
Abstract
The purpose of this work is to investigate the correlation between regional oxygen saturation (rSO2) changes and stump pressure (SP) during cross-clamping of the internal carotid artery in carotid endarterectomy (CEA) and verify the perspectives of rSO2 to become a criterion for shunting. Sixty consecutive CEAs under general anesthesia were studied prospectively. Selective shunting was based on SP ≤40 mmHg exclusively. Regression analysis with high order terms and receiver operating characteristic analysis were performed to investigate the association between ΔrSO2(%) and SP and to determine an optimal ΔrSO2(%) threshold for shunt insertion. A quadratic association between ΔrSO2(%) and SP was documented regarding the baseline to one and five minutes after cross-clamping intervals. A cut-off of 21 and 10.1% reduction from the baseline recording was identified as optimal for the distinction between patients needed or not a shunt regarding the first and fifth minute after cross-clamping, respectively. In conclusion, cerebral oximety reflects sufficiently cerebral oxygenation during CEA compared with SP, providing a useful mean for cerebral monitoring.
Keywords
Introduction
Clamping of the internal carotid artery (ICA) during carotid endarterectomy (CEA) may result in neurological deficits due to the insufficiency of blood supply to the brain. Adequacy of cerebral perfusion during the clamping period depends on the collateral circulation. However, in many cases (for example, stenosis or occlusion of the contralateral ICA, or anatomical variations of the circle of Willis) the collateral circulation might prove unable to respond to the needs for blood and oxygen and thus cerebral damage may develop. 1–3 The frequency of perioperative stroke during CEA ranges from 1.1 to 7.5% in several studies, 4–8 while a mortality rate between 0.1 and 1% is reported in the literature. 9 Being aware of the status of brain oxygenation is, therefore, a matter of importance during CEA, especially during the ICA cross-clamping.
The decision for shunt insertion during the ICA occlusion is one of the critical points to be decided. 10,11 Several methods have been used for monitoring neurological function during the operation in order to allow adequate interventions and to prevent cerebral hypoperfusion. Electroencephalography, 1,11–14 transcranial Doppler, 12,15,16 somatosensory evoked potentials 11,17,18 and stump pressure (SP) 1,11,12,19 are the most frequently used techniques for this purpose. Nevertheless, despite the great experience, so far none of these methods are considered to be the gold standard. CEA under regional anesthesia and constant examination of the neurological status is an additional, less used but apparently more direct, method that is not exempted from complications. 1,12,20,21
Cerebral oximetry is a non-invasive technique that may provide realtime information about cerebral oxygenation by using near-infrared spectroscopy. 22–25
Reduction in regional oxygen saturation (rSO2) >20% during ICA cross-clamping has been used as a cut-off point for development of cerebral ischemia, 4–6,25 while different optimal thresholds or failures in determining a cut-off point are revealed by other studies. 26–29
This study investigated the correlation between rSO2 and SP to determine the use of rSO2 in becoming a criterion for shunt insertion.
Methods
Between June 2007 and April 2009, 56 consecutive patients (11 women) with mean age 71 years (range: 36–83 years) undergoing 60 CEAs under general anesthesia were studied. They all presented with high-grade ICA stenosis (>70% in symptomatic patients and >80% in asymptomatic patients) documented by preoperative color duplex ultrasound. According to these criteria, four patients had to undergo a bilateral side endarterectomy, although none of them at the same time (the time interval between the two procedures ranged between 7 and 45 days). All patients underwent a standard longitudinal CEA by the same surgeon using patch closure of the arteriotomy with bovine pericardium. 30 Intravenous heparin was administered before clamping. Intraoperative care and monitoring after the operation were provided by the same team of anesthesiologists. All patients were informed about the study and gave written consent. The study was conducted at the University Hospital of Ioannina, Greece, and was approved by the Institute's Committee on Human Research.
The cerebral oximeter that was used in this study was the INVOS SYSTEM 4100 (Somanetics Corporation, Troy, MI, USA). This device consists of one portable bedside monitor and two disposable optical sensors, which are applied to the patient's forehead. Details of the principles of cerebral oximetry have already been described. 6,24,25,31 A baseline rSO2 measurement was obtained while the patient was still awake. rSO2 was continuously monitored during the operation. The measurements of the ipsilateral hemisphere were recorded one minute before ICA cross-clamping (preclamp) and one and five minutes after ICA cross-clamping (after clamp). Selection of the first minute after clamp benchmark was due to the need of examining the rSO2 changes in a short lapse after cross-clamping, beyond which possible cerebral hypoperfusion would become dangerous. The five minutes after clamp time lag was selected as representative of the latter circulatory responses after the time required for autoregulation. 26 The relative rSO2 changes, denoted as ΔrSO2(%), were calculated. For instance, concerning the preclamp time point, ΔrSO2(%) was calculated as follows: ΔrSO2(%) = 100 × (rSO2preclamp − rSO2baseline)/rSO2baseline. The baseline rSO2 value, the rSO2 measurement for each specific time point and the %rSO2 change between them were continuously provided by the oximeter. In addition, mean blood pressure and heart rate were monitored continuously and regulated to be within the range of ±20% compared with the preoperative measurements. Coexisting factors that could affect arterial pressure and heart rate, such as hypertension, arrhythmias or use of β-blockers, were taken into account and each patient was treated as a separate individual.
No decision was based on cerebral oximeter recordings. SP was measured before cross-clamping and was the exclusive criterion for selective shunting. Calligaro and Dougherty, 32 in a study of 474 carotid endarterectomies with cervical block anesthesia and 142 under general anesthesia, showed that an SP value ≤40 mmHg was a threshold for shunting. We adopted our criterion for shunting to SP ≤40 mmHg according to this publication, which was recently confirmed by another study. 33
Statistical analysis
In order to provide insight into the properties of rSO2 as a criterion for shunt insertion, statistical analysis encompassed two axes: (i) overall association between ΔrSO2(%) and SP and (ii) evaluation of various ΔrSO2(%) criteria at the first and fifth minute after cross-clamping with receiver operating characteristic (ROC) analysis. Concerning axis (i), regression analysis with high-order terms was performed. Specifically, apart from the first-order association, second-order and, if appropriate, third-order, coefficients were evaluated to better describe the association between SP and ΔrSO2(%). The assumption necessitating the normal distribution of residuals was tested with the Kolmogorov–Smirnov test. Statistical analysis was performed with STATA 8.0 software (Stata Corp, College Station, TX, USA). Concerning axis (ii), ROC analysis was performed assessing various criteria in the literature. 4,5,7,26–28,34–37 For the determination of the optimal cut-off point in ΔrSO2(%), the Youden's index (maximization of sensitivity + specificity − 1) was adopted as this index seems to represent the best approach. 38 The need for shunting (SP ≤40 mmHg) was treated as the gold standard at the ROC analysis.
Results
Applying an SP ≤40 mmHg as a criterion for development of cerebral ischemia, 32,33 seven of the patients (one woman and six men) needed insertion of a shunt in order to maintain adequate cerebral perfusion (group S), while for the remaining 53 patients, shunt placement was not considered necessary (group NS). None of the patients exhibited any neurological dysfunction after the operation. Table 1 provides a comparison between the NS and S groups regarding demographic data and attendant diseases and Table 2 presents ΔrSO2(%) in these subgroups.
Demographic data and attendant diseases in the NS and S groups
ICA, internal carotid artery
*Mann–Whitney Wilcoxon test
†Fisher's exact test
rSO2 and ΔrSO2(%) at baseline, preclamp, first minute after clamp and fifth minute after clamp in the NS and S groups
rSO2, regional oxygen saturation; SD, standard deviation
Concerning the baseline to one minute after clamp interval, a positive, first-order linear association between ΔrSO2(%) and SP was documented (equation 1: ΔrSO2(%) = 0.22 × SP − 21.94; P = 0.013 for the coefficient of SP; Figure 1a). The subsequent addition of a second-order term yielded significant results also; thus, the association between ΔrSO2(%) and SP follows a quadratic pattern (equation 2: ΔrSO2(%) = −0.006 × SP2 + 1.164 × SP − 53.02; P = 0.018 for the second-order coefficient and P = 0.005 for the first-order coefficient; Figure 1b). The third-order approach did not lead to a significant third-order coefficient. The predicted maximum corresponds to a value of SP equal to 91.6 mmHg, where the predicted ΔrSO2(%) is equal to +0.26% (nearly equal to zero). The application of the SP = 40 mmHg value at equations (1) and (2) yielded ΔrSO2(%) = −13 and −16% values, respectively. These values have been retained for evaluation at the ROC analysis.

(a) First-order association between ΔrSO2 and SP during baseline – 1 minute after clamp (ΔrSO2 [1 minute] = rSO2 1 minute after clamp − rSO2 baseline/rSO2 baseline). (b) Second-order association between ΔrSO2 and SP during baseline – 1 minute after clamp (ΔrSO2 [1 minute] = rSO2 1 minute after clamp − rSO2 baseline/rSO2 baseline). SP, stump pressure; rSO2, regional oxygen saturation
Regarding the fifth minute after clamp, the results were in line with those derived from the first minute. The first-order linear association between ΔrSO2(%) and SP persisted (equation 3: ΔrSO2(%) = 0.18 × SP − 19.45; P = 0.036 for the coefficient of SP; Figure 2a). The second-order approach revealed again the quadratic pattern (equation 4: ΔrSO2(%) = −0.006 × SP2 + 1.025 × SP − 47.23; P = 0.035 for the second-order coefficient and P = 0.013 for the first-order coefficient; Figure 2b). The third-order approach did not lead to a significant third-order coefficient. The predicted maximum corresponds to a value of SP equal to 90.28 mmHg where the predicted ΔrSO2(%) is equal to −0.95% (i.e. once again very close to zero). For SP = 40 mmHg, ΔrSO2(%) = −12 and −16% values were estimated using equations (3) and (4), respectively. Once again, these values have been retained for evaluation at the ROC analysis.

(a) First-order association between ΔrSO2 and SP during baseline – 5 minutes after clamp (ΔrSO2 [5minutes] = rSO2 5minutes after clamp − rSO2 baseline/rSO2 baseline). (b) Second-order association between ΔrSO2 and SP during baseline – 5 minutes after clamp (ΔrSO2 [5 minutes] = rSO2 5 minutes after clamp − rSO2 baseline/rSO2 baseline). SP, stump pressure; rSO2, regional oxygen saturation
Using ROC analysis, in baseline to one minute after clamp interval, ΔrSO2(%) ≤ −21% was identified as an optimal cut-off point (Figure 3), while ΔrSO2(%) ≤ −16% scored below the maximum Youden's index. For comparison, the evaluation of various criteria published in the literature, according to the results of ROC analysis derived from this study, is presented in Table 3. The results of ROC analysis in the case of the baseline to five minutes after clamp interval are shown in Table 4. A ΔrSO2(%) ≤ −10.1% was yielded as optimal but the alternative optimal cut-off (ΔrSO2(%) ≤ −19.3%) provided a similar Youden's index being, however, in favor of higher specificity (Figure 3). The values derived from the first order and quadratic approach scored below the maximum Youden's index. The detailed results underlying the three criteria that emerged at ROC analysis have been provided in the form of 2 × 2 tables in Table 5; the evaluation of the ΔrSO2(%) criteria using Fisher's exact test revealed significant results (P < 0.001) which are in agreement with the ROC findings, as expected.
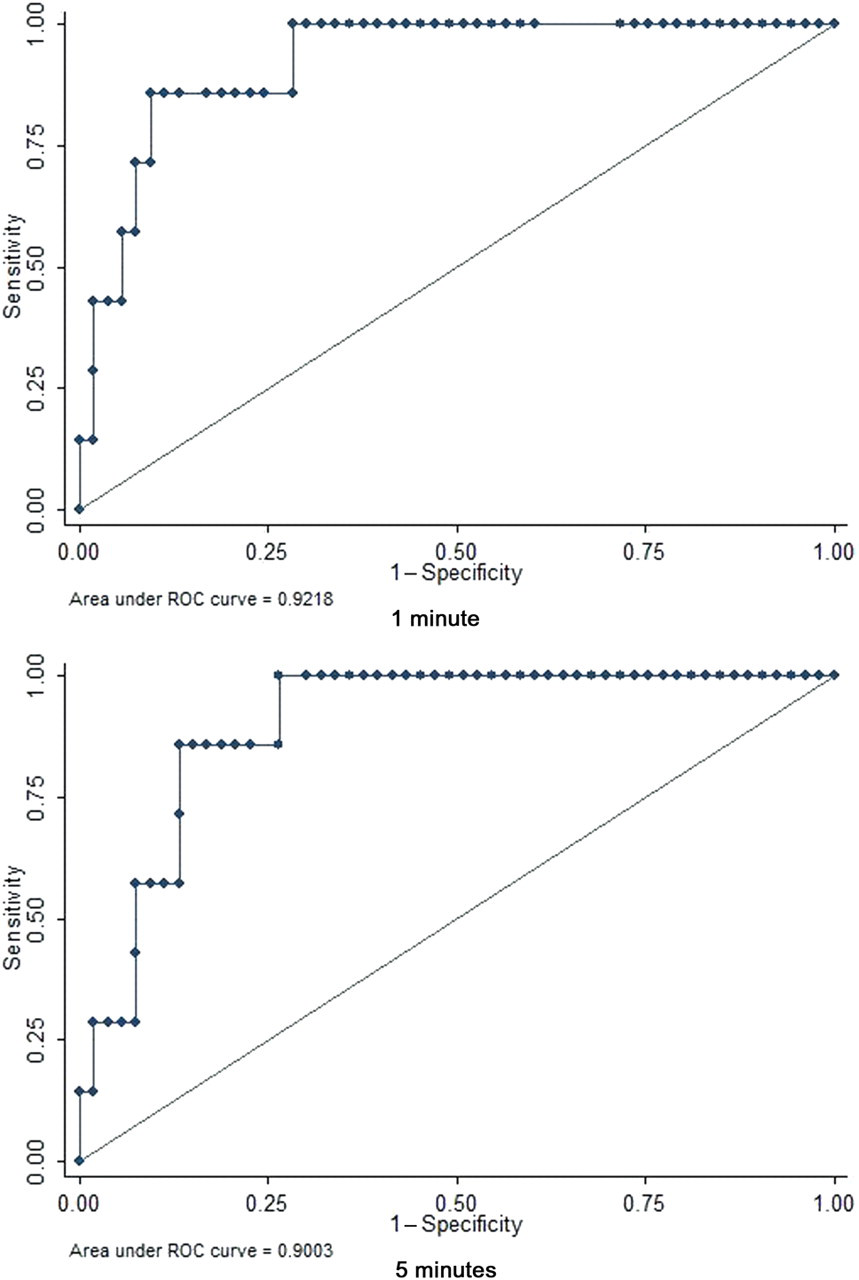
Receiver operating characteristic curves regarding the baseline to first and fifth minutes after clamp intervals
Evaluation of ΔrSO2(%) criteria according to the results of receiver operating characteristic analysis derived from this study
CEA, carotid endarterectomy; EEG, electroencephalography; SSEP, somatosensory evoked potential; TCD, transcranial Doppler ultrasound; SP, stump pressure
The criteria are presented in ascending order
*Youden's index corresponds to the maximum value of (sensitivity + specificity − 1) 38
ΔrSO2(%) criteria derived by receiver operating characteristic analysis regarding the baseline to five minutes after clamp interval
The criteria are presented in ascending order
rSO2, regional oxygen saturation
Detailed 2 × 2 results underlying the three cut-off points that were yielded by receiver operating characteristic analysis
rSO2, regional oxygen saturation
Discussion
The association between ΔrSO2(%) and SP describes the correlation between oxygen saturation at the ipsilateral hemisphere and SP values. Concerning the baseline to one minute after clamp interval, the ΔrSO2(%) − SP association seems to follow a quadratic pattern. The first-order analysis regarding the correlation between ΔrSO2(%) and SP revealed significant results. However, the evaluation of a second-order term was also significant and outperforms the first-order association. The quadratic curve shown in Figure 1b could be schematically divided into two sections: section A (relatively low values of SP, ΔrSO2(%) below the maximum point) and section B (high SP values). Section B most likely represents a plateau; in other words the quadratic model implies that no significant increase in ipsilateral ΔrSO2(%) values is observed after SP reaches 91.6 mmHg. This pattern seems to reflect the underlying properties of cerebral oximetry in describing cerebral oxygenation in patients who do not require shunt insertion, since high SP values reflect adequacy of blood supply to the brain; as a result, no significant change in oxygen saturation is expected. On the contrary, section A denotes a parallel change in ΔrSO2(%) and SP values prior to the plateau. In other words, the lower the SP values, the more pronounced the decrease in ΔrSO2(%).
The ROC analysis revealed that the distinction between shunted and not shunted patients was best provided by the ΔrSO2(%) ≤ −21% threshold regarding the baseline to one minute after clamp interval. This result is in agreement with the 20% threshold usually reported in the literature 4–7 as critical for development of cerebral ischemia during cross-clamping, even though there are also studies concluding to other cut-off points. 26–28,34–37 The ΔrSO2(%) values derived from the first order and quadratic approach did not exhibit optimal cut-off properties. For the optimal interpretation of the results it should be kept in mind that the regression modeling and ROC analysis represent two distinct statistical entities; the regression modeling procedure aims to estimate values with a certain degree of prediction (probabilistic error), 39 whereas ROC analysis provides a data-driven approach. Nevertheless, it is worth noting that the quadratic approach was rather closer to the result of the ROC analysis when compared with the first-order estimation. As mentioned above, the optimal cut-off in our study is in line with the one demonstrated in previous studies (Table 3). Specifically, Pugliese et al. 4 reported a sensitivity of 100% and a specificity of 100% for the ΔrSO2(%) < −20% criterion. Similarly, Botes et al. 7 reported also a very satisfactory sensitivity (100%) and specificity (87%) for the same threshold comparing cerebral oximetry with electroencephalography and Samra et al. 5 reported a sensitivity of 80% and a specificity of 82.2%. It should be noted that these three studies, as well as the studies that found other cut-off points, used different monitoring methods and methodological sequence than this study in calculating the ΔrSO2(%) (Table 3). This fact might explain the discrepancies in results. Factors such as the time point considered as baseline, the comparative monitoring method and the measurement procedure probably affect the outcomes and are discussed in this text.
As shown in Table 3, the ΔrSO2(%) ≤ −21% criterion has a sensitivity of 85.71%. The clinical interpretation of this finding is that if shunting was based exclusively on this criterion, about 86 of 100 patients developing intraoperative cerebral ischemia would have been shunted correctly while 14 out of 100 patients needing a shunt would not have one inserted. In addition, the specificity of 90.57% of this criterion means that among 100 patients who did not require shunt insertion, only nine would have been shunted unnecessarily. These rates are high in comparison to the results of the other studies demonstrated in Table 3.
An aspect of the present study that seems to merit commenting is the notion of baseline. As evidenced in Table 3, published studies set preclamp rSO2 values as baseline. Nevertheless, the 20% criterion emerged as a reliable threshold irrespectively of the nature of baseline. According to a recent review article, it has been recommended that the baseline values should be determined before inducing general anesthesia. 6 The rationale underlying this recommendation takes into account the wide patient to patient variability of baseline rSO2 values and seems, thus, to provide a more reliable measurement. Indeed, individual circulatory reactions to surgical and pharmaceutical interventions made after the induction of anesthesia may contribute to the modulation of the preclamp value. 25,40 For example, the lower preclamp rSO2 values in the S group in this study point to an already modified value at this step of the procedure prior to the oncoming hypoperfusion (Table 2). Consequently, the preclamp rSO2 values do not obligatorily reflect true baseline data.
Regarding the baseline to five minutes after clamp interval, the results were consistent with those at the first minute. However, in this case the distinction between shunted and not shunted patients was provided by the ΔrSO2(%) ≤ −10.1% criterion; the ΔrSO2(%) ≤ −19.3% threshold provided similar results but lower sensitivity and higher specificity. Studies on larger samples are needed to clear which criterion for shunting outperforms as the operation and the ipsilateral cerebral ischemia go on.
A technical aspect of this study that should be discussed pertains to the measurement procedure per se. In the present study, one value of rSO2 was obtained at each time point and rSO2 change was found based on the comparison between specific measurements of specific time points. However, other studies 5,26,36 have adopted the comparison of mean preclamp and after clamp rSO2 measurements for the definition of the critical threshold. Yet, realtime calculation of mean values may be impractical, whereas a simple observation of ΔrSO2(%) values, as provided by the spectrometer at specific time points, seems much more applicative during the operation.
The results of this study demonstrate the potential ability of cerebral oximetry to replace SP, a time-honored technique, 41 in brain monitoring during CEA. Cerebral oximetry seems to be at least as reliable as SP in detecting patients at risk of cerebral ischemia, but it also has the advantage of providing continuous, realtime, direct evidence of brain oxygenation. The 21% criterion could essentially contribute to the detection of patients needing shunt insertion intraoperatively, timely and trustworthily using a non-invasive method. The constant, non-invasive evaluation of anesthetized patients provided by near-infrared spectroscopy allows the appropriate interventions (for example, adjustment of arterial pressure or partial pressure of carbon dioxide) 40 in order to avoid neurological damage during the cross-clamping period. Furthermore, the ability of cerebral oximetry to detect early postoperative complications, such as acute carotid thrombosis in the recovery room, should be studied.
This study bears certain limitations that should be acknowledged. The major weakness of this study pertains to the fact that the study sample size was relatively small and no neurological events were observed in any patient in this cohort, while only seven patients required a shunt. The categorization of patients was based solely on shunt insertion for SP ≤40 mmHg, and this limits the extrapolation of the present findings upon studies where the decision for shunting is based on other criteria (such as SP <25 mmHg or <50 mmHg in patients with contralateral occlusion). 41 Nevertheless, statistically significant findings emerged at the regression analysis. This may point to the reproducibility of the present findings in larger studies.
In conclusion, a quadratic association between the % cerebral oxygen saturation changes, measured by near-infrared spectroscopy, and SP was demonstrated by this study. A ΔrSO2(%) ≤ −21% cut-off point during the baseline to one minute after clamp interval was revealed as the equivalent of the SP ≤ 40 mmHg criterion for selective shunting. There is a potential ability of cerebral oximetry to replace SP in brain monitoring during CEA. Studies on larger samples are warranted in order to further investigate the properties and criteria applicable in the context of cerebral oximetry during CEA.
Footnotes
Acknowledgments
Financial disclosure of authors and reviewers: none reported.