
Abstract
In our department we started a program in order to offer a mini-invasive approach to all patients affected by abdominal aortic aneurysms (AAAs), trying to offer this option also to patients not eligible for endovascular aneurysm repair (EVAR) due to unfavorable anatomy, age under 65 years and aorto-iliac occlusive disease, considering nowadays EVAR is the gold-standard for the mini-invasive treatment of AAAs. The aim of this study was to compare endovascular versus fast-track surgical treatment in patients undergoing elective surgery for AAAs. We wanted to verify if it was possible to be totally mini-invasive in the treatment of AAAs. A total of 128 patients were chosen for the study. Ninety-four patients were enrolled in the OPEN group and 34 were enrolled in the EVAR group. This study demonstrates that minimally invasive treatment with the fast-track protocol may be a valid alternative to EVAR.
Introduction
For several years, researchers have focused on the search for what might be considered a ‘stress-free’ technique that could lower the traumatic impact related to surgery to a minimum.
In 1991, the possibility of aneurysm exclusion by endovascular technique raised a great deal of interest in the area of aortic aneurysm treatment. At the same time, traditional surgeons were looking for new invasive methods that could reduce surgery-related stress. Thus, so-called ‘Fast-track surgery’ was born, although it was already being practiced in other surgical areas, 1 including aortic surgery. The introduction of ‘Fast-track management’, including mini-invasive surgery, stress-free anesthesia and analgesia and enforced postoperative rehabilitation, has provided important possibilities for enhanced recovery after surgical procedures. It is not clear at present as to what is the relative importance of individual, surgical or anesthetic features in the enhancement of recovery.
Minimally invasive surgery does not simply mean surgery that is performed through a ‘small incision’, but it is a new concept in the treatment of patients, and it implies a review of the whole perioperative process. 2 Fast-track surgery is therefore a team activity, thus making it mandatory to review the philosophy of the whole team, from the surgeon to the anesthesiologist, down to the nurse and the patient him/herself.
In our department we started a program in order to offer a mini-invasive approach to all patients affected by abdominal aortic aneurysms (AAAs), trying to offer this option also to patients not eligible to endovascular aneurysm repair (EVAR) (considering that nowadays EVAR is the gold-standard for the mini-invasive treatment of AAAs) due to unfavorable anatomy, age under 65 years and the presence of aorto-iliac occlusive disease.
The aim of this study was to compare endovascular versus fast-track surgical treatment in patients undergoing elective surgery for AAAs at the Vascular Surgery Unit of the Novara University Hospital. We wanted to verify if it was possible to be totally mini-invasive in the treatment of AAAs.
Materials and methods
We carried out a retrospective study on patients affected with AAAs who underwent elective surgery between January 2006 and September 2007 in the Division of Vascular Surgery in Novara. Emergency surgery patients were excluded from the study.
During this period, 184 patients affected by AAAs underwent elective surgery at our institution, and among them, 128 patients were chosen for the study. Ninety-four patients were enrolled in the OPEN (left subcostal mini-laparotomy) group (73.4%) and 34 were enrolled in the EVAR (endovascular aneurysm repair) group (26.6%).
In the group of patients treated by the open technique, we have chosen only the patients who underwent surgery by the minimally invasive technique (left subcostal incision), in order to avoid all possible statistical bias due to the surgical technique performed. All cases that had been treated by extraperitoneal surgical access, as well as the ones treated by accesses other than the left subcostal minimal incision, were excluded from the study; all patients were also treated with a fast-track protocol. Our study also included patients who underwent surgery using the minimally invasive technique in operations requiring clamping either suprarenally or at the iliac bifurcation in the presence of common iliac artery disease. 3
Exclusion criteria for the endovascular technique were the presence of a juxta-renal (or with a collar < 7 mm) aneurysm, an especially tortuous and/or stenotic iliac axis (caliber < 6 mm) and chronic renal failure.
All patients were treated by the same team of health professionals following the protocol described below.
Preoperative protocol
Diagnostic imaging
Thoracic-abdominal computed tomography (CT) angiography was performed on all patients in both groups (except for those who had recently undergone this examination). Maximum intensity projection reconstructions, multiplanar reconstructions and volume rendering were carried out in anticipation of EVAR by using multislice CT (64-slice MSCT, with size cuts of 1.25 mm) which allowed the exam to be carried out quickly and low doses of contrast agent to be used (70 mL of Iomeron 300, Bracco SpA, Milan, Italy).
In order to obtain full cooperation, all patients and their families were summoned to the hospital, and the patients were examined prior to admission. The whole health-care team (including surgeons, anesthesiologists and nurses) participated in these meetings, during which the patients were provided with information concerning both the surgery and the perioperative therapy.
Before surgery, all patients continued taking their usual medication, except for warfarin which was discontinued seven days prior to surgery and was replaced by low-molecular-weight heparin until the evening before the operation.
‘Mild’ intestinal preparation was carried out in both groups, as follows:
Three days prior to surgery: senna (Pursennid 12 mg, Novartis Consumer Health SpA, Basel, Switzerland), two tablets at 8 p.m; Two days prior to surgery: senna (Pursennid 12 mg, Novartis Consumer Health SpA) two tablets at 8 p.m., one tablet of vegetable carbon three times a day, low-fiber diet; One day prior to surgery: one tablet of vegetable carbon three times a day, low-fiber diet.
Two hours prior to surgery, 0.1 mg/kg of intramuscular morphine was administered.
EVAR patients were hydrated with 500 mL of saline solution and with 600 mg of n-acetylcystein before and after surgery.
Intraoperative protocol
Anesthesiological technique in the OPEN group
To achieve sensory block (pin-prick tested) between T4 and L5 dermatomes, an epidural catheter was placed at the T6–T7 interspace and 15–25 mL of 0.5% bupivacaine was administered. An epidural infusion of 0.5% bupivacaine at a rate of 2–5 mL/hour was maintained throughout and for the first 48 hours after surgery. The induction of a light general anesthesia was achieved with 0.11 mg/kg midazolam and 1 mg/kg propofol. A laryngeal mask was inserted and ventilation with 80% oxygen was performed while maintaining patients in spontaneous breathing. Anesthesia was continued with 0.4 minimum alveolar concentration sevofluorane. No curare was administered. A thermal blanket placed to keep the exposed parts of the upper body warm allowed the patients to remain normothermic. Cell saver was routinely used.
No opioid anesthesia was administered during the intra- or postsurgical period.
Anesthesiological technique in the EVAR group
On the basis of the patient's characteristics, the anesthesiologist chose from among:
Subarachnoid anesthesia; Lumbar peridural anesthesia; Sedation associated with local infiltration.
No opioid anesthesia was administered during the intra- or postsurgical period.
Surgical technique in the OPEN group
Patients were placed on the surgical bed in the supine position. The prosthesis was implanted through a transperitoneal access with a left subcostal transverse mini-incision, resecting the left rectus muscle of the abdomen, the posterior layer and the anterior peritoneum followed by manual dislocation of the intestinal mass without using orthostatic retractors (no disembowelment was done). Mini-laparotomy is associated with less hemodynamic instability, fluid shift and hyperthermia, inflammatory response and immunosuppression, pain and ileus. In addition, transverse laparotomy produces lower traction on the wound edges, therefore requiring less muscle relaxation, better pain relief and lower respiratory impairment. 4
Clamping was performed using flexible clamps or Foley's catheters # 12 for the iliac arteries.
Standard surgical instruments were used for the anastomosis. The incision was closed by continuous peritoneal suture using the posterior band of the rectus muscle (with absorbable Vycril 2/0 suture; Ethicon SpA, Pomezia, Italy), after which the anterior band of the rectus muscle was also sutured using the same technique (with non-absorbable Ethibond Excel Polyester 0 suture, Ethicon SpA). Closure was performed without placing drainage tubes. The technique of mini-laparotomy may have some difficulties in overweight patients, due to the deeper site of anastomosis, performed with standard instruments with less space than with a median standard incision. This disadvantage in our opinion is not very important, with respect to the advantages of this incision: faster to perform and to close with respect to the standard median incision, less postoperative pain and ileus, lower traction on the wound edges, better pain relief and respiratory impairment.
In our program, we combined mini-laparotomy with intraoperative regional anesthesia and continued postoperative epidural infusion. Attenuation of the catabolic component of the stress response, provision of excellent pain relief that facilitates mobilization, reduction of pulmonary, cardiac and thrombotic complications, faster recovery of intestinal function, improvement of substrate utilization after surgery, decrease in postoperative protein breakdown and preservation of tissue protein, are the most important advantages of thoracic epidural anesthesia and analgesia.
Surgical technique in the EVAR group
All the procedures were carried out in a dedicated angiographic room next to the operating room in case the need arose for surgical conversion.
A digital angiograph (Philips Integris 5000; Royal Philips Electronics, Amsterdam, Holland) and organic iodide angiographic contrast media (Iomeron 300; Bracco SpA) were used.
Bilateral femoral access was performed, including preparation of the femoral bifurcation and examination of the common femoral artery, the profunda femoral artery (PFA) and the superficial femoral artery (SFA) using vessel loops. Following a right common transfemoral injection, preliminary aortographic examination was carried out by positioning a marker pigtail catheter using the Seldinger technique.
After systemic heparinization (50 IU/kg), followed by clamping of the SFA and PFA to avoid embolization, the endoprosthesis was advanced at the proper angle until the edge of the origin of the renal arteries was reached, all the while continuously under fluoroscopic control.
After road mapping at the level of the proximal collar, the endograft was released using the origin of the most distal renal artery as the reference point.
Catheterization of the contralateral iliac axis, followed by placement of the residual endoprosthesis branch was done using an angled catheter (Cobra or vertebral; Cordis Corporation, Bridgewater, NJ, USA).
After releasing all the iliac extensions and re-modeling the junctions using a compliant balloon catheter, final angiography was performed to verify the correct position of the endoprosthesis, the patency of the renal and internal iliac arteries and to check for the absence of type 1 endoleaks.
After removing the introducers, we performed arteriography of the femoral arteriotomies using polypropylene 6–0. No drainage tubes were placed at the surgical accesses.
Intraoperative management
The upper bodies of all patients were warmed by using a warm air ventilation system and by heating the infused liquids. Administration of fluids was regulated on the basis of the estimated loss of water (respiratory circuit and convection) and of blood. Nasogastric tubes were not used.
End of surgery protocol
All patients were woken up directly in the operating room. An abdominal elastic support band was placed. After verifying the stability of the hemodynamic and respiratory parameters, the patients were transferred to the ward.
Postoperative protocol for OPEN and EVAR groups
In the OPEN group, analgesia was administered for 48 hours by continuous infusion of peridural local anesthetic associated with 600 mg ibuprofen orally administered every eight hours, 5, 6 while in the EVAR group, analgesia was assured by administering 600 mg ibuprofen orally every eight hours. Ketoprofen 100 mg intravenous (every 12 hours) was scheduled for additional demand of analgesia in both groups.
Both groups followed an accelerated rehabilitation program. Patients were given liquids right away, followed by a semisolid diet after 1–2 hours, and a light dinner on the evening of the surgery.
Misoprostol 200 mg and metoclopramid 10 mg was orally administered every 8 hours, and 10 mg of vegetable fibers (apple pectin) twice daily and any previous medication was immediately resumed.
Patients were forced to perform breathing exercises while resting in bed. An oxygen mask was provided during the first two postoperative nights. Soon after surgery, patients were encouraged to start bed exercises and foot-pump. When in the absence of motor block and when in the presence of stable hemodynamic parameters, patients were forced to ambulate with assistance. Oral administration of salicylic acid 100–325 mg/day was started four hours after surgery.
The bladder catheter was removed at 6 a.m., the morning after surgery.
In case of lack of bowel movement, a tablet of senna (Pursennid 12 mg, Novartis Consumer Health SpA) was administered the evening following surgery.
We evaluated the following data for patients in both groups:
Personal data (sex, age); Body mass index; American Society of Anesthesiologists (ASA) class; Metabolic equivalent (MET) in line with the most recent standards of the patient's functional capacity; Associated co-morbidities; Aneurysm diameter at the time of surgery; Intraoperative data (length of surgery, infusions, blood and liquid loss, complications and so on); Hospitalization data (clinical conditions, blood tests, complications and so on); Discharge.
Please note that ‘day 0’ refers to the day of surgery, and ‘day 1’ refers to the first day after surgery.
Statistical analysis
Nominal and ordinal variables are given as absolute and relative frequencies. Continuous variables are given as average ± standard deviation. Analysis for repeated surveys was carried out by repeated measures analysis of variance.
Comparison between normally distributed independent variables was performed using the two-tailed Student's t-test. P < 0.01 was considered statistically significant.
Results
Between January 2006 and September 2007, 246 patients affected by AAAs were treated at the Department of Vascular Surgery at the Maggiore della Carità Hospital (Novara, Italy): 62 were emergency surgeries (ruptured aneurysm or in a phase of rupture) and 184 were elective.
After excluding patients on the basis of the previously listed criteria, 128 patients were enrolled in the study, including:
Ninety-four patients who underwent surgery by the minimally invasive technique, i.e. the OPEN group; Thirty-four patients who underwent surgery by the endovascular technique, i.e. the EVAR group.
The selection of the technique was made by the surgeon with the patient himself, after a specific explanation of both techniques and their results.
Demographic characteristics
BMI, body mass index; AAA, abdominal aortic aneurysm; OPEN, left subcostal mini-laparotomy group; EVAR, endovascular aneurysm repair group
Associated co-morbidities
OPEN, left subcostal mini-laparotomy group; EVAR, endovascular aneurysm repair group; COPD, chronic obstructive pulmonary disease
Preoperative risk
OPEN, left subcostal mini-laparotomy group; EVAR, endovascular aneurysm repair group; ASA, American Society of Anesthesiologists; MET, metabolic equivalent
It must be pointed out that arterial hypertension and smoking were both present simultaneously in 76% of the OPEN group and in 58% of the EVAR group. Several risk factors were also associated in many other patients.
Demographic characteristics and co-morbidity for both groups are superimposable, except for diabetes which is more common in the EVAR group.
We found that:
Thirty-four percent of the OPEN group patients had undergone previous abdominal surgery (32 patients); Thirty-five percent of the EVAR group patients had undergone previous abdominal surgery (12 patients).
Operative risk proved to be higher in the EVAR group as shown by the ASA class (ASA 4 in 61.8% of the EVAR patients versus 28.7% in the OPEN group) and by the MET class.
Table 4 summarizes the type of surgery that was performed in the two groups.
Type of surgery performed
OPEN, left subcostal mini-laparotomy group; EVAR, endovascular aneurysm repair group
In the OPEN group, one patient had to be converted to the bisubcostal incision in order to control an aortic lesion in the clamping area.
Due to the occlusion of an iliac axis in one patient in the EVAR group, an aorto-uniliac endoprosthesis had to be implanted, while in six patients the internal iliac artery required embolization to allow the correct sealing of the endoprosthesis and to avoid endoleak.
Regarding the anesthesiological technique that was used:
All the patients in the OPEN group received peridural thoracic analgesia during surgery, associated with light anesthesia, through a laryngeal mask while in spontaneous breathing; Postoperative analgesia consisted of a 48-hour continuous infusion of peridural local anesthetic associated with oral non-steroidal anti-inflammatory drugs; The anesthesiological technique in the EVAR group varied from patient to patient: six patients underwent general anesthesia, four received peridural and 22 were given subdural anesthesia.
With regard to transfusions, 15 patients in the OPEN group (16%) and nine patients in the EVAR group (27%) received transfusions. Furthermore, 56 patients in the OPEN group were re-transfused with blood that had been retrieved during surgery, with an average of 410.32 mL per patient (±214.11).
Blood loss in the EVAR group was caused by the blood transfer through the arteriotomy and the introducers. In this group, blood that was lost was not retrieved (autotransfusion) and transfused, as was the procedure in the OPEN group, because in our department, at the time of the study, the cell saver was not placed in the hybrid operatory room.
After surgery, patients rose from the bed as follows:
Eighty-nine patients (98%) in the OPEN group got up, on average, two hours after the end of surgery; Twenty-seven patients (80%) in the EVAR group got up, on average, during day 1. In 98% of the patients in the OPEN group; In all the patients in the EVAR group (100%).
Following surgery, food intake resumed on day 0:
Vomiting occurred in 12% of the OPEN patients and in 9% of the EVAR patients, which, however, did not influence resumption of oral nutrition. Such episodes were extremely rare on day 1 (3% OPEN and 3% EVAR). The main intraoperative and postoperative characteristics are listed in Table 5.
Intraoperative and postoperative parameters
OPEN, left subcostal mini-laparotomy group; EVAR, endovascular aneurysm repair group
Trends in diuresis and creatinine levels do not overlap in the two groups. Greater intravenous infusion of liquids was needed in the EVAR group on day 0, and continued in 22% of the EVAR patients and in 12% of the OPEN patients on day 1. This is related to the fact that a renal protection protocol requiring intravenous infusion of liquids (10 mL/kg/hour in the first 24 hours) was applied to the EVAR group because of the possible contrast medium-induced nephropathy.
Even though the result is not statistically significant, it is interesting to note that a greater movement of troponin was observed in the OPEN group, albeit with no changes in ECG. Cardiac troponin I is a specific marker of cardiac damage; there is no cross-reactivity with the skeletal muscle isoforms. Our study could not determine the critical level that could influence the postoperative course, but a favorable outcome in 100% of the patients may suggest physiological effects of the aortic-iliac axis clamping.
Postoperative pain control was significantly better (P = 0.001) in the EVAR group, although the average analogic visual scale of pain (VAS) score in the OPEN group never went above 19 on a scale from 0 to 100 (Figure 1).
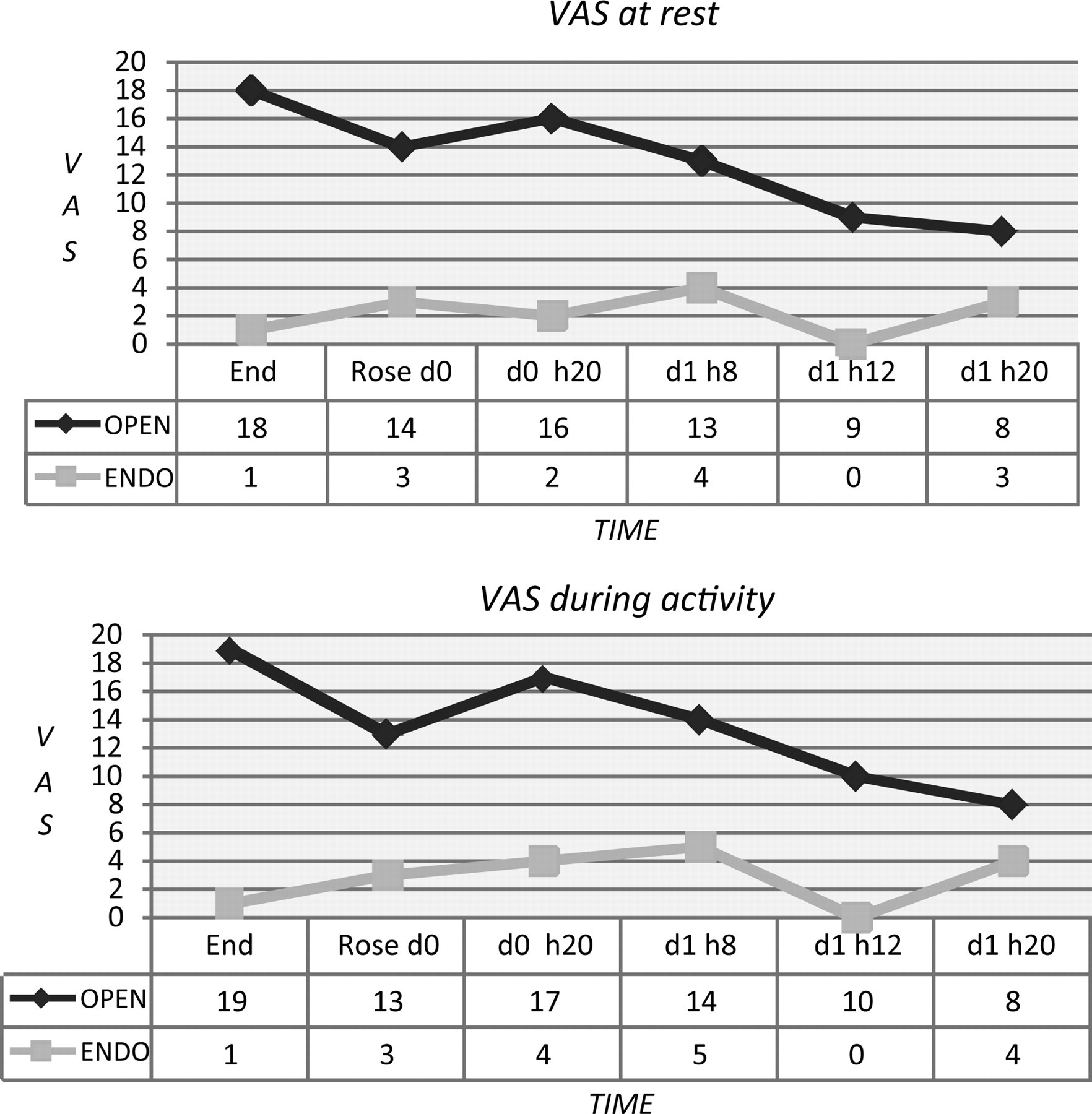
VAS at rest and during activity
This is due to the fact that the OPEN group underwent laparotomic access, and although it was of limited size, it was associated with greater pain as compared with the inguinal incision that was used in the EVAR group.
Postoperative complications on day 30 are shown in Table 6.
Thirty-day postoperative complications
OPEN, left subcostal mini-laparotomy group; EVAR, endovascular aneurysm repair group; MOF, multiorgan failure; VF, ventricular fibrillation, ARF, acute renal failure; AF, atrial fibrillation
It must be pointed out that 24% of the EVAR group patients showed an increase in temperature in the postoperative period. We observed fever with a body temperature ranging from 37.8 to 38.2°C, with negative blood cultures. Passage of stool occurred on day 2 in the OPEN group, and on day 1 in the EVAR group.
Patients in both the OPEN group and in the EVAR group were discharged on the fourth postoperative day (median). Postoperative discharge days for the two groups are reported in Figure 2.
Postoperative discharge day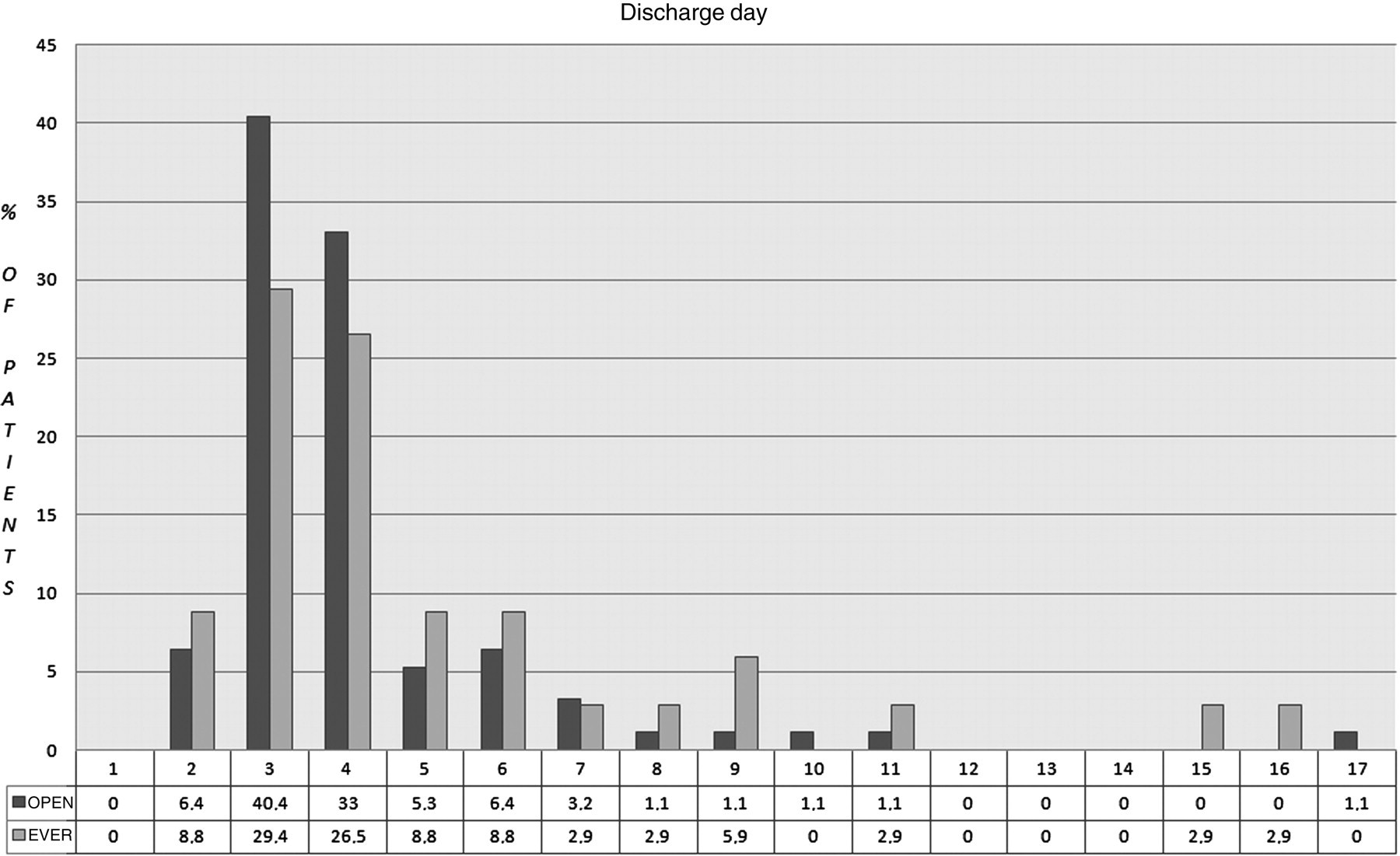
Discussion
The aim of this work was to compare the perioperative period in patients treated by the endovascular method (EVAR) to that of patients undergoing the fast-track approach with left subcostal mini-incision (OPEN), in order to verify whether it was possible to treat all patients affected by AAAs with a mini-invasive approach, with the open or endovascular technique.
EVAR would appear to cause less stress on the organism and to have an attenuated cytokine-mediated inflammatory response, also on account of the reduced hemodynamic shock on the organism. 7 Many studies in the literature report that EVAR also shows better results than the open traditional technique with regard to perioperative outcome and hospitalization. The Dutch Randomized Endovascular Aneurysm Management (DREAM) trial and the Endovascular Aneurysm Repair Trial 1 (EVAR-1) have, however, demonstrated that mortality rates for EVAR and OPEN overlap after two years of follow-up. 8
The European Collaborators Registry on Stent-graft Techniques for AAA repair (EUROSTAR) 9 reported that EVAR had an 18% (approximate) re-intervention rate after 14 months of follow-up, and that 12% of these patients required laparoscopic access, 11% underwent extra-anatomic bypass and 76% had transfemoral procedures.
Lederle et al. 10 reported the data from the Open vs Endovascular Repair (OVER) trial, a randomized multicenter clinical trial of 881 veterans (aged 49 years) from 42 Veterans Affairs Medical Centers with eligible AAAs who were candidates for both elective endovascular repair and open repair of AAAs. In this randomized trial, endovascular repair resulted in fewer perioperative deaths than open repair, even though open repair was performed with low mortality. Two European trials, the UK EVAR-1 11 and the DREAM trial, 12 previously reported lower operative mortality with endovascular versus open repairs. Perioperative mortality in OVER was lower than in the European trials for both treatments. Mortality within 30 days or during hospitalization for endovascular repair was 2.1% in the EVAR-1 trial, 1.2% in the DREAM trial and 0.5% in the OVER trial, and for open repair, mortality was 6.2% in the EVAR-1 trial, 4.6% in the DREAM trial and 3.0% in OVER.
Murphy et al. 13 simply accelerated the recovery without changing the surgical or anesthesiological techniques. In 2005, Abullarage et al. 14 compared EVAR with the open technique using the fast-track protocol for the treatment of elective AAAs through retroperitoneal access. This comparison showed that surgery lasted longer and that the number of blood transfusions and liquid infusions was higher in patients undergoing the open technique using the fast-track protocol. However, length of hospitalization in the EVAR group was the same, but costs were lower in the open-technique group.
Consistent with the literature data, among our group of 128 patients, a greater number of high-risk patients underwent EVAR. It must, however, be stressed that risk stratification was not an exclusion criterion for open surgery, since 68% of the patients were in MET classes ranging from 4 to 7.
It must also be pointed out that there are no significant differences between the OPEN and EVAR groups regarding the duration of surgery or blood loss.
During the intraoperative period, the OPEN group patients received about 500 mL more blood than the EVAR ones (data referred to abdominal opening), while in the postoperative period, the OPEN group patients required fewer intravenous infusions than the EVAR patients.
In fact, the lesser ‘aggressiveness’ of EVAR is due to the fact that abdominal access is not foreseen.
One of the advantages of the OPEN technique we perform, as compared with the traditional technique, may be the reduced surgical trauma due to the transverse mini-incision and to the decreased peritoneal exposure. 1
It is noteworthy that all the OPEN group patients but two, rose the same afternoon following surgery. As a matter of fact, over the years, our team has acquired considerable knowledge about the perioperative management of open-surgery aneurysm patients based on accelerated recovery techniques. 1 Therefore, mobilization on day 0 is a routine event. On the contrary, since the information that is available in the literature regarding the management of EVAR patients is not reassuring, during the first months of the study, we did not attempt to have the patients rise on day 0, while this was later accomplished in the following patients. This may explain the difference in length of stay, which is higher in the EVAR group, but in the last year, we changed our protocol and the EVAR patients rose 2–3 hours after surgery.
With regard to nutrition, as described in the literature, feeding was immediately resumed in the EVAR group during the postoperative period. This, however, also occurred in the OPEN group, thanks to the early feeding programs.
While in the EVAR group, bowel movement occurred within the expected time frame (day 1), bowel movement in the OPEN group in day 2 proved to be faster than what is reported in the literature regarding traditional OPEN surgery. This is due to both the minimal surgical and anesthesiological invasiveness and to the postoperative protocols of accelerated rehabilitation. We believe that not using opioids in the intra- and postoperative period was a significant factor.
No discrepancies regarding renal function data were observed between the two groups.
Although the sample size is small and statistical significance is not reached, it is interesting to underline an increased movement of troponin in the OPEN group. This increase may be attributed to the physiological effects of the aortic-iliac axis clamping. One feature that does stand out is postoperative pain, which was undoubtedly better controlled in the EVAR group.
Some fundamental data must be pointed out. First of all, no abdominal wounds were present in the EVAR group. The OPEN group reported optimum median postoperative analgesia VAS scores: 15 at rest and 16 while moving. While the VAS score remained unchanged on days 0 and 1 in the EVAR group, a progressive decrease in pain was observed in the OPEN group. In fact, on the evening of day 1, it was almost the same as the score in the EVAR group. These data can be confirmed by the fact that the request for supplementary analgesia decreased in the OPEN group the day after surgery, while in the EVAR group, it increased. This latter observation may be accounted for in several ways: on day 0 the VAS score in the OPEN group is strongly influenced by lumbar pain, that is typically observed following retroperitoneal access, but which decreases on day 1; on day 0 the EVAR patients have not yet risen from bed, and therefore the pain is greater on day 1.
Although the duration of hospitalization should not be considered a primary goal, in the last few years the length of hospitalization has been one of the targets in the comparative studies between EVAR and open standard. These studies have almost always shown an advantage of EVAR over open surgery.
None of the patients in either group required postoperative admission to an intensive care unit.
If the discriminating factor between techniques is the length of hospitalization (as related to costs), at the end of our work we can confirm that the OPEN minimally invasive technique overlaps the EVAR technique. A limit of this study is related to the fact that this is a retrospective study.
Performing a randomized, prospective study would have ethical limits since to date, the two techniques do not totally overlap, due to the exclusion criteria of EVAR.
In conclusion, we can say that the study is an expression of a 10-year experience of our team in the research of mini-invasive approach to AAAs. We think that a Vascular Surgery Unit must be mini-invasive with all patients treated in elective conditions, with the aid of the endovascular or open technique.
Footnotes
Acknowledgments
Financial disclosure of authors and reviewers: None reported.