
Abstract
Endovascular repair for ruptured abdominal aortic aneurysm has demonstrated superior results when compared with open repair and will likely become the standard of care when the anatomy of the aneurysm is appropriate for endovascular repair.
Keywords
Introduction
Endovascular repair for ruptured abdominal aortic aneurysm (AAA) has demonstrated superior results when compared with open repair and will likely become the standard of care when the anatomy of the aneurysm is appropriate for endovascular repair. 1–5
We present a case of ruptured AAA managed by endovascular repair followed by laparotomy to ligate an internal iliac artery to prevent retrograde endoleak and thrombin injection into the sacs of the common iliac artery aneurysm and AAA to achieve complete thrombosis of the sacs. To the best of our knowledge, this is the first description of a hybrid repair of ruptured AAA with the use of thrombin for acute treatment of type II endoleaks.
Case report
GM is an 83-year-old man who presented with abdominal pain and back pain. A computed tomography (CT) angiogram showed the presence of a ruptured infrarenal AAA with blood in the retroperitoneum (Figure 1).

Computed tomography scan showing ruptured abdominal aortic aneurysm with blood in the retroperitoneum
The patient was hypotensive with a systolic blood pressure in the 70s but with normal mental status, normal renal function and no evidence of myocardial infarction. There was a 3.0-cm neck to the large AAA, and both the common iliac arteries and the left internal iliac artery were aneurysmal (Figure 2). A left-sided aortouniiliac repair using a 28-mm device, the Talent model (Medtronic, Minneapolis, MN, USA), was performed. The repair was extended into the external iliac artery across the orifice of the internal iliac artery using an iliac extender limb. The decision was made not to coil embolize the left internal iliac artery prior to extending the endograft into the left external iliac artery due to the patient's hemodynamic instability. A 24-mm occluder plug was placed in the contralateral common iliac artery and a femoral–femoral bypass graft was performed.

Intraoperative angiogram demonstrating infrarenal abdominal aortic aneurysm, bilateral common iliac aneurysms and left internal iliac aneurysm
A completion angiogram showed opacification of the aorta and common iliac artery aneurysm sacs. This could represent a type IV endoleak due to the porosity of the fabric, which would resolve in time or could represent a retrograde endoleak from the large internal iliac artery aneurysm with refilling of both the common iliac artery and AAA sacs (Figure 3a). It was thought that it would be prudent to assume the latter, and since the patient had a ruptured AAA, we proceeded to correct this.
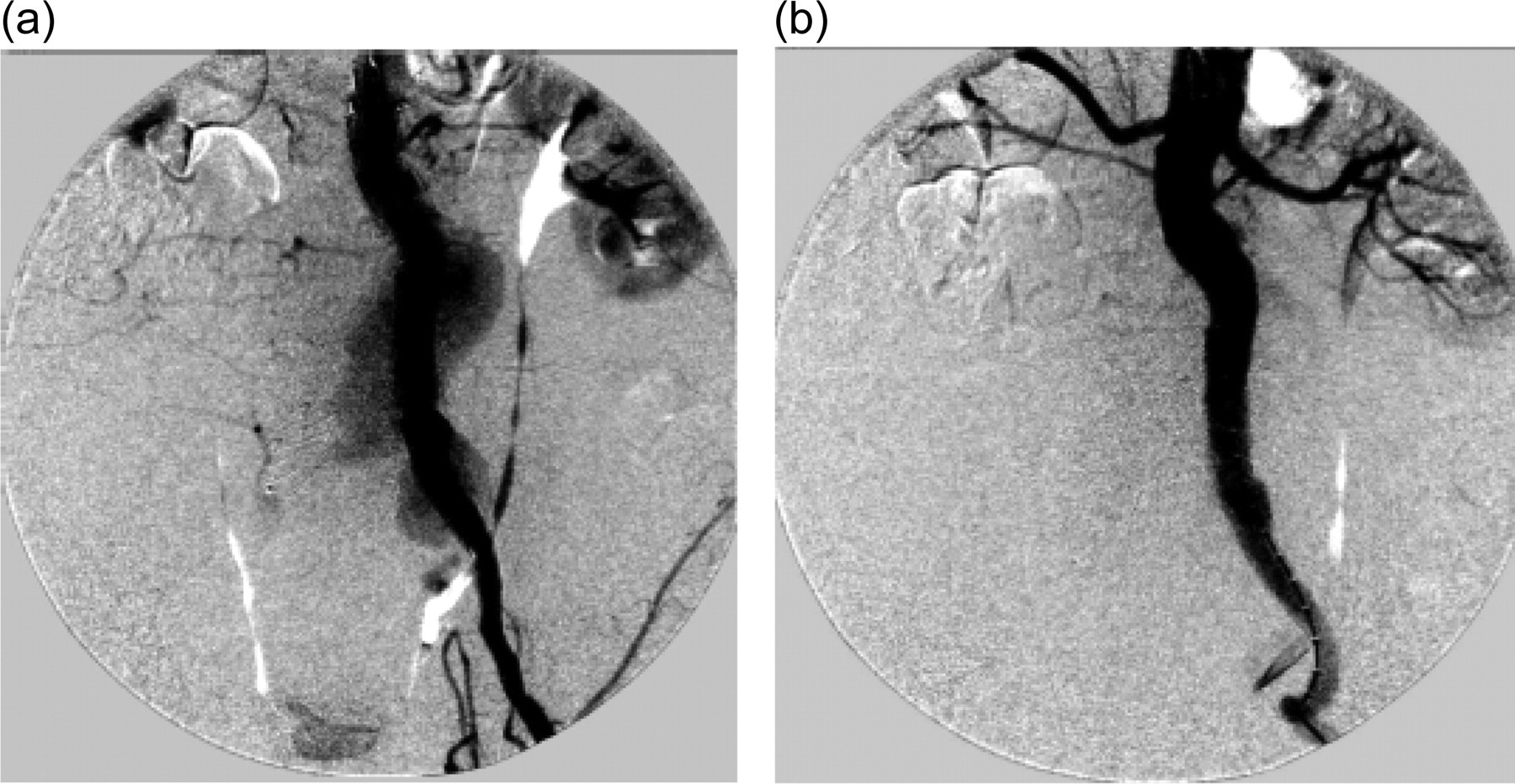
(a) Aortouniliac repair with type II endoleak. (b) Without endoleak
A laparotomy was done to ligate the origin of the internal iliac artery with permanent suture material. Under ultrasound guidance, 2.0 mL of bovine thrombin (1000 units/mL; King Pharmaceuticals, Middleton, WI, USA) was injected into the common iliac artery aneurysm and 2.0 mL was injected into the AAA sac (with minimal pressure on the plunger of the syringe containing the thrombin), achieving complete thrombosis of the sacs with no evidence of endoleak (Figure 3b). To note, care was exercised while injecting thrombin into the anterior segment of the aorta and common iliac aneurysm sacs, staying away from the lumbar vessels. Then, the inferior mesenteric artery was ligated and blood was evacuated from the retroperitoneum and peritoneal cavity and the abdomen closed.
The subsequent postoperative course was uneventful, and he was discharged to a skilled nursing facility on postoperative day 13 in good condition. The patient was seen at three-month follow-up and found to be doing well. An ultrasound examination of the repair demonstrated no endoleak and gross shrinkage of the sac (Figure 4). A CT angiogram was not performed on account of modest renal insufficiency.
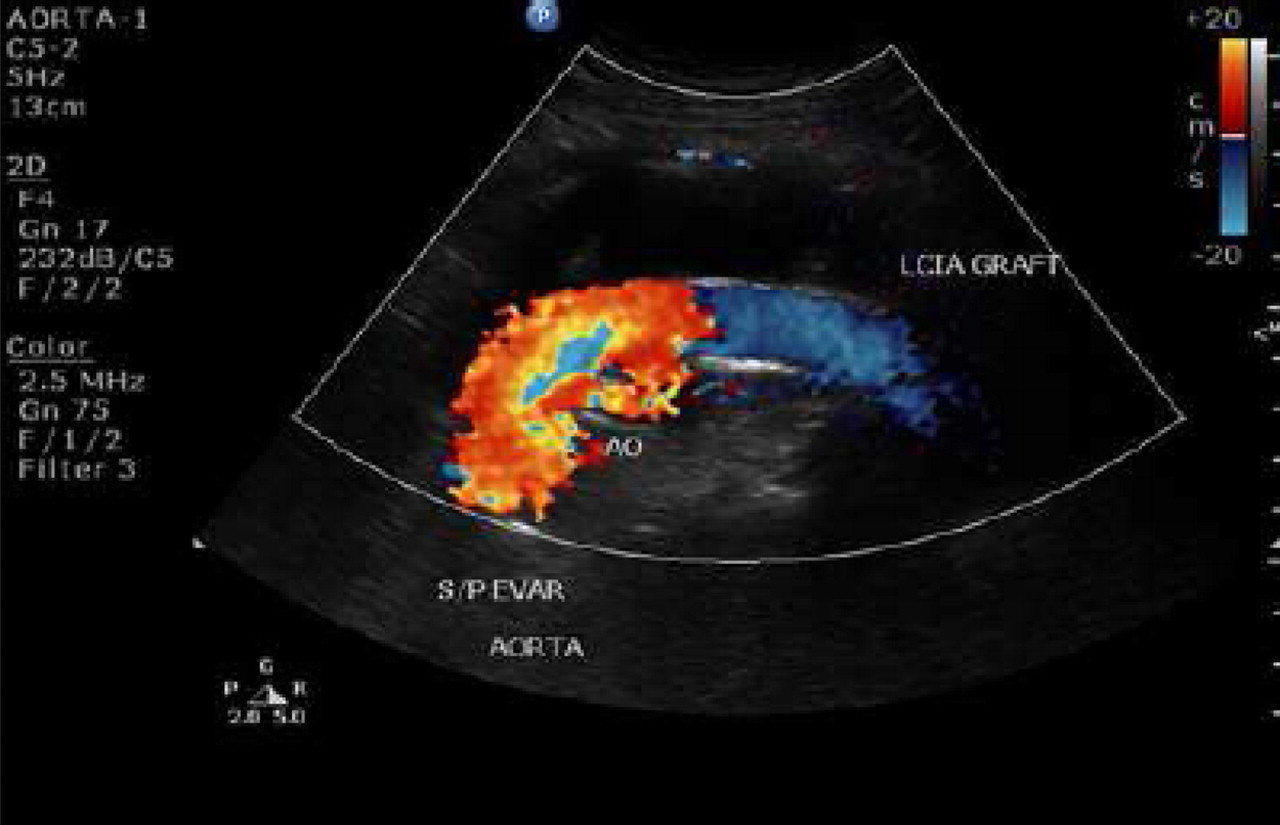
Three months' postoperative ultrasound showing exclusion of aneurysm with no endoleak
Discussion
At our institution, we follow a definitive protocol in the management of ruptured AAA. From the time a potential ruptured AAA is suspected, a ‘code vascular’ is called. This activates the entire vascular team, including the operating room with endovascular capabilities. The patient undergoes a quick CT scan with contrast, obtaining 2.5-mm cuts to determine if the anatomy is favorable for endovascular repair. Depending upon the stability of the patient and quality of the access vessels, either a standard aortobiiliac repair or an aortouniiliac repair with an occluder plug in the contralateral common iliac artery, followed by a femoral–femoral bypass graft, is performed.
The downside of endovascular aneurysm repair (EVAR) for aneurysm repair is the problem of endoleak. Getting a seal at the attachment sites both proximal and distal is paramount in obtaining a satisfactory repair.
Type II endoleaks can also be a potential problem, as the ruptured sac may allow ongoing bleeding and blood loss. The need for laparotomy to address these issues, as well as to prevent abdominal compartment syndrome, is a vitally important component of the management paradigm.
Type I endoleaks following elective EVAR have been treated by placing extender cuffs, bare-metal stents or balloon molding, or all of the above. When these maneuvers are unsuccessful, catheter-based procedures (glue and coil deposition) and open repair have been used.
Maldonado et al. 6 reported the following success rate in resolving type I endoleaks for elective EVAR during postoperative follow-up: using n-butyl cyanoacrylate (92.3%), extender cuff (80%), and coil with or without thrombin (75%). These, however, are time-consuming interventions and not quite appropriate for the management of ruptured AAA.
Lu et al. described a success rate of 97.6% for sealing type I endoleaks using fibrin glue for embolization. A mean of 15 ± 10 mL of glue was required to obtain a seal, which appeared to be durable over the longer-term follow-up. Balloon occlusion of the proximal aorta was done during glue injection. 7
Concerns with the use of thrombin or fibrin glue to treat type I endoleaks include outflow vessel embolization, including the inferior mesenteric artery and lumbar arteries leading to colon or spinal cord ischemia or infarction, thrombosis of the aorta and recurrence of endoleak over the longer term.
Thrombin is widely used to induce thrombosis in pseudoaneurysms at all locations. Thrombin and fibrin glue have also been injected into AAA sacs under CT or ultrasound guidance during elective procedures in order to seal type II endoleaks. 8–12
Ultrasound-guided injection into a large AAA and left common iliac artery aneurysm sac lowers the risk of inadvertent injury to the endograft, as has been reported in the case of CT-guided injection. 13 Thrombin injection under realtime ultrasound guidance can limit the volume of the drug necessary to induce thrombosis. By injecting the medication under low pressure in the anterior segment of the sac, this may lower the possibility of the drug entering the lumbar vessels, which could result in spinal cord ischemia.
Conclusion
Patients presenting with ruptured AAA tend to have challenging anatomy for EVAR. A hybrid approach with the above-mentioned adjunct procedures is likely to produce improved results in the challenging patient cohort. To our knowledge, this is the first report of successful management of a patient with ruptured AAA by EVAR, with subsequent open ligation of the internal iliac artery and thrombin injection into the sac to resolve type II endoleaks.