
Abstract
Although acute elbow dislocations are common orthopedic injuries, concomitant neurovascular injury is rare. Brachial artery transection can result from open elbow dislocation and responds well to vascular repair. Rapid evaluation and a high level of suspicion are essential to facilitate immediate treatment. Delay to identify vascular injury after elbow dislocation or reduction can potentially lead to limb ischemia, and potential loss of limb. We present a case of relatively rare transection of the brachial artery, with an accompanying traumatic open elbow dislocation in a 12-year-old boy.
Introduction
The elbow is the second most commonly dislocated joint in the adult population and the most commonly dislocated major joint in the pediatric population. 1 Despite this, neurovascular injury associated with acute traumatic elbow dislocation is rare. 2 Arterial injury is a recognized complication of closed and open traumatic elbow dislocation. 3
In this case report, we present a case of relatively rare transection of the brachial artery, with an accompanying traumatic open elbow dislocation in a 12-year-old boy.
Case presentation
A 12-year-old boy (height, 4 ft 11.8 in; weight, 103.6 pounds) was admitted to another hospital's emergency department with open elbow dislocation as a result of a heavy object falling on his left elbow. Anamnestically, he complained of severe elbow pain and a laceration on his left arm. He had a laceration over the antecubital fossa and this was an open injury. Roentgenograms performed at the local rural hospital revealed a posterior elbow dislocation without associated fractures. He was evaluated by a consultant orthopedic surgeon. Under analgosedation, the elbow was reduced with a closed reposition by the orthopedic surgeon. Subsequently, primary closure of the laceration was carried out. His arm was maintained in 90° of flexion with a posterior plaster splint. There were no signs of acute limb ischemia in the patient and he was discharged. Additional information cannot be obtained about the vascular examination at the initial evaluation in the patient report.
Three days after the initial injury, the patient was referred to our hospital with complaints of coldness in the left hand. On physical examination, his left hand was cooler than the opposite side, but well colored. There was an approximately 5-cm sutured laceration over the antecubital fossa. In bilateral comparison, left radial and ulnar pulses were absent. However, capillary refill was presented but delayed, indicating incomplete ischemia by collateral perfusion. No neurological deficit was noticed. A control roentgenogram of the elbow made in our institution showed no dislocation. Subsequently, a duplex sonography was performed and revealed an unclear discontinuance of the brachial artery with complete occlusion of the left brachial artery. An angiogram was performed through a right femoral approach using a 4 French sheath and diagnostic catheter. An arteriogram revealed complete occlusion of the left brachial artery with some preserved collateral circulation (Figure 1).
Angiogram shows a disruption of the brachial artery with good collateral circulation filling the distal vessels
With the diagnosis of brachial artery injury, the patient was taken to the operating room. A longitudinal incision was made over the ante-cubital fossa under general anesthesia. An incision was extended along the medial aspect of the arm. A complete transection of the brachial artery, approximately 5 cm in length, was detected with lacerated distal and proximal vessel ends and homeostasis by internal stagnation thrombus (Figure 2a). The brachial artery diameter was ∼3.2 mm. The median nerve was found to be intact. After resecting all bruised segments of the brachial artery, the brachial artery was repaired with a reversed, end-to-end, autogenous greater saphenous vein graft (Figure 2b). The greater saphenous vein diameter in the proximal thigh was ∼3.5 mm. The ruptured brachial vein was ligated. No kink was observed with a 90° flexion. Skin closure was performed without any tension.
(a) Operative photograph shows the complete transection of the brachial artery at the level of the elbow. The arrow indicates the transected brachial artery. (b) Operative photograph shows that the brachial artery was repaired with a reversed, end-to-end, autogenous greater saphenous vein graft. The arrow indicates the arterial bypass with the saphenous vein graft
Following the repair, adequate pulsations were noted in the distal brachial artery and at the wrist. His arm was maintained in 90° of flexion with a posterior plaster splint for a period of two weeks. Postoperative follow-up was without complications. He was discharged home on the fourth postoperative day in good condition. For three months, standard antiaggregation therapy was applied. Six months later, the arm functioned normally. The graft was patent and the patient was asymptomatic.
Discussion
Acute elbow dislocations are relatively common injuries. Elbow dislocations run the risk of concomitant injury due to the anatomic proximity of neurovascular structures. Concomitant vascular injuries are rare but serious.
4
The arterial injuries are estimated to occur in approximately 5–13% of elbow dislocations, most frequently in cases of open or penetrating injuries.
5
The majority of elbow dislocations are closed and posterior, but a small percentage is either anterior dislocations or open injuries (Figure 3a and 3b).
6
Risk factors for vascular involvement include open injuries, concurrent trauma and the absence of a radial pulse.
7
Open elbow dislocations are often associated with vascular injuries. Vascular injury usually results from direct, either penetrating or blunt, trauma. Indirect injuries (artery avulsion) are much rarer. Indirect avulsion-type injuries are usually connected with dislocations of large joints.
8
The brachial artery is most commonly injured, but occasionally the radial and ulnar arteries are the involved vessels. The different lesions of the brachial artery have been described in the literature. Injuries to the brachial artery include spasm, stretching, contusion, laceration, intimal flap, rupture, entrapment and thrombosis.
9
The presence of pulses at the wrist does not exclude an arterial injury; however, the absence or weakness of pulses at the wrist should suggest concomitant vascular injury until proved otherwise. The diagnosis of arterial spasm should not be accepted as the cause of an ischemic appearing limb without further diagnostic procedures. Rapid evaluation and a high level of suspicion are essential to facilitate prompt treatment, as a delay in diagnosis is associated with a poorer outcome.
7
If there is a suspicion of arterial injury, appropriate diagnostic studies must be performed.
Sample X-ray demonstrating a posterior (a) and an anterior (b) dislocation of the elbow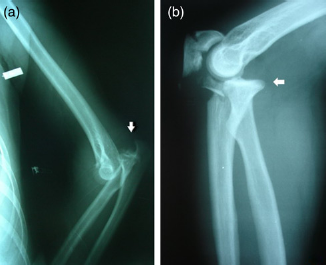
The rich collateral circulation around the elbow involves seven vessels as shown in Figure 4. As in our case, severe acute ischemia is not inevitable in the case of brachial artery transection, and the initial diagnosis of arterial damage may not be clinically evident. The rich collateral circulation around the elbow can mask findings of acute arterial occlusion, with the accompanying risk of a delayed diagnosis. The collateral circulation explains why delayed operative management is not always linked with bad prognosis.
10
Drawing shows the rich arterial collateral circulation around the left elbow
Both emergency room physicians and orthopedic surgeons play a vital role with regard to the initial evaluation and treatment of these patients. One of the most important roles of the emergency room physician and orthopedic surgeon with individuals presenting with elbow dislocations is the evaluation for concomitant vascular injuries. Failure to identify vascular injuries with a thorough vascular examination both before and after elbow dislocation reduction can potentially lead to severe morbidity with limb ischemia, cold intolerance, compartment syndrome and potential loss of limb. 5 If there are any signs of a vascular injury, a vascular surgeon consultation should be obtained immediately.
Duplex ultrasonography (USG) is used to evaluate suspected injury to the brachial artery. 11 However, its benefits are mostly dependent on the experience of the radiologist. 8 Duplex USG should not be routinely done in all patients with elbow dislocation including anterior and open. If there is any suspicion of a vascular injury, it should be done. Angiography is considered as the gold standard diagnostic procedure, because duplex sonography is not easily performed on an injured limb. 10 Initially, we used non-invasive duplex ultrasound to evaluate our patient. The brachial artery injury was suspected with duplex ultrasound. Thereon, angiography was performed to make a definitive diagnosis.
Satisfactory treatment of this injury includes immediate reduction of the dislocation, vascular repair and bridging fixation of the elbow. 12 In the first stage, bone stabilization is indicated. Subsequently, vascular repair is performed. 8 Although conservative treatment with simple ligation of the brachial artery has been described, results are less consistent. Despite the rich collateral circulation, most authors have recommended arterial repair with either direct suture or interposition with a reversed vein graft. Arterial repair is believed to lessen the risk of delayed complications, including claudication of the forearm and hand, cold intolerance and potential growth disturbances. 9 Primary repair of the vessel is always preferable if the gap is not too large or if the ends are not too traumatized. A gap that is too large to be approximated with a native vessel should be bridged with autogenous tissue. 11 Primary repair is usually impossible because of lack of length after debridement. Arterial ligation is reserved for those who require immediate attention to other injuries or severe hypovolemic shock. 3 Venous repair is not performed, as there are usually sufficient collateral vessels to allow adequate venous drainage in the upper extremity. 7 We preferred to bypass with a reversed saphenous vein graft because of the large damaged segment of the brachial artery. To prevent postoperative compartment syndrome, fasciotomy is indicated in cases of elevated pressure in the forearm compartment, severe soft tissue injury or extended delay between injury and repair. 4 Prophylactic fasciotomy was not performed, because compartment syndrome signs were not detected in our case.
In conclusion, elbow dislocations are common and their association with a brachial artery injury is very rare. The rich periarticular collateral circulation can mask findings of acute arterial occlusion, which can delay the diagnosis. The absence or weakness of pulses at the wrist with the open elbow dislocation can be a very important alarm sign of artery injuries. Emergency physicians and orthopedic surgeons play a vital role with regard to the initial evaluation of these patients. Early diagnosis and immediate operative repair synchronized with the vascular surgeon happen to be the only acceptable treatment of this complicated injury.
Footnotes
Acknowledgments
Financial disclosure of authors and reviewers: none reported.