
Abstract
The use of prosthetic grafts in below-knee bypasses may be necessary in patients with no available autologous vein and critical limb ischemia not amenable to angioplasty. Such conduits, however, have generally yielded disappointing results. A new, heparin-bonded, expanded polytetrafluoroethylene graft (Gore Propaten vascular graft) designed to provide resistance to thrombosis may be associated with decreased early graft failure and increased patency. A concern with exposure to heparin, and therefore heparin-bonded prostheses, is the development of heparin-induced thrombocytopenia (HIT). Although rare, this requires prompt graft removal. We present a case to highlight this serious complication and review the literature on this topic.
Introduction
Femoral–tibial saphenous vein grafts, with primary patency rates of up to 69% and secondary patency rates of 85% at five years, 1 are the conduits of choice to perform bypasses to small distal arteries in the lower extremity. When greater saphenous or alternate veins are not available, prosthetic grafts have been used for distal bypasses in selected patients. However, these grafts are less durable with five-year patency rates of <50%, 2 motivating attempts to improve patency by vein cuffs and patches, arteriovenous fistulas and by pretreatment of prosthetic grafts with heparin. The results of infrainguinal bypass with a heparin-bonded graft have demonstrated improved patency compared with standard prostheses. 3,4 It therefore appears to be an appropriate conduit choice for lower extremity bypass when an autologous vein is unavailable. A concern with the use of heparin-bonded prostheses is the development of heparin-induced thrombocytopenia (HIT) in a patient who undergoes insertion of such a prosthetic.
We report a case of HIT that developed in a patient in association with implantation of a heparin-bonded, expanded polytetrafluoroethylene (ePTFE) graft for infrainguinal revascularization and review some of the lessons which can be learned regarding the management of this surgical rarity.
Case report
A 92-year-old woman presented with rest pain and dry gangrene affecting the hallux of the left foot with visible bone. There were no palpable pulses at, or distal to, the left groin, and the ankle brachial pressure index was 0.46. Her medical history included hypertension, hyperlipidemia, diabetes and mild renal impairment. There was no previous history of vascular intervention or exposure to heparin. A computed tomography angiogram showed severe common and external iliac disease, and occluded femoral, superficial femoral and proximal popliteal arteries. The posterior tibial artery was the only crural vessel to remain patent across the ankle. On preoperative venous mapping, she was found not to have any suitable autogenous conduits and in view of her extensive disease was not a candidate for endovascular treatment.
Therefore, she underwent an urgent left axillofemoral bypass with profundaplasty using a 7-mm Dacron graft, and a profunda (graft hood) to tibio-peroneal trunk bypass using a heparin-bonded 6-mm ePTFE graft (Propaten, W L Gore and Associates, Flagstaff, AZ, USA). Intraoperative unfractionated heparin (5000 IU) was given intravenously prior to vessel clamp application. The hallux was amputated at the end of the procedure. Surgery was uneventful and the patient made a good early recovery. Despite graft patency determined by duplex, her foot began to deteriorate on postoperative day 6 with progression of the wound in the presence of a cyanotic appearance. Routine blood analysis revealed a progressive thrombocytopenia (Figure 1). A provisional diagnosis of HIT was made. Deep vein thrombosis (DVT) prophylaxis with subcutaneous enoxaparin (40 mg) was ceased and intravenous argatroban was commenced at 1 µg/kg/min as a continuous infusion, with dosing rate adjusted to maintain the activated partial thromboplastin time at 1.5–3 times baseline (day 8). A HIT assay confirmed the diagnosis of HIT. Platelet factor 4-heparin IgG antibodies were detected by enzyme immunoassay (1.95 optical density units [positive result, 0.45 optical density units]). In addition, the patient's serotonin release assay demonstrated 94% serotonin release at 0 U of heparin per mL, 100% serotonin release at 0.2 U of heparin per mL and 0% serotonin release at 100 U of heparin per mL.
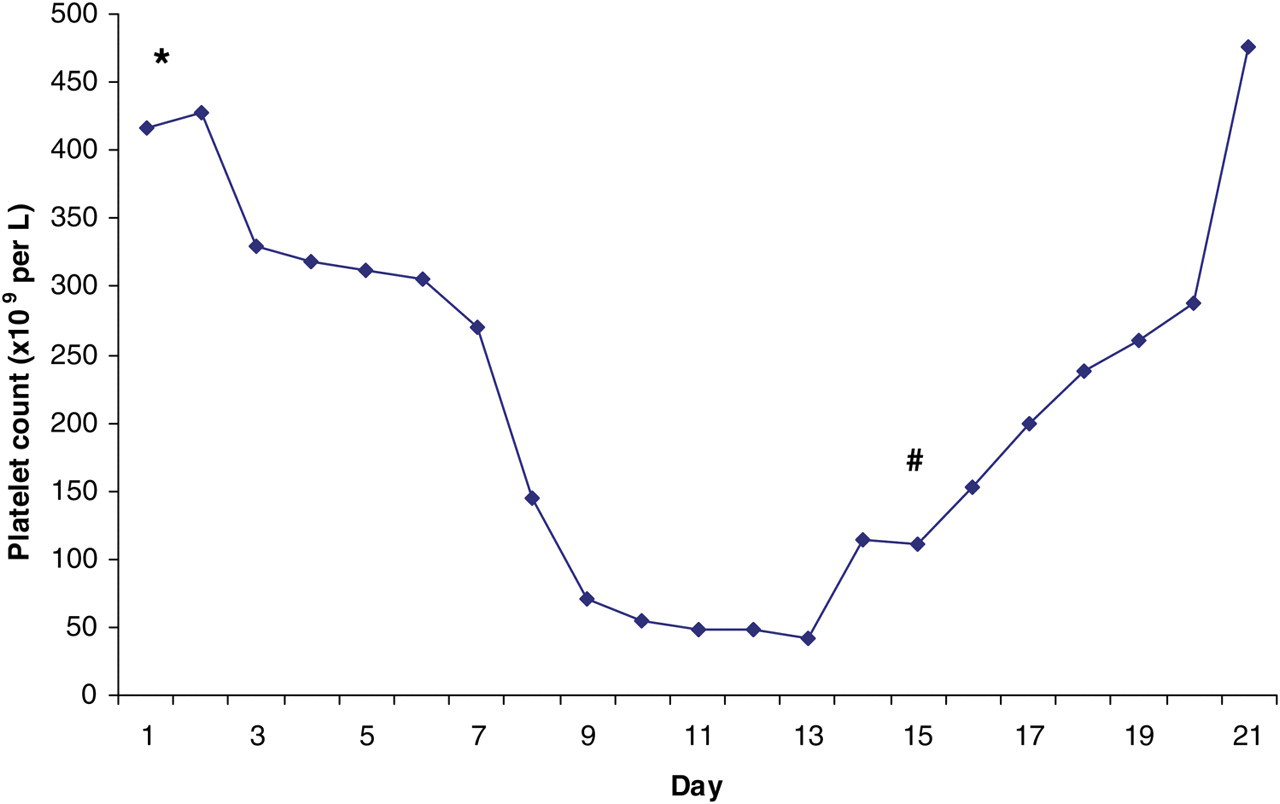
The trend in the patient's platelet count is shown in relation to graft insertion (*), treatment of heparin-induced thrombocytopenia and graft explant(#)
The platelet count reached a nadir of 42 of 11 × 103/μL five days postcommencement of argatroban. Despite anticoagulation and patent bypass grafts, the wound edges of the amputation site became progressively necrotic along with extension along the plantar aspect. It was felt that the heparin bonding of the Propaten graft may have been an ongoing stimulus to the immune reaction of HIT and on postoperative day 15, the patient underwent left above knee amputation and complete removal of the Propaten graft. Intraoperatively, the graft was well incorporated with no evidence of gross clot in the graft. The platelet count recovered quickly on removal of the graft. Warfarin therapy was initiated and argatroban ceased once the international normalized ratio was therapeutic. The patient then made a slow but uneventful recovery with no significant wound complications.
Discussion
Autologous vein has been shown to have superior long-term patency rates for infrainguinal bypass compared with prosthetic conduits despite various adjunctive procedures such as vein cuffs or patches (Trans-Atlantic Inter-Society Consensus [TASC] 5 II). Frequently, however, vein is unavailable, either being used previously or too diseased. The use of prosthetic grafts for infrainguinal bypass procedures is therefore not uncommon and has fueled the search for a prosthetic graft with superior patency rates.
The Gore Propaten graft is an ePTFE graft with unfractionated heparin covalently bonded to the luminal surface through a proprietary endpoint attachment mechanism (Carmeda® BioActive Surface [CBAS®]; Carmeda, Upplands, Vãsby, Sweden), which serves to anchor heparin molecules to the luminal surface while still maintaining heparin's intrinsic bioactive properties. 6 Endpoint covalent bonding is a unique concept that allows the anticoagulant properties of heparin to be applied directly on the graft surface. The end of each heparin molecule is bonded to the luminal surface, allowing the heparin active site to freely interact with antithrombin. This produces a persisting antithrombotic tendency within the graft without significant systemic release of heparin. Graft explants from an in vivo canine model demonstrated sustained heparin bioactivity over a period of 12 weeks. 6 It has been shown to achieve patency rates superior to those of standard prosthetic grafts and is therefore an attractive conduit for use in those lacking a suitable vein. 3,4
One to three percent of all patients exposed to heparin can develop the severe complication of HIT. HIT is defined as a >50% decrease in platelet count while receiving unfractionated (UFH) or low molecular weight heparin (LMWH) in association with HIT antibody formation. 7 Type 1 HIT is a mild, non-immune reaction that may not be recognized if platelet counts are not routinely monitored. Type 2, by comparison, can be life-threatening. This immune-mediated reaction typically occurs 4–10 days after initial heparin exposure in 1–3% of all patients exposed to UFH and up to 0.8% in patients receiving LMWH. 8 It is due to an immune-mediated reaction caused by heparin in which platelet-activating IgG antibodies are formed against platelet factor 4 bound to heparin. The IgG antibodies cause excessive platelet activation with resulting thrombosis of large veins and arteries and also the microcirculation. 9
Factors influencing the risk of developing HIT in order of importance include: duration of heparin use (increased risk with longer duration), type of heparin (lower risk with LMWH), patient population (surgical > medical > pregnant women) and sex (females at increased risk). 10 DVT and pulmonary embolism are, by far, the commonest complications of HIT, particularly in postoperative patients, followed by arterial thrombosis in limbs, cerebral and myocardial circulations, with resulting acute limb ischemia, stroke and myocardial infarction, respectively. Limb loss rates have been quoted as 20% and mortality rates of 30%. 11 HIT is treated by ceasing all heparin products and commencing anticoagulation with a non-heparin alternative such as the direct thrombin inhibitors argatroban or lepirudin.
It is uncertain whether heparin covalently bonded to the luminal surface of a graft has the same antigenic properties as heparin in solution, and thus whether heparin-bonded grafts can continue to drive HIT after cessation of all other forms of heparin. Heyligers et al. 12 studied blood samples drawn from patients with heparin-bonded bypass grafts and compared them with samples from patients with a standard graft of the same material. In vivo markers of platelet activation and coagulation parameters were no different between groups and heparin antibodies were not detected, thus suggesting that heparin-bonded grafts have no systemic heparin effect. However, this study was underpowered if one accounts for the relatively low incidence of HIT. Conversely, in vitro studies show that heparin-bonded grafts do elute heparin and that this caused platelet aggregation when exposed to plasma from HIT-positive patients. The possibility of sensitizing patients to heparin leeching from a heparin-bonded graft with the activation of platelets and secondary thrombosis strongly suggests that heparin-bonded grafts be used with great caution. 13,14 In addition, other authors have linked heparin-coated pulmonary artery catheters with cases of HIT 15 and one group has reported a case in relation to a heparin-bonded graft. 16
When deciding to implant a heparin-bonded graft, deliberation may be given to the avoidance of administration of perioperative subcutaneous and intervenous fractionated and unfractionated heparin to avoid the scenario described here. Bivalirudin, a direct thrombin inhibitor, is an alternative for this role. Some advantages of direct thrombin inhibitors are that they do not require antithrombin as a co-factor, they are not inhibited by platelet factor and do not activate platelets, there is no cross-reactivity with HIT antibodies, they raise the activated clotting time in a dose-dependent manner and are convenient to use. 17 It is, however, an expensive medication and has primarily been used for anticoagulation during percutaneous transluminal coronary angioplasty.
Conclusions
While the possibility of HIT developing as a result of Propaten graft implantation appears to be low, we advise the close monitoring of the patient's platelet count postoperatively. Patients with heparin-coated grafts who have thrombocytopenia should be tested for the presence of heparin-associated antiplatelet antibodies. If HIT is confirmed, heparin should be discontinued and treatment with a direct thrombin inhibitor initiated. In addition, if symptoms persist or the health of the patient appears compromised, strong consideration must be given to the removal of the heparin-bonded graft if the thrombocytopenia is to be reversed and complications avoided.
Footnotes
Acknowledgments
Financial disclosure of authors and reviewers: none reported.