
Abstract
A significant percent of patients undergoing endovascular abdominal aortic aneurysm repair (EVAR) have concomitant common iliac artery aneurysms. While most of these patients will tolerate sacrifice of the hypogastric artery during repair, a subset will develop sequelae of hypogastric occlusion. EVAR was performed in two patients using a bifurcation-sparing unibody endograft (Powerlink, Endologix, Irvine, CA, USA). To avoid simultaneous bilateral hypogastric occlusion, one side was treated with coil embolization while the other was treated with a hypogastric graft (Viabahn, W L Gore and Associates, Flagstaff, AZ, USA). Access to the preserved hypogastric artery was obtained from a sheath inserted from the contralateral femoral artery and brought over the aortic bifurcation with the assistance of a ‘rail-wire’ traversing from the contralateral to ipsilateral femoral sheaths. The hypogastric limb was deployed simultaneously with the ipsilateral external iliac limb extension, creating a double-barrel flow lumen preserving both hypogastric and external iliac flow. At a mean follow-up of 5.1 months, both hypogastric limbs are patent and no endoleaks were observed. In conclusion, until commercially-produced branched hypogastric endografts are widely available, techniques such as those described above can allow for hypogastric preservation during aortoiliac aneurysm repair without the need for device modification or brachial access for hypogastric limb delivery.
Introduction
Concomitant iliac aneurysms are seen in as many as 30% of patients undergoing endovascular aneurysm repair. 1,2 Although there are open surgical options for hypogastric preservation during endovascular aneurysm repair, patients with aortoiliac aneurysms treated by fully endovascular means typically undergo embolization of the hypogastric artery with extension of the iliac endograft limbs into the external iliac arteries, as prefabricated branched hypogastric grafts are not yet commercially available. 3,4 While many patients will tolerate hypogastric occlusion without major sequelae, between 12 and 50% of patients will suffer thigh and buttock claudication postoperatively, and sexual dysfunction has been observed in 20–50%. 4–6 Several reports have described either off-label or surgeon-modified use of devices to achieve aneurysm repair with hypogastric preservation, as commercially available devices with prefabricated hypogastric side branches are not yet available. 7–10 This report details the use of a bifurcation-sparing endograft which allows placement of additional covered stent-grafts into the hypogastric artery to preserve hypogastric perfusion without device modification or the need for brachial access.
Case report
Patient 1
An 82-year-old man presented to the emergency room with abdominal pain and a 6.7-cm abdominal aortic aneurysm (AAA) with bilateral common iliac artery aneurysms (with chronic dissections) measuring greater than 3 cm. His past medical history included oxygen-dependent chronic obstructive pulmonary disease and coronary artery disease, as well as a history of a left colectomy. Because of his co-morbid medical conditions, he was felt to be a poor candidate for open surgical repair. Because of his prior colectomy, we were concerned that bilateral hypogastric occlusion could place him at risk of bowel ischemia and, therefore, decided to proceed with coil embolization of one hypogastric artery followed by preservation of the other through endovascular aneurysm repair with a hypogastric branch technique.
Patient 2
A 66-year-old man with a history of hypertension and hypercholesterolemia was evaluated for a rapidly enlarging 5.3-cm AAA with bilateral common iliac artery aneurysms measuring 3.8 cm on the right and 3.3 cm on the left. The patient wished to undergo endovascular repair, and because of his concern regarding the risk of claudication and sexual dysfunction with occlusion of the bilateral hypogastric arteries, we decided to proceed with unilateral coil embolization followed by hypogastric branch technique aneurysm repair.
Operative technique
For each of these procedures, bilateral femoral access was obtained by duplex-guided puncture of the common femoral arteries, and following angiographic confirmation of appropriate puncture placement through a micropuncture sheath, the sheaths are upsized to 6F sheaths bilaterally. The ‘preclose’ technique is used to place sutures in each femoral artery (in a manner previously described by Lee et al. 11 ) prior to dilation of the arteriotomies. Next, the appropriately sized Endologix Powerlink (Endologix Inc, Irvine, CA, USA) unibody bifurcated device is introduced (ipsilateral to the common iliac aneurysm and the hypogastric artery requiring preservation) and deployed according to the manufacturer's instructions for use, followed by the aortic proximal extension cuff. Following this, the existing marker pigtail catheter within the endograft is advanced to the suprarenal aorta and used to introduce a 0.035-inch stiff-angled Glidewire (Terumo Medical, Somerset, NJ, USA) on the contralateral side. The Endologix delivery sheath is then removed in exchange for an 18F Cook sheath (Cook Medical, Bloomington, IN, USA) and then another Glidewire is advanced through this sheath in a buddy-wire fashion adjacent to the existing Lunderquist wire (Cook Medical) up to the ipsilateral endograft limb. The pigtail catheter is then advanced over the wire up to this level and then reformed. The reformed catheter is then advanced through the limb and main body of the device to avoid passing behind the stent interstices of the endograft (which lie on the inside of the fabric of the graft). Once it reaches the suprarenal aorta, it is exchanged over a guide-wire for a tri-lobed snare and its catheter (ev3, Plymouth, MN, USA). This is then used to snare the contralateral stiff-angled Glidewire which is then brought out through the ipsilateral sheath in order to create a rail which enters the contralateral sheath, spans the aortic bifurcation and exits the ipsilateral sheath (Figure 1a). This ‘rail-wire’ then allows exchange of the existing sheath (Figure 1b) in the contralateral groin for an appropriately sized sheath (measuring 55 cm in length) to deliver the hypogastric stent graft (typically ranging in sizes between 8 and 12F). Use of a sheath 2F larger than the size required for the delivery of the hypogastric stent graft will allow one to keep the ‘rail-wire’ in place for additional stability during hypogastric cannulation and stent delivery, though this is not required. Once the up-and-over sheath has been advanced from the contralateral groin to the origin of the ipsilateral hypogastric artery, catheterization of the ipsilateral hypogastric artery is performed with an angled Glide Catheter (Cook Medical) and stiff-shaft Glidewire (Terumo Medical). Once confirmatory angiography has been performed and distal hypogastric artery landing zone has been identified and sized, the angled Glide Catheter is exchanged for a 0.035-inch Rosen wire (Cook Medical). Next, an appropriately sized Viabahn covered stent (W L Gore and Associates, Flagstaff, AZ, USA) is advanced into position, spanning the distance from the origin of the iliac limb of the bifurcated device down to the distal landing zone of the hypogastric artery. Before delivery, an Endologix iliac extension limb (16 mm diameter) is advanced up to the origin of the iliac limb of the bifurcated device alongside the Viabahn (Figure 2a). The up-and-over femoral sheath is then backed up until its tip rests at the aortic bifurcation, and then these two grafts are deployed simultaneously (Figure 2b). Finally, postimplantation balloon angioplasty is performed simultaneously using a non-compliant angioplasty balloon in the Viabahn graft and a semi-compliant Coda balloon (Cook Medical) in the Endologix limb. The stronger radial force of the Viabahn stent graft relative to the Endologix iliac extension limb allows the iliac limb to deform around the Viabahn stent graft, thus reducing the chance of type III endoleak (inset, Figure 3). This allows for convenient sizing of these components, as the Viabahn can be chosen to match the diameter of the hypogastric artery and the 16-mm Endologix limb can be used with any diameter Viabahn. Additional molding of the iliac limb around the Viabahn is performed with the combination of the non-compliant angioplasty balloon in the Viabahn and the semi-compliant balloon in the iliac limb.
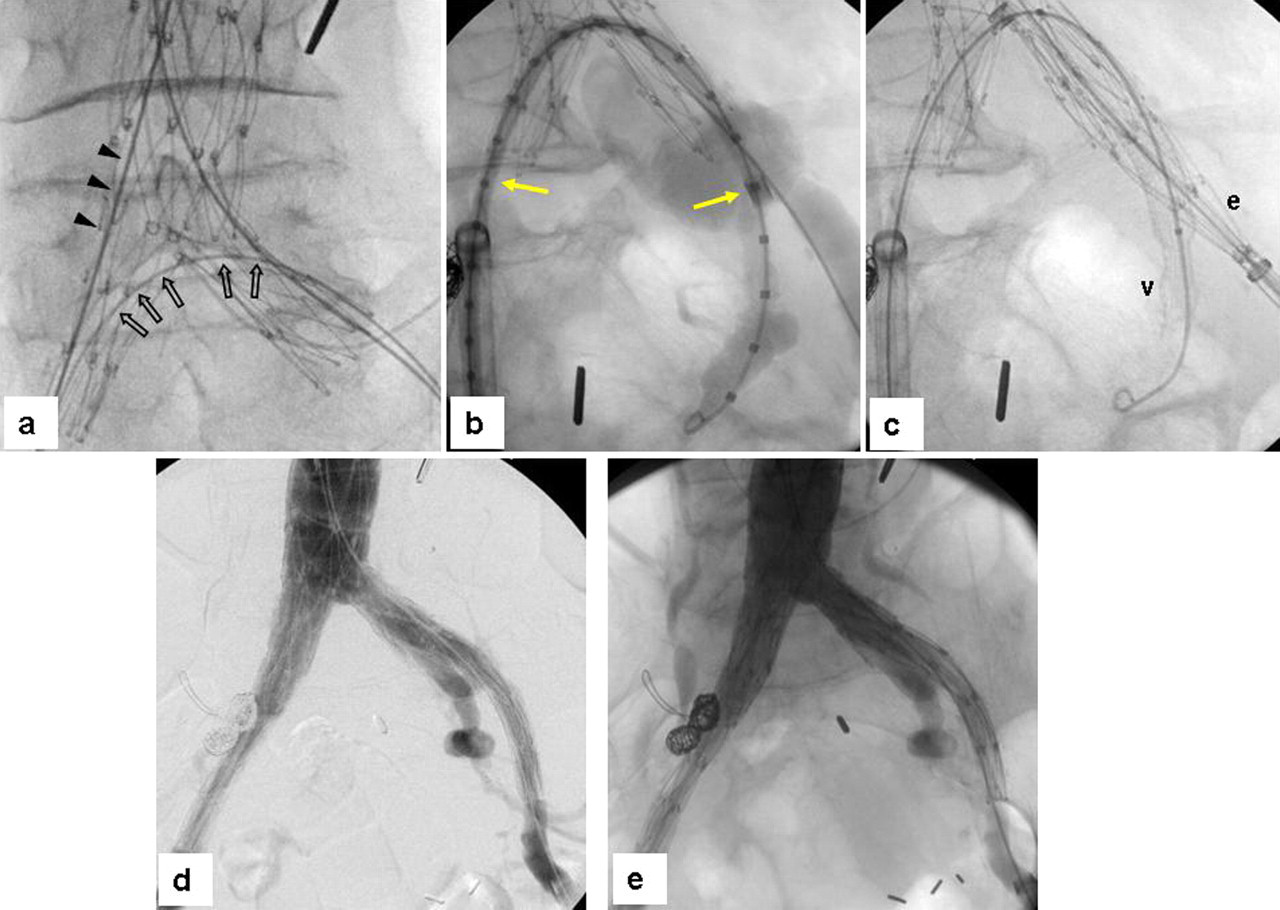
Intraoperative angiograms for patient 1. (a) The unibody bifurcated graft has been implanted, and the stiff shaft angled Glidewire (open arrows) has been inserted alongside the ipsilateral Lunderquist wire (arrowheads) and brought out the contralateral sheath as a ‘rail-wire’ to facilitate passage of the up-and-over sheath. (b) Angiogram through the up-and-over sheath (yellow arrow) with a Rosen wire/marker pigtail catheter allows for hypogastric limb sizing. (c) Simultaneous deployment of the Viabahn covered stent (‘v’) into the hypogastric and Endologix limb (‘e’) into the external iliac. The origins of both these stents rest at the origin of the left iliac limb of the bifurcated endograft. Completion angiography demonstrates preserved perfusion of the hypogastric artery (d, e)
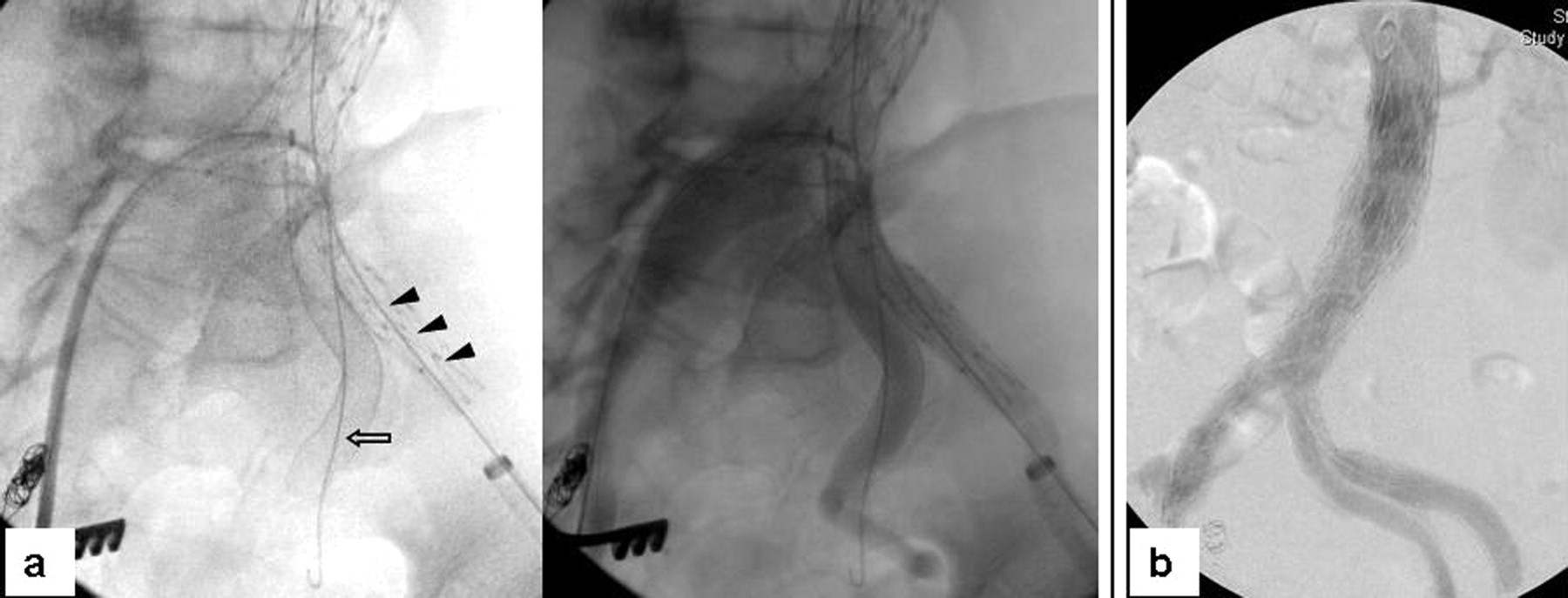
Intraoperative angiograms for patient 2. (a) The Lunderquist wire (arrowheads) is used to guide the Endologix external iliac limb while a Rosen wire (open arrows) guides the Viabahn covered stent in the hypogastric artery. (b) Double-barrel configuration of the hypogastric and external iliac limbs within the iliac limb of the bifurcated endograft excludes the common iliac aneurysm and preserves hypogastric blood flow
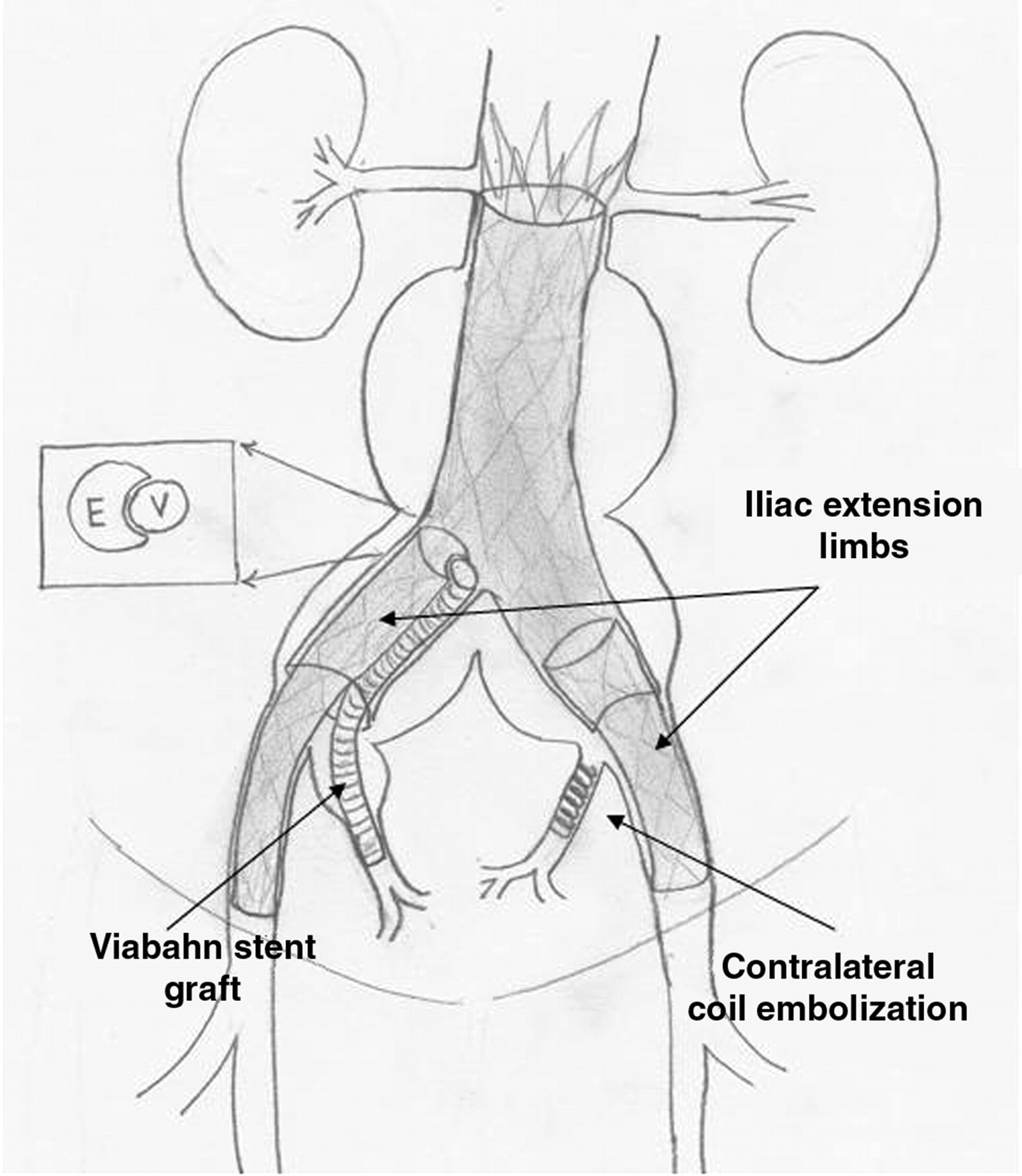
Diagram demonstrating ‘double-barrel’ configuration of the hypogastric stent graft and iliac extension limb. The stronger radial force of the Viabahn graft relative to the Endologix iliac extension limb allows the iliac limb to conform around the hypogastric stent graft (inset)
At this point, completion angiography is performed to rule out the presence of major endoleak, though mild type III endoleaks between the double-barrel components are left untreated as these tend to resolve spontaneously. Sheaths and wires are then removed, and the arteriotomies are closed with the previously placed Perclose (Abbott Vascular, Abbott Park, IL, USA) sutures.
Each of these patients did well following their respective procedures and were discharged home within the first two postoperative days without complications. At a mean follow-up of 5.1 months, both are free from endoleaks and have patent iliac and hypogastric graft limbs (Figure 4). Patient 2 developed mild unilateral buttock claudication ipsilateral to the hypogastric artery which had been treated with coil embolization, though this was improved at last follow-up.

Postoperative computed tomography angiogram with three-dimensional reconstructions demonstrating successful aneurysm repair with preservation of hypogastric perfusion in both patients. No endoleaks are present and all external iliac and hypogastric limbs are patent
Discussion
Typical management of common iliac aneurysmal disease includes coil embolization of the ipsilateral hypogastric artery with extension of the iliac graft limb into the external iliac artery. 3,4 While pelvic circulation collaterals often provide sufficient perfusion to the affected side to avoid major sequelae, between 12 and 50% of patients who undergo sacrifice of one or both hypogastric arteries will suffer thigh and buttock claudication postoperatively. 4,5 Of those who develop claudication, symptom improvement or resolution will occur in roughly half, but the remaining will continue to have some degree of disability due to this problem. 4 Additionally, sacrifice of hypogastric blood flow can also result in impotence in 20–50% of patients, as well as more serious complications such as bowel ischemia. 4,6 While the rate of clinically significant bowel ischemia is less well characterized and likely quite rare, this complication has been reported in the literature and can have a catastrophic impact on outcome. 12,13
Options for preserving hypogastric perfusion in those patients without sufficient distal landing zone for placement of an endograft within the ipsilateral common iliac artery have typically required some type of open surgical intervention. Such options include standard open aneurysm repair with direct anastomosis to the common iliac bifurcation, hybrid approach involving hypogastric artery bypass or transposition in conjunction with placement of a standard endograft, or other types of hybrid extra-anatomic reconstructions. 14–18
Repair of these aneurysms with aortic endografts containing prefabricated hypogastric branches is another method for preserving hypogastric perfusion. While these devices are under development and currently in use through clinical trials in the USA and elsewhere, they are not yet commercially available, and access to such technology is limited for patients and their treating physicians. 19–23 Because of these limitations, several groups have recently developed techniques for hypogastric preservation utilizing commercially available devices. 7–10 Oderich and Ricotta 7 have described back-table modification of an iliac stent graft limb with a presewn polyester side graft delivered into the ipsilateral hypogastric artery. While technically feasible, back-table modification of commercially available devices carries concerns of long-term device durability as well as regulatory issues. Friedman et al. 8 described the repair of bilateral common iliac artery aneurysms using multiple main body bifurcated endograft devices deployed in the iliac vessels. While this technique allows for successful aneurysm repair, there is a significant financial cost associated with using multiple main body bifurcated endograft components. To circumvent these issues, Lobato et al. 9 described aortoiliac aneurysm repair using brachial access to deliver a covered stent into the hypogastric artery alongside an endograft limb delivered via the ipsilateral femoral artery, thus creating a double-barreled system originating in the iliac limb of a standard bifurcated graft with termination of the double-barrel system into the ipsilateral external iliac and hypogastric arteries. While our group has used this technique for treating aortoiliac aneurysms, we have noted that considerable tortuousity can be introduced throughout the course of the subclavian artery, thoracic and pararenal aorta, and aortic bifurcation, thus increasing the technical difficulty and leading to inability to deliver the hypogastric stent graft in at least one patient. Additionally, the need for brachial access leads to increased morbidity, especially considering the large sheath sizes sometimes required to introduce stent grafts of appropriate size for the main trunks of the hypogastric artery. To address these issues, we utilized the Endologix Powerlink device for repair of the aneurysms in these two patients, as this endograft preserves the aortic bifurcation in contradistinction to all other commercially available endografts. This allows for placement of an up-and-over sheath from the contralateral groin which is used for delivery of the hypogastric stent graft without the need for brachial access. By use of a through-and-through femoral guide-wire acting as a guide-rail, we have delivered sheaths as large as 14 Fr over the aortic bifurcation within the endograft. The design of this particular device leads to sparing of the normal anatomy of the aortic bifurcation, thus facilitating hypogastric preservation procedures such as these.
While these two case reports describe unilateral hypogastric preservation using this technique, the procedure can be performed for bilateral hypogastric preservation by using the ‘rail-wire’ to move the up-and-over sheath to the opposite femoral artery. The branching-procedure can then be repeated to preserve the second hypogastric artery in the same fashion as the first.
Type III endoleak between the iliac limb and hypogastric stent graft component is a potential source of failure of this technique. Though our experience with this and similar procedures suggests that these endoleaks will tend to resolve by the time of subsequent axial imaging, we have chosen to use the 16-mm Endologix limb as the iliac limb component in part due to the concern regarding persistent type III endoleak. If such a leak is to persist, a balloon-expandable stent can be deployed in the proximal iliac limb, thus expanding into the Endologix iliac limb to its full intended diameter and simultaneously collapsing the hypogastric artery stent graft. Functionally, this results in hypogastric exclusion and extension of the endograft into the external iliac artery.
The primary limitation of this technical report is the limited follow-up period available on these two patients. While the long-term durability of this technique is not yet known, full aneurysm exclusion with preservation of hypogastric perfusion and absence of endoleak was achieved in each of these patients.
Conclusions
Hypogastric preservation during endovascular repair of aortoiliac aneurysms is feasible utilizing non-modified, commercially available devices. Use of a bifurcation-sparing endograft facilitates such operations by allowing delivery of the hypogastric stent graft limb via contralateral femoral access. This fact not only decreases the technical complexity of these procedures and alleviates the morbidity associated with brachial access, but also has implications for future branched endograft development.
Footnotes
Acknowledgments
Financial disclosure of authors and reviewers: none reported.