
Abstract
Pyoderma gangrenosum (PG) is an uncommon and frequently misdiagnosed inflammatory dermatosis. This neutrophilic inflammation of the dermis has been well described in relation to other inflammatory illnesses (i.e. inflammatory bowel disease). Although rare, PG is increasingly described in relation to trauma or surgical interventions. It is important for vascular surgeons to be aware of the potential development of PG at vascular access sites. Although endovascular surgery is a minimally invasive form of vascular surgery, it does require cutaneous manipulation, which can incite PG. The purpose of this report is to describe a case of PG that developed after an attempted endovascular surgery and to elucidate this rare dermatologic disorder's diagnosis and treatment.
Case report
In September 2009, an 80-year-old man with a past medical history significant for vascular co-morbidities (i.e. hypertension, diabetes, coronary artery disease, etc.) and a recent diagnosis of rheumatoid arthritis underwent an attempted endovascular repair of a 6.5-cm descending aortic aneurysm. After an attempt was made to access the patient's femoral arteries via cut down exposure, it was apparent that the patient had extensively calcified and tortuous femoral and iliac vessels. This finding was surprising to the operative team. A month prior, the patient underwent imaging of the aneurysm via computed tomography aortogram with three-dimensional reconstructions that noted both modest infra-renal calcifications and normal caliber lumens. Our patient's endovascular procedure was terminated without additional imaging because it was felt that passage of endovascular devices through his particularly extensively calcified and brittle arterial entry sites would subject the patient to unnecessary distal emboli and require substantial vascular reconstruction. He was scheduled for an open procedure at a later date.
Three days later, the patient presented to the emergency department for evaluation of pain, swelling and redness along bilateral inguinal incision sites. The patient was admitted from the emergency department and started on broad-spectrum antibiotics for presumed cellulitis. On hospital day 2, due to increased erythema and tenderness extending to the symphysis pubis and scrotum bilaterally, the closed wounds were electively opened at bedside. The clear fluid expressed was sent for culture and later grew minimal pan-sensitive Streptococcus species consistent with contaminant. Wound dressings were scheduled three times daily. The next day, the wound demonstrated mild necrosis of underlying fat pads, ulceration and skin slough in a scalloped pattern along the wound edges (Figures 1a and b). The constellation of these symptoms and progressively increasing leukocytosis to >30,000 prompted immediate operative debridement.
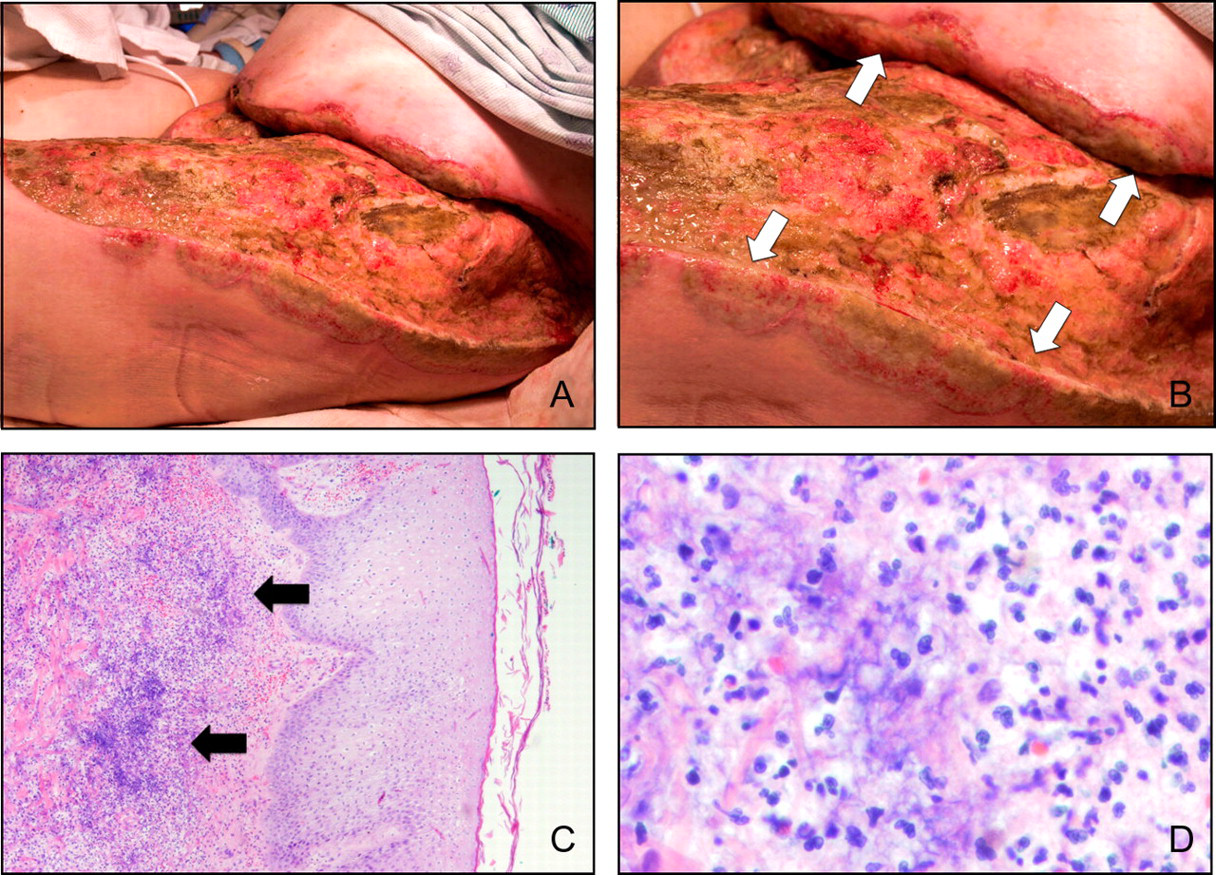
A) The patient's wound after debridement. B) A closer detail of the wound, demonstrating skin slough and separation from the underlying fascia in a scalloped pattern along the wound edges, highlighted by white arrows. C) Histologic examination of tissue biopsies revealing an ulcerated epidermis with marked neutrophilic infiltration. The infiltration is highlighted by black arrows and involves both the epidermis and dermis – ×4 magnification of hematoxylin and eosin (H&E) stained section. D) Closer magnification of neutrophilic infiltration – ×40 magnification of H&E stained section.
In the operating room, fat necrosis, fascial separation and superficial skin slough was found well beyond the original operative site. Debridement was carried back to healthy bleeding tissue. Cultures were taken and tissue samples were sent to general pathology, which confirmed an overwhelming infiltration of inflammatory cells along the fascia and dermal components. The debridement required exposure of the patient's femoral arteries, which were subsequently covered by local muscle advancement flaps.
Postoperatively, the patient continued to have elevated leukocytosis (i.e. >22,000), despite the debridement and broad-spectrum antibiotics. Two days later, intraoperative cultures revealed no organisms and the patient once again demonstrated evidence of skin slough in a scalloped pattern along the wound. With the working diagnosis of necrotizing fasciitis, the patient returned to the operating room again for a more extensive debridement. This cycle of skin ulceration, slough and separation prompting debridement occurred once more despite changes in antibiotic therapy, silver impregnated dressings and negative pressure therapy. The patient was even given a brief antibiotic holiday of 24–36 hours after prior therapies did not demonstrate resolution. The patient's local skin slough continued at the same rate. Histological review of the biopsy specimens by a dermatopathologist revealed that the patient had an ulcerated epidermis with marked neutrophilic infiltration of both the epidermis and dermis (Figures 1c and d); however, there was no apparent vasculitis. These findings and multiple negative culture results throughout the patient's hospital course shifted the working diagnosis from necrotizing fasciitis to the neutrophilic dermatosis, pyoderma gangrenosum (PG).
The patient was given high-dose systemic intravenous corticosteroids to treat PG. Systemic therapy, compared with topical therapy alone, carried a more substantial risk of worsening his condition if the diagnosis was incorrect. However, it was felt by both the patient's family and health-care team that the patient's developing morbidities (i.e. respiratory failure, atrial flutter and renal failure) warranted an immediate therapeutic response rather than one that may take up to seven days for clinical effect. The patient responded favorably to immunosuppression (within 48 hours) and had no further development or recurrence of skin ulceration during his hospitalization. Once he was stabilized from a cardiopulmonary standpoint, he was then able to begin a four-week stepwise process of wound closure. Of note, during his entire hospital course, the patient's vessels were well protected by his muscle flaps. He retained adequate bilateral lower extremity perfusion as evidenced by distal palpable pulses, brisk capillary refill and the ability to heal skin grafts.
Discussion
Today endovascular surgery is a minimally invasive form of vascular surgery with several therapeutic uses. While the complications associated with endovascular surgery are typically less severe than those associated with traditional vascular surgery, they do exist. 1 The complications commonly described thus far include, but are not limited to, pseudoaneurysm, laceration, occlusion, hematoma, arterial venous fistula, arterial embolism, arterioduodenal fistula and infection. This case report describes a potentially morbid complication to the exposure and groin access required to perform complex endovascular stenting procedures.
PG is a dermatosis defined clinically by the presence of recurrent ulcers with either mucopurulent or hemorrhagic exudates. The peak incidence of PG occurs between the ages of 20–50, and women are more frequently affected than men. Although its etiology is unknown, several diseases have been associated with PG. For example, inflammatory bowel diseases (IBDs) such as Crohn's disease and ulcerative colitis (up to 10–15%) display the dermatosis. 2 Due to its association with IBD, cross-reacting antigens in the bowel and skin are believed to be responsible for disease manifestation. Circulating hyperglobulinemia, interleukin-8 overexpression and aberrant neutrophil trafficking with resulting insufficient epidermal protection have all been implicated in its pathogenesis. 3–6 It has also been associated with various hematological malignancies, hepatitis, seronegative rheumatoid arthritis, spondylitis and monoclonal gammopathies. 7 Other diseases that must be included in the differential diagnosis include necrotizing fasciitis, vascular occlusive disease, vasculitis, cancer, infection (sporotrichosis, late syphilis, erysipelas, herpes), exogenous tissue injury and drug reactions.
In about 20–50% of patients, PG is known to exhibit pathergy, which is the development of new lesions or aggravation of pre-existing ones due to trivial trauma. 6,8 As a result, operative incisions, biopsies, skin testing and even needle sticks can all create new lesions. Pathergy may also explain why autologous skin grafts are rejected and new lesions develop in the donor site. As such, PG has been reported as a complication in various types of surgery including coronary artery bypass graft surgery, laparoscopic appendectomy, knee arthroscopy, lower extremity vascular bypass, abdominoplasty, skin grafting, breast reconstruction and free tissue transfer flaps. 4,9–15 Within the past year, over 100 articles have been published describing the disease and its treatment. The increasing body of case reports within the literature demonstrates a growing awareness that PG can be associated with virtually any cutaneous manipulation regardless of how minimally invasive the procedure is perceived.
PG and necrotizing fasciitis often have similar clinical presentations. It is careful clinical management that delineates the two processes and leads to successful treatment outcomes. For example, one could argue that our patient had necrotizing fasciitis and that his microbiology culture results could have been skewed since the patient had been on antibiotics. Of note, the mainstay treatment for necrotizing fasciitis is debridement and not antibiotic therapy alone because capillary beds adjacent to the disease process thrombose, preventing antibiotic penetration into the infected tissue. Our patient had been on antibiotics and underwent both extensive debridement and frequent dressing changes. His initial wound cultures were essentially negative and subsequent wound cultures did not grow any organisms. However, skin along his wound edges continued to serially slough despite being debrided back to healthy bleeding tissue. The patient even had an antibiotic ‘holiday’ to evaluate the confounding diagnosis. In fact, the patient's skin slough did not improve until the addition of immunosuppression. Although it is possible that the etiology for this case could be infectious in nature, it is unlikely considering his course would have dramatically worsened with either an antibiotic holiday or immunosuppression therapy. Instead, he improved. No additional biopsies were taken after corticosteroid treatment. His clinical improvement inferred that a correct diagnosis and treatment were ultimately found.
There is no currently described means to prevent PG. As such, it is important to identify which vascular patients are prone to develop PG, how to diagnose it and ultimately how to treat it. Vascular patients are particularly challenging as they represent a population of individuals who typically have many co-morbidities. Early identification starts with a knowledge of the patient's pre-existing conditions that increase their tendency for immune reaction (e.g. IBD, rheumatoid arthritis, spondylitis, etc.). The diagnosis is essentially clinical and can be supported by biopsy. In fact, it is a diagnosis of exclusion. PG has been reported to occur on various body sites, but most typically appears in the lower legs, especially the pretibial area. 16 The ulcers typically appear to have bluish borders and surrounding erythema. The ulcer begins as a follicular pustule that rapidly grows and leads to tissue necrosis. The surrounding skin then becomes erythematous, edematous and painful. 17 There are no specific laboratory parameters or circulating antibodies that identify PG. Patients will typically demonstrate laboratory findings consistent with systemic inflammation such as elevated erythrocyte sedimentation rate, leukocytosis and C-reactive protein. Cultures should be taken from wound exudates or by direct tissue biopsy, if possible. Histopathology findings are typically non-specific and include a deep suppurative folliculitis with a rich neutrophilic infiltration without microvascular involvement. Early involvement by dermatopathologist may direct the diagnosis.
There are several modalities to treat PG. Treatment typically begins with local wound care and controlling associated intestinal disease. 18 Topical treatments such as concentrated corticosteroids, cromolyn sodium solution and 5-aminosalicylic acid have fewer systemic side-effects, but may take longer to reach clinical effect. 16 Pulsed corticosteroids are the most well described and typically display clinical improvement in 1–2 days. 19 Generally, 0.5–2 mg/kg/day of oral prednisone (or equivalent) are given and tapered off as clinical condition improves. The exact treatment course is variable depending on clinical response. As prolonged courses with steroids result in many unwanted side-effects, treatment regimens with other immunomodulating medications such as cyclosporine, and mycophenolate mofetil, thalidomide, azathioprine, tacrolimus, cyclophosphamide, chlorambucil, tumor necrosis factor-alpha (TNF-alpha) inhibitors and intravenous immune globulin have been developed. 20–24 Miller et al. 25 recently reviewed the evidence behind these expanding treatment modalities. Poor prognostic indicators include male gender, older age at onset and bullous PG associated with hematologic malignancy. 26 Mortality has been reported to be up to 18% at 26 months in some series. 2
Conclusions
In the rapidly expanding field of endovascular therapies, it is important for the vascular surgeon to be aware of the potential development of PG after minimal cutaneous manipulation. This case report demonstrates that PG, albeit rare, is a potential devastating surgical complication at vascular access sites. As there is no means to prevent PG, early clinical suspicion with a thorough clinical workup, including tissue biopsy reviewed by a dermatopathologist, are paramount in approaching this disease. Fortunately, an increasing number of immunosuppressive therapies are available to treat it. Vascular surgeons should be aware that immune dysfunction (i.e. seronegative rheumatoid arthritis in our case) places patients at an increased risk for developing PG, and they can treat this potential surgical morbidity if they employ both a systematic and a multidisciplinary approach to the problem.
Footnotes
Acknowledgments
Financial disclosure of authors and reviewers: none reported.