16 their compliance is closer to native vessels compared with PTFE, and therefore the improved patency shown for Vectra grafts might also be the result of a better compliance match. Despite its increased compliance, the outer layer of the Vectra graft is reinforced with two thin monofilament polyester fibers to increase kink resistance; we believe that these properties reduce collapse of the Vectra graft during thrombotic episodes. This hypothesis is supported further by a randomized study that compared thin wall with standard wall e-PTFE grafts; 19 in agreement with our results, the graft with the thicker (standard) wall had better patency that was evident after the first two years of follow-up. The authors made the assumption that the thick wall configuration may have greater resistance to kinking and compression from tunnel tract hematomas and thrombus and that the thicker wall may also provide a more stable platform for needle-hole thrombus plugging. 19 Similarly, a PTFE graft with internal rings (Intering, W L Gore, Flagstaff, AZ, USA) is claimed to have a reduced risk of thrombosis resulting from graft compression after removal of the cannulation needle, 20 and possibly better long-term patency. Although experimental studies have shown that the carbon lining of IMPRA Carboflo PTFE grafts reduces platelet deposition, 8,9 carbon PTFE has not been shown to have superior patency compared with standard PTFE in hemodialysis, 21 or lower extremity bypass grafts. 22 The microporous inner layer of the Vectra graft has also antithrombotic properties because it is enriched with siloxane that contains a surface-modifying additive, but studies directly comparing this graft type with IMPRA Carboflo grafts are lacking. Further modifications of graft structure have the potential to improve graft longevity, 23 and additional research on this area is warranted. Nevertheless there are additional factors responsible for differences among different series of prosthetic graft, including monitoring and surveillance protocol, 3 and effectiveness of the thrombectomy procedure. 1,17 Although straight upper arm Vectra grafts had the best secondary patency compared with their PTFE counterparts and loop grafts, loop configuration was the single predictor of worse secondary patency on multivariate analysis; graft type was marginally rejected and this is possibly a result of type II error that could be addressed with a larger study or more prolonged follow-up.
In our study we could not confirm the high infection rates of Vectra grafts observed in three studies: 19%, 24 30% 25 and 38%, 7 respectively. Like others, 13,14,26 we did not observe such a problem. Clinical presentation of prosthetic graft infection can be variable and include infected false aneurysm, periprosthetic abscess and tunnel contamination. 27 Alternatively, infection can be classified into operative, hemodialysis-related, postthrombectomy, stump of previously excised graft and spontaneous in abandoned grafts. 28 Exposed grafts are by definition infected and can belong to any of the above categories. Operative infection rates range between 1% and 3%; 28,29 this was 1.7% in our series including one infected seroma in a patient with a PTFE graft. As expected, these rates were low in our series and representative of clean operations. On the other hand, late infection was far more common and similar (about 10%) at three years between the two study groups. About one-third of these infections involved a pseudoaneurysm. The infection rate of PTFE grafts have been reported to vary between 5% and 21%/year. 29–31 This wide range might represent different sterility conditions or patient groups. Cumulative infection rate have been reported to vary between 9% 32 and 42% at 10 years. 29 Recurrence of infection has been reported to be even more frequent than its de novo development and annual rates as high as 12% have been reported. 29 Most infected grafts require early or late excision and variable salvage rates have been reported. One study reported, like our series, a salvage rate of 7%; 31 others have reported a 60% salvage rate, significantly higher for puncture infections (77%) or erosions (90%) than for abscesses (40%) or wound infections (48%). 29
Repeated cannulation of a prosthetic graft may cause degeneration of the graft material and lead to a pseudoaneurysm at the needle-stick site. Originally, Vectra grafts were thought to be pseudoaneurysm-free, 13,14 due to their self-sealing properties that allows early cannulation and avoids development of seromas. More recent studies showed that pseudoaneurysms can indeed develop between 1% and 3.5%. 24,25 Corresponding rates for PTFE grafts are 6%. 19 The vast majority of operated pseudoaneurysms occur after two years, 18 which can explain the difference in reported rates between different series. Improved graft longevity in our study explains the higher average rate (9.9%), which was even higher at 17% (5.7%/year) and 23% (7.7%/year) for Vectra and PTFE grafts, respectively. According to the Kidney Dialysis Outcomes Quality Initiative (KDOQI) guidelines, indicators of risk for graft rupture due to changes in the integrity of the overlying skin include poor eschar formation, evidence of spontaneous bleeding, rapid expansion in the size of a pseudoaneurysm and severe degenerative changes in the graft material. 11 Consequently, indications for revision/repair include grafts with severe degenerative changes or pseudoaneurysm formation in cases where the number of cannulation sites are limited by the presence of a large (or multiple) pseudoaneurysm(s), or if the pseudoaneurysm threatens the viability of the overlying skin, is symptomatic or infected. Interventions for prosthetic graft pseudoaneurysms – 3% annual rate in one study, 31 – are rarely performed, because most of them can be managed conservatively. Surgical revision of complicated pseudoaneurysms reveals acceptable postintervention primary patency rates. 33 Treatment with stent graft has been proposed as an alternative option. 34 In our study five non-infected pseudoaneurysms (5/26, 19%) were managed with a stent graft, which was successful only in three of them.
Our study has several limitations that should be considered when trying to interpret the outcome of patients of the two study groups. First, our investigation had a non-randomized, case-controlled, although prospective design. As such certain bias might have been introduced due to different selection criteria of patients (e.g. age and previous access surgery, especially on the ipsilateral side). However, because particular graft-type implanted was the individual surgeon's preference, we believe that the bias introduced was not the result of intentionally choosing a particular graft type in unfavorable conditions. Also, the long-term infection and pseudoaneurysm rates are more likely related to graft properties and cannulation methods, and probably not associated to initial patient selection which should have an impact on patency rates though. Finally, another confounding variable could be the variable experience of the operating surgeons involved with this study, although they were all in practice for more than 10 years.
In conclusion, three-year secondary patency of vascular access grafts, maintained with contemporary endovascular methods, is satisfactory. In the subgroup of grafts placed in the upper arm, Vectra grafts had better patency than Carboflo PTFE grafts. The two graft types were comparable in terms of late infection and pseudoaneurysm formation rates.
Footnotes
Acknowledgments
Financial disclosure of authors and reviewers: none reported.