
Abstract
Inferior vena cava (IVC) thrombosis at its hepatic portion (also known as obliterative hepatocavopathy [OH]), in the absence of systemic or local diseases such as vasculitis, coagulopathy, infection and malignancy, is a rare event. We report the case of a 25-year-old woman with progressive abdominal pain and leg edema after exercise. Imaging showed congestive liver and IVC occlusion at the intrahepatic portion. A liver biopsy demonstrated portal congestion without evidence of fibrosis; after unsuccessful percutaneous attempts for recanalization, consideration was given to liver transplantation with IVC reconstruction versus IVC bypass. Due to the presence of preserved liver function, an externally supported 16-mm ringed polytetrafluoroethylene graft was used to bypass from the suprarenal IVC to the suprahepatic IVC. At five years, she remains symptom-free, with normal liver function and a patent graft on systemic anticoagulation. This report highlights the successful surgical management of a patient with OH with a thick membrane. It supports other published proposals that this entity differs significantly from classic Budd–Chiari syndrome with thrombosis that affects only the hepatic veins and, thus, OH should be approached and managed differently.
Keywords
Introduction
Thrombosis at the hepatic portion of the inferior vena cava (IVC), in the absence of systemic or local diseases such as vasculitis, coagulopathy, infection and malignancy, is a rare event. Although it has been classified as a form of Budd–Chiari syndrome (BCS) (hepatic vein outflow tract obstruction), primary thrombosis of the IVC, also known as membranous occlusion of the IVC (MOVC), 1 may represent a different disorder from the ‘classic BCS’ with hepatic vein thrombosis.
MOVC is more common in the far east, with the majority of BCS cases being caused by this entity. 2 Until recently, MOVC was regarded as a congenital vascular anomaly, but the etiology is now considered to be a membranous sequelae of IVC thrombosis commonly occurring in the hepatic portion. 1 In 1998, Okuda et al. 3 proposed the term ‘obliterative hepatocavopathy’ (OH) to designate this clinical entity and emphasized that this disorder should be clinically distinguished from BCS with hepatic vein thrombosis. Angioplasty with stenting or surgical membranotomy can be performed if the obstructive lesion is thin, 4–6 while various surgical shunts such as cavoatrial and mesoatrial bypasses have been described to treat thicker occlusions. 6,7
We report a case of a 25-year-old woman with complete occlusion of the intrahepatic portion of the IVC that was successfully treated with a polytetrafluoroethylene (PTFE) venous bypass from the infrahepatic to the suprahepatic portion of the IVC.
Case report
A previously healthy 25-year-old Caucasian woman presented with new onset of right-side abdominal pain, early satiety and mild lower extremity edema that worsened after exercise or prolonged upright position. These symptoms progressed over three months. Hepatosplenomegaly was noted upon physical examination. Of note, as a child she had a progressive growth in her abdominal wall that was resected five years prior to presenting to our institution. She reported that this growth was thought to be a varix. Her past medical, family and social histories were non-contributory and her liver function was normal. She underwent a computed tomography (CT) scan and a magnetic resonance imaging of her abdomen that showed diffuse nodularity throughout her liver, along with splenomegaly. The portal vein was patent, as was the IVC below the liver. The majority of the intrahepatic IVC was not visualized as well as the hepatic veins due to caudate lobe hypertrophy. The IVC was patent suprahepatic to the level of the right atrium. Large collateral veins were present in the retroperitoneum and in the paraspinous area. These findings were interpreted as veno-occlusive disease in the intrahepatic portion of the IVC. A subsequent venocavagram confirmed the IVC obstruction and demonstrated venous drainage from the caudate lobe into the patent portion of the intrahepatic IVC; also, contrast could be injected through the short hepatic veins filling into the liver parenchyma (Figures 1a–c). Contrast injection via the right internal jugular vein demonstrated abrupt interruption of the IVC and the absence of hepatic outflow at that level due to complete occlusion of the hepatic veins (Figures 2a and b). Percutaneous attempts at re-canalization from the right internal jugular and right femoral veins were unsuccessful. Ultrasound-guided percutaneous liver biopsy demonstrated portal congestion but no evidence of severe fibrosis. Consideration was given to liver transplantation with an IVC reconstruction or an IVC bypass; however, with preserved liver function and limited fibrosis, the decision was made to proceed with a venous bypass of this obstructed IVC.
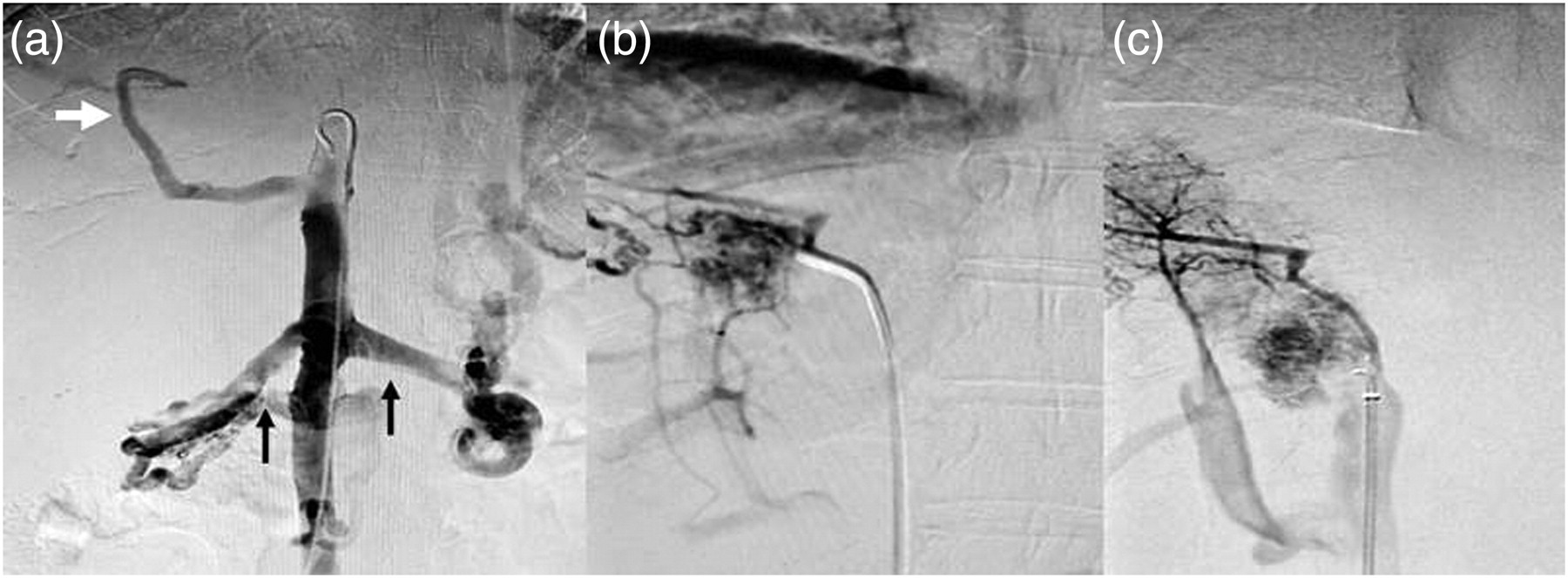
(a) Ascending venocavagram shows the IVC occlusion and a vein (white arrow) from the caudate lobe that appeared to drain into the patent portion of the intrahepatic IVC. Renal veins (black arrows) and retroperitoneal collaterals can also be observed. (b) and (c) Contrast is injected through short hepatic veins filling into the liver parenchyma. IVC, inferior vena cava
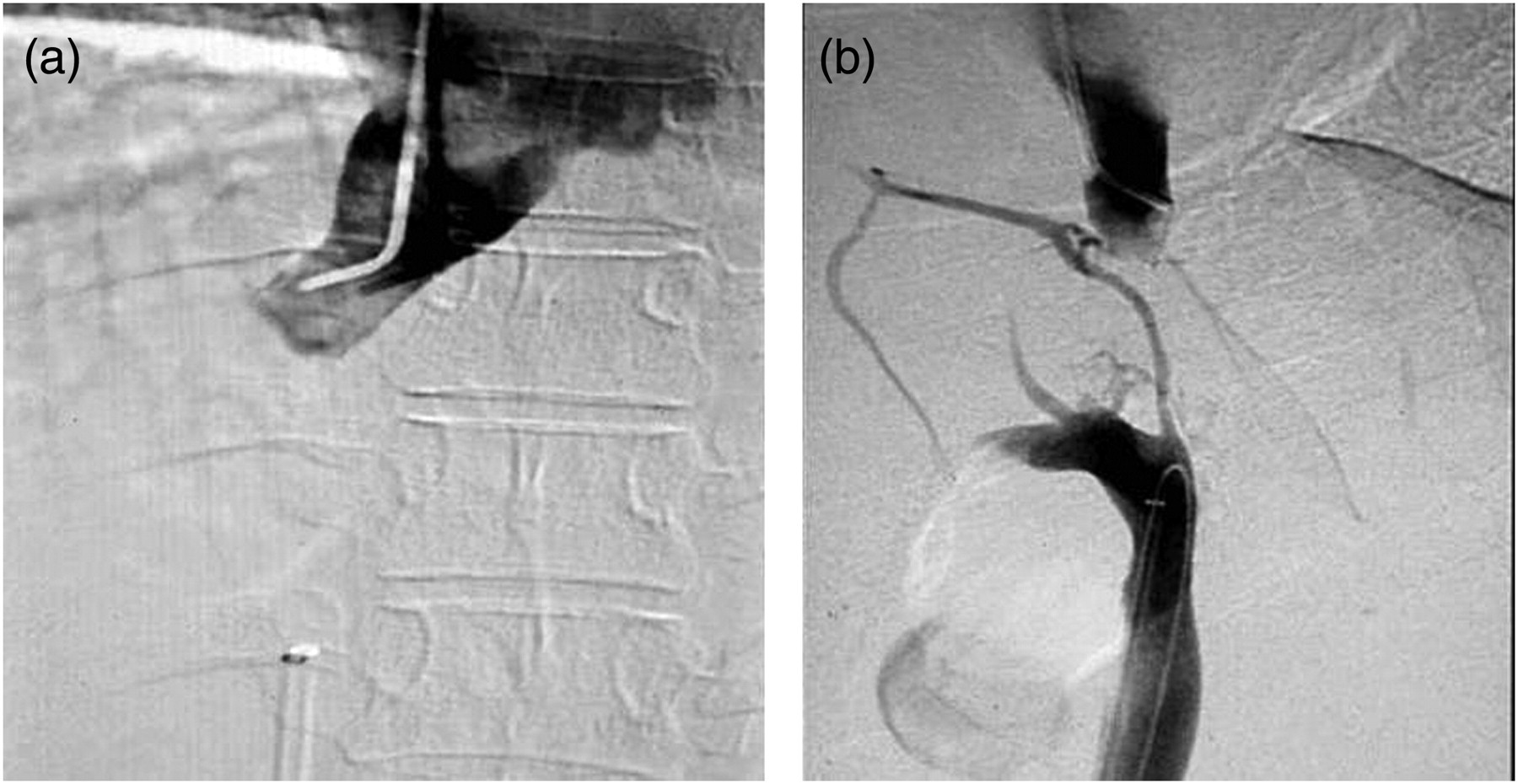
(a) Contrast injection via the right internal jugular vein demonstrated abrupt interruption of the suprahepatic IVC and the absence of hepatic outflow at that level due to complete occlusion of the hepatic veins. (b) Contrast from above and below showed the occluded segment in the intrahepatic portion of the IVC and intrahepatic collaterals. Percutaneous attempts for re-canalization were unsuccessful. IVC, inferior vena cava
A right thoracoabdominal incision was made through the seventh intercostal space. The IVC was exposed immediately under the liver between the renal veins and just above the diaphragm. An externally supported 16-mm ringed PTFE graft was selected and an end-to-side anastomosis was performed to the IVC above the diaphragm. Following this, an end-to-side anastomosis was performed down to the suprarenal portion of the IVC (Figure 3). A completion venogram was performed and demonstrated good contour of both anastomoses (Figures 4a and b). A liver biopsy was also performed and a chest tube was placed. The patient was fully anticoagulated. Intraoperatively, the biopsy report showed marked fibrosis, sinusoidal dilation and congestion around the central veins. She was transferred to the surgical ICU for close monitoring and on the second postoperative day was transferred to the floor and started on heparin, which was subsequently converted to enoxaparin and coumadin. The chest tube was removed on postoperative day 3. A liquid diet was started on postoperative day 2 and successfully advanced, and the patient was discharged home on postoperative day 10. The patient was followed with periodic duplex imaging, and CT demonstrated graft patency (Figures 5a and b). Four years later, the patient decided to become pregnant. During the course of her pregnancy she was switched to low molecular weight heparin and no obstetric complications occurred. At five years she remains asymptomatic, a liver function test remained normal, recent magnetic resonance angiography revealed a patent graft on systemic anticoagulation and she has not required re-interventions (Figure 6).

Intraoperative photograph. A right thoracoabdominal incision was made through the seventh intercostal space; the IVC was exposed immediately and a 16-mm ringed polytetrafluoroethylene graft was selected and an end-to-side anastomosis was performed onto the IVC above the diaphragm. The diffuse nodular hepatic parenchymal process can be observed. IVC, inferior vena cava
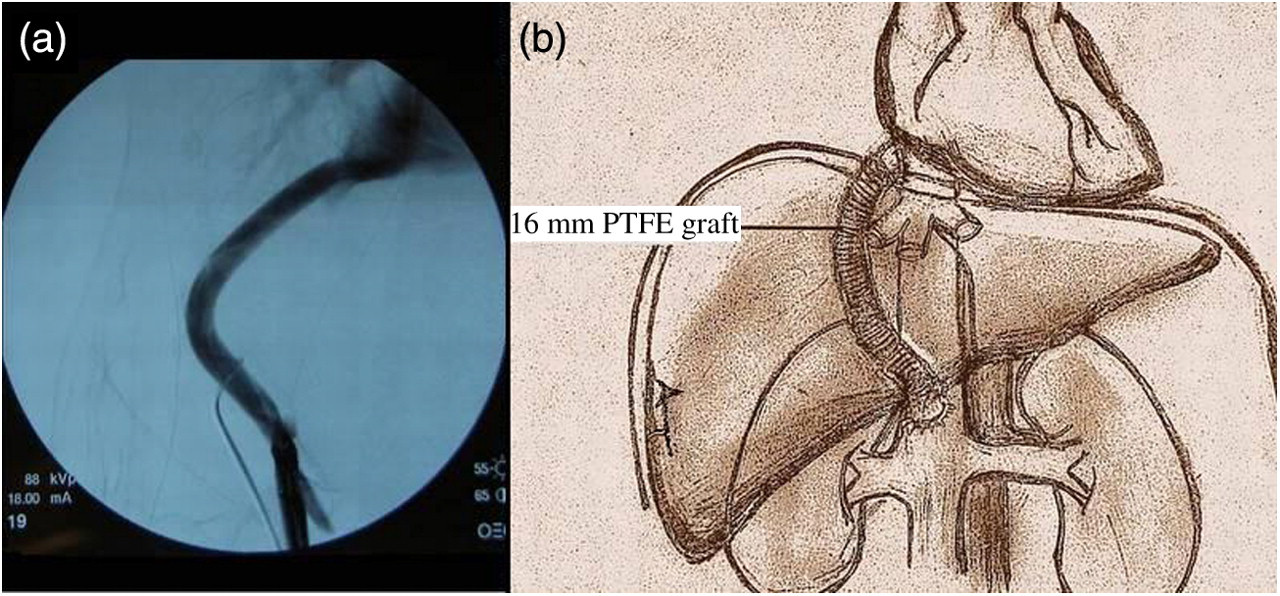
Postoperative venogram (a) demonstrated graft patency. (b) Schematic drawing of the configuration of the 16-mm polytetrafluoroethylene bypass graft
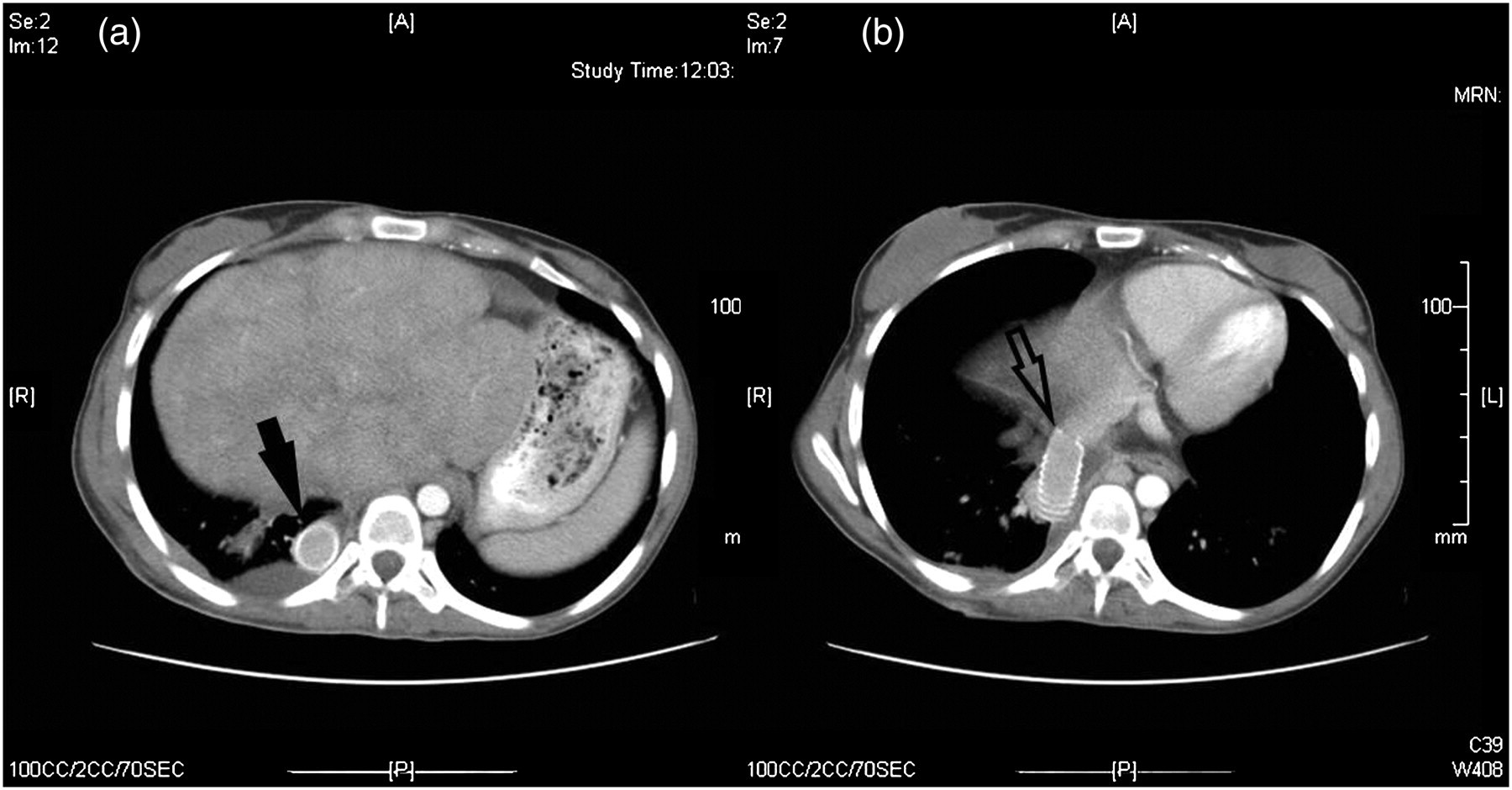
Computed tomography scans at two different levels. (a) Scan at the intrahepatic portion of the IVC and (b) at the polytetrafluoroethylene graft anastomosis in the suprahepatic portion of the IVC. The graft has been patent for five years after the surgery. IVC, inferior vena cava
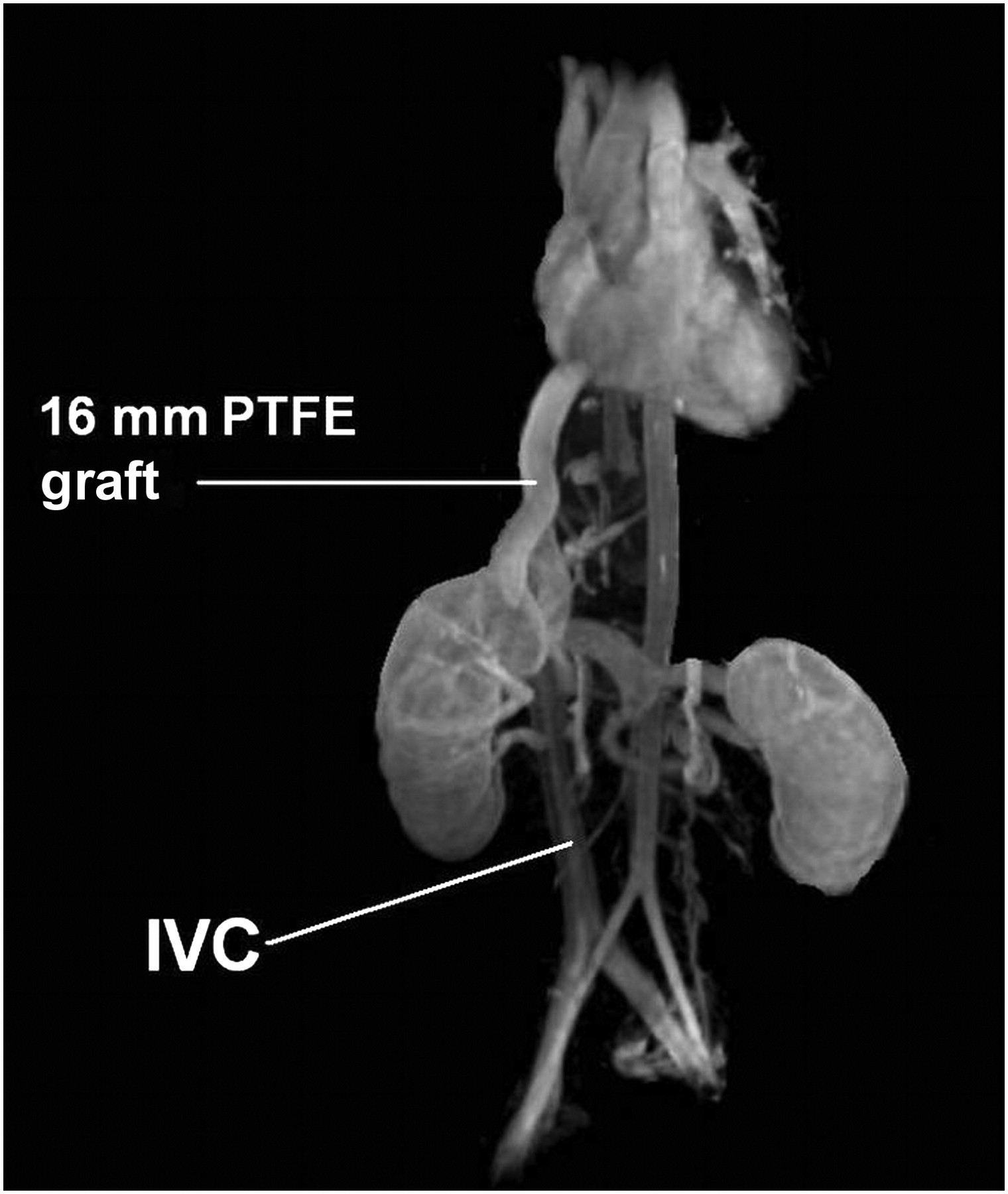
Magnetic resonance angiography three-dimensional re-construction at five years demonstrated the patency of the 16-mm PTFE bypass graft. IVC, inferior vena cava; PTFE, polytetrafluoroethylene
Discussion
Numerous terms have been used in the medical literature to denote the occluding lesion in the hepatic portion of the IVC: coarctation, congenital stenosis or occlusion of the IVC in its diaphragmatic portion, membranous stenosis, and fibrous constriction of the IVC, partial BCS and congenital MOVC. 2 The term ‘membranous’ was first used in 1950 by Bennet 8 and many authors have subsequently used it. The true etiology has not been well established because the differential diagnosis of primary hepatic vein thrombosis and IVC thrombosis is difficult. 2 Further studies suggest that IVC occlusive disease is different from hepatic vein thrombosis (classic BCS), which usually presents acutely at any age with abdominal pain, hepatomegaly, ascites and jaundice. In contrast, the former generally presents with less severe symptoms with dilation of the truncal subcutaneous veins when the ascending lumbar vein becomes the major collateral route. 3 The hepatic vein orifices are affected to varying degrees, resulting in congestive liver damage. Cirrhosis may develop after a long clinical course that may be complicated by hepatocellular carcinoma. 1
A number of researchers concluded that many of these entities involving the intrahepatic IVC were congenital vascular anomalies. However, others do not support this theory of IVC stenosis. The histopathological studies by Parker 9 and Kage 10 demonstrated that the occluding changes along the IVC were the result of the organization of a thrombus.
IVC thrombosis of the hepatic portion is uncommon in Western, developed countries. In classic BCS, a number of hypercoagulable conditions are demonstrable, such as coagulation factor deficiency, mutation, myeloproliferative disorders, paroxysmal nocturnal hemoglobuinuria, anticardiolipin antibodies, oral contraceptive use and pregnancy, as well as thrombosis-related disorders, Behcet's disease, sarcoidosis, connective tissue disease or vasculitis. In OH or primary IVC thrombosis, thrombotic states may be found, but the majority of patients have no demonstrable hypercoagulability, as is the case with our patient. 1 The interesting question is why a thrombus forms preferentially in the hepatic portion of the IVC. The theory proposed by Kretz 11 explains that the intima of the IVC is mechanically and microscopically damaged by the movements of the diaphragm and thus prone to thrombosis. An additional mechanism favoring this theory is the presence of eddying blood currents in this portion of the IVC, where the hepatic veins join the IVC at a right angle. 3
Case reports and small series describe several types of cavoatrial bypasses for thick lesions, but to our knowledge, there is no previous report of a bypass from the infrahepatic to the suprahepatic IVC. In their series, Kieffer et al. 12 reported their experience with six patients. Five had patent bypasses by interposition grafts with a mean follow-up of 28 months after surgery. Wang reported the largest series to date on membranous occlusion of the vena cava, with 12 patients. Treatment entailed placement of cavoatrial Dacron bypasses; 13 nine of the patients had improvement during a median follow-up of 1.5 years. In 1992, Gloviczki et al. published a series of 28 venous reconstructions, including thoracic and infradiaphragmatic veins, and concluded that the spiral saphenous vein is a good conduit for SVC bypass; however, the outcomes were disappointing for IVC reconstructions, with 43% of the patients requiring reinterventions and only 29% of veins remaining patent at two years. Seven of 11 patients with abdominal or pelvic PTFE bypass had patent grafts after a mean follow-up of nine months. 14 Nine years later, the same group from the Mayo Clinic reported two cavoatrial bypass grafts, one with PTFE and one spiral vein graft; the PTFE graft was patent at one year and the spiral graft occluded at three months. 6 Endovascular techniques represent the first line of therapy for non-malignant IVC occlusion of the veins; stenting has demonstrated higher technical success and patency rates than percutaneous transluminal angioplasty alone. Razavi reported a technical success of 88% in his series of 17 patients with IVC occlusion with a primary patency of 80% at 19 months. 15 Robbins et al. 16 reported two cases with unrelenting lower extremity venous hypertension in whom a rapid improvement was achieved with relief of chronic IVC by means of stenting, and Thompson et al. 17 described a successful endovascular treatment of OH and renal vein thrombosis; suprarenal IVC stenting was performed with Wallstents (18 mm × 4 mm and 20 mm × 80 mm; Boston Scientific, Natick, MA, USA) to the level of the stenosis and the patient remained asymptomatic two years after the procedure.
In our patient, occlusion of the IVC at the hepatic portion and complete occlusion of the hepatic veins manifested as progressive enlargement of abdominal subcutaneous veins, liver congestion and mild lower extremity edema exacerbated after physical activity; however, liver function remained normal throughout her course. Our approach was influenced by the anatomy of the lesion. The caudate lobe drained blood into the patent portion of the intrahepatic IVC and then into retroperitoneal collaterals; therefore, a bypass graft was placed from the infrahepatic portion of the IVC, just above the renal veins, to the supra-diaphragmatic portion of the IVC, providing better drainage of the remaining hepatic outflow, and also allowing continuous blood flow to the right atrium from the lower half of the body (Figure 7). This report highlights successful surgical management of a patient with OH with a thick membrane. It also supports the proposal that this entity differs clinically from classical BCS with hepatic vein thrombosis and should be approached and managed in a different manner.
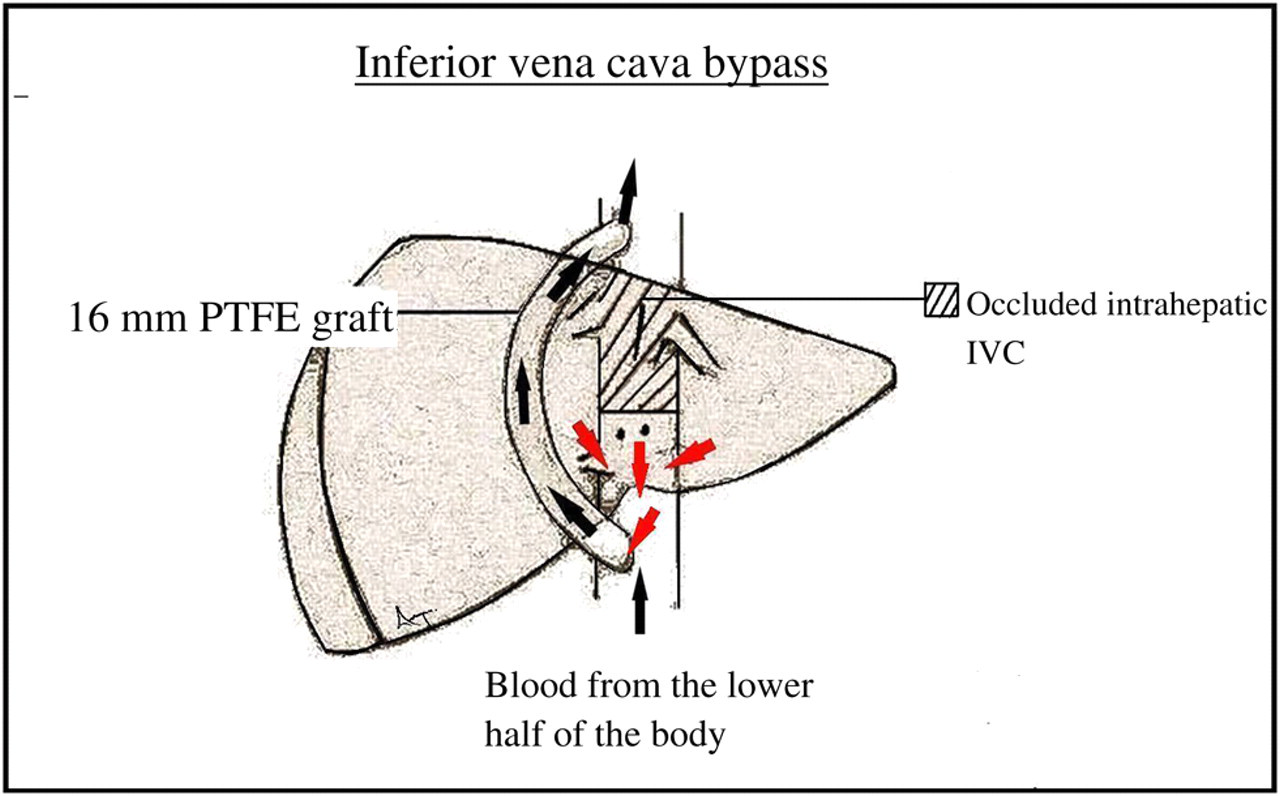
Diagram illustrates hemodynamics after the IVC reconstruction. The IVC and hepatic veins were occluded. The caudate lobe drained blood into the patent portion of the intrahepatic IVC (red arrows) through a major collateral and the short hepatic veins. The surgical approach was influenced by the anatomy of the lesion; therefore, a bypass graft was placed from the suprarenal IVC, to the supra-diaphragmatic portion of the IVC, providing better drainage of the remaining hepatic outflow, and also allowing continuous blood from the lower half of the body (black arrows). IVC, inferior vena cava; PTFE, polytetrafluoroethylene
Footnotes
Acknowledgments
The authors thank Nyla Ismail PhD and Daynene Vykoukal PhD for critical reading of the manuscript.
Financial disclosure of authors and reviewers: none reported.