
Abstract
The purpose of this study was to describe the use of a bifurcated endovascular graft to treat endograft migration with major endoleaks. We present four patients who presented at a mean of 72.0 months after their initial endovascular abdominal aortic aneurysm repair. Three patients had type I endoleaks resulting from proximal attachment failure and graft migration. A fourth patient had separation of a proximal aortic cuff from a migrated main body device resulting in a type III endoleak. All were treated with a bifurcated Zenith (Cook Medical Incorporated, Bloomington, IN, USA) endovascular graft. There was 100% technical success with no perioperative complications. On follow-up, one patient died of unrelated causes at five months. The mean survival for the remaining three patients was 37 months. In conclusion, treatment with a bifurcated Zenith endograft has advantages over the use of an aortic cuff or aortouniiliac reconstruction. To perform this technique, there must be a sufficient distance between the proximal landing zone and the flow divider of the migrated endograft to allow for deployment of the Zenith device. While there remain limitations in its applicability, the use of a bifurcated endovascular graft is a viable alternative for endovascular salvage in treatment of endograft migration with major endoleaks.
Introduction
Since the introduction of endovascular abdominal aortic aneurysm (AAA) repair (EVAR) in 1991, this technique has become widely accepted as a safe and effective treatment modality for infrarenal AAAs. 1 While numerous studies have demonstrated the perioperative benefits of EVAR, the long-term survival benefits of EVAR remain uncertain. 2,3 Furthermore, EVAR has been associated with an increased rate of graft-related complications and need for secondary interventions. 4,5
Potential complications of EVAR include the development of endograft migration which can lead to type I or type III endoleaks. 6 As major endoleaks can lead to aneurysm expansion, surgical intervention is warranted to prevent aneurysm rupture. In this report, we present the first report of the use of bifurcated Zenith (Cook Medical Incorporated, Bloomington, IN, USA) endovascular grafts to treat endograft migration with major endoleak.
Case reports
Patient information including mode of failure and implanted device
*At time of secondary intervention
†After initial endovascular abdominal aortic aneurysm repair
All EVARs were performed in the operating room under general anaesthesia with endotracheal intubation. Open-surgical exposure of the bilateral femoral vessels was utilized and imaging was performed with portable C-arm fluoroscopy. No adjunctive procedures were required to lower the flow divider of the migrated endograft. All patients had placement of a bifurcated Zenith endovascular graft main body and additional iliac limbs with the landing zone distal to the prior endograft in the native artery. In one patient, the aortic neck was short and endovascular repair was attempted with a surgeon-modified endograft with a fenestration created for preservation of a previously stented renal artery. However, this ultimately proved unsuccessful and there was intentional coverage of the left renal artery orifice. In all cases, completion angiography was performed following deployment to confirm exclusion of the aneurysm sac. Technical success was 100% and there were no perioperative complications (Figures 1–3). The patient who required coverage of the left renal artery had elevated serum creatinine levels to 1.9 mg/dL (baseline 1.0). All patients were subsequently discharged home after a mean length of hospital stay of 3.8 (range 2–8) days. Follow-up after discharge included office visits and telephone interviews, as well as CT imaging.
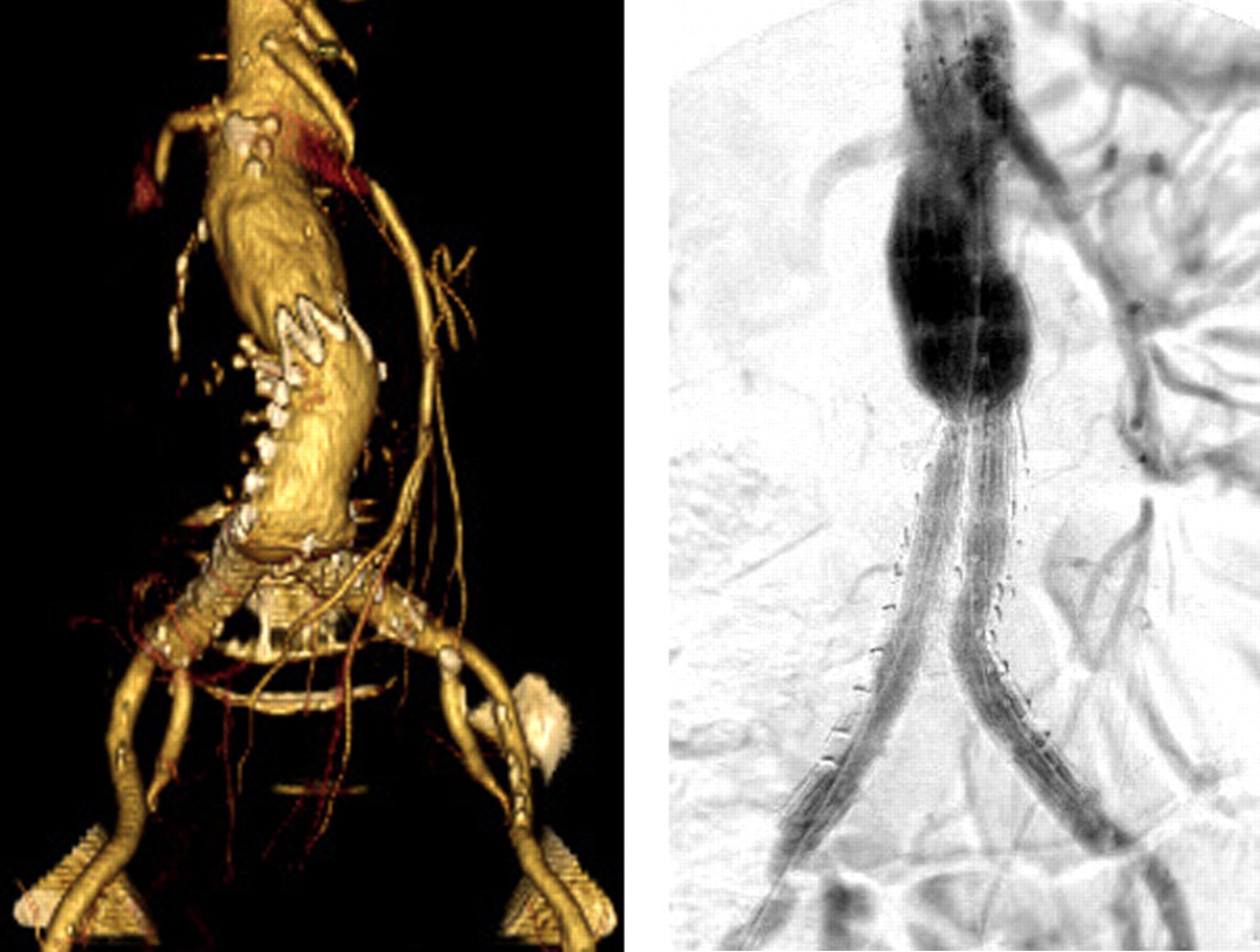
Intraoperative angiogram (left) and postoperative computed tomography angiogram (right) of a patient treated for migration of a Talent endograft three years after initial implantation Preoperative computed tomography angiogram (left) and completion angiogram (right) of a symptomatic patient (abdominal pain) treated for migration of an Ancure endograft 10 years after initial implantation Preoperative computed tomography angiogram (left), intraoperative angiogram (middle) and completion angiogram (right) of a patient who presented with separation of an AneuRx aortic cuff and migrated main body device over seven years after initial implantation

During follow-up, one patient died at five months after the secondary intervention. There was no evidence that the death was aneurysm-related. The remaining patients are alive at a mean of 40 (range 23–62) months after their secondary intervention. Two patients have type II endoleaks not associated with aneurysm expansion. The third patient developed evidence of a proximal type I endoleak 24 months after the secondary intervention. However, further treatment was deferred due to the patient's advanced age (97 years old). The patient remains alive 35 months after the secondary procedure.
Discussion
Potential failures of endovascular repair include the development of major endoleaks. Proximal type I endoleaks can develop from endograft migration and type III endoleaks result from separation of modular components. As these major endoleaks can lead to aneurysm expansion with the potential for rupture, intervention is warranted when they are identified. Major endoleaks can happen several years after initial endograft implantation. As such, the patients will be several years older and may have additional medical co-morbidities not present during the initial operation. Intervention in these patients, therefore, may be more challenging as they are often not candidates for open-surgical conversion.
Migration has been shown to be a potential complication of all available endografts. However, the AneuRx device (Medtronic, Santa Rosa, CA, USA) has been reported to have higher migration rates than other devices. In an earlier series, migration rates of 27 to 42% at three years were reported. 7,8 This was partially attributed to its use in patients with suboptimal anatomy. In general, the rates of migration are low with other available devices. The decline in this complication may be attributable to improved design features such as suprarenal fixation, proximal barbs and hooks or the use of anatomic fixation. 6
Endovascular treatment of migrated endografts has been reported in the literature with varying degrees of success. In a series of 20 patients, 14 out of 16 (88%) patients with proximal attachment failure from an AneuRx device were successfully treated with an aortic cuff at one year follow-up. 9 A later report showed that only 17 of 23 (74%) patients had successful secondary reconstruction with proximal cuffs at 14 months of follow-up. 10 In another series of patients (with a mean follow-up of 16.4 months) requiring secondary intervention for a variety of failure modes, proximal cuffs were successful in only five of 11 (45%) patients while the use of a Talent AUI device (Medtronic) allowed successful repair in 13 of 15 (86%) cases. 11 This study also reported the successful use of a bifurcated Talent endograft (Medtronic) in six of seven patients with failed tube graft repairs. More recently, the results of the Zenith Renu AAA Ancillary Graft (Cook Medical) post-market registry demonstrated a clinical success rate of 78.8% in a group of 151 patients with a mean follow-up of 45 months. 12
There have been several reports describing complete relining of failed endografts. In most cases, relining with endovascular components (aortic cuffs and/or iliac limbs) was performed to treat sac expansion from endotension seen with the original permeable Excluder (W L Gore and Associates, Flagstaff, AZ, USA) device. 13,14 The use of a bifurcated device in the treatment of major endoleaks from a prior bifurcated EVAR was first reported in 2003. 15 A patient underwent placement of a bifurcated Excluder to treat a type III endoleak due to fabric tear in an implanted Ancure device (Guidant, Menlo Park, CA, USA). In a more recent study, six patients (five bifurcated, one tube) with failed Vanguard prosthesis (Boston Scientific, Natick, MA, USA) were successfully treated using an Excluder device. 16 Three patients with migration were successfully treated without the need for additional technical measures. However, the remaining three patients suffered from endograft disintegration and the failed Vanguard endograft remained in place. In these patients, there was insufficient length to allow the opening of the contralateral gate of the Excluder device within the trunk of the failed prosthesis. The authors presented their technique of placement of a transfemoral crossover guidewire in order to pull the prior endograft caudally in order to gain sufficient length. In a mean follow-up of 26 months, two patients died of unrelated causes and there was no need for additional secondary interventions.
It is important to point out that the use of a bifurcated device cannot be applied to all cases of migration as there are specific anatomic requirements to this technique. To perform endovascular salvage, there must be sufficient length between the proximal landing zone and the flow divider of the migrated endograft to allow deployment of the contralateral gate of the bifurcated device. The length required varies with the available bifurcate devices and depends on the distance between the proximal edge and the contralateral gate: 70 mm for an Excluder; 74 mm for the Zenith and the Endurant (Medtronic); and 80 mm for a Talent endograft. If the required length is not present, endovascular salvage with a bifurcated device may still be possible if the migrated endograft can be pulled caudally (as described by Rancic et al. 16 ) to create the necessary distance.
In cases where the anatomy is appropriate, the use of a bifurcated device may provide the most durable repair for major endoleaks from device migration. In a bifurcated repair, arterial flow is completely eliminated from the prior endograft and there is no further reliance on the prior endograft for aneurysm exclusion. This differs significantly from the use of aortic cuffs as the continued structural integrity of the prior endograft is still required for durable success. In addition, the seal between an aortic cuff and a prior endovascular device depends on the overlap between the devices. It has been shown that any device with a short body will have a higher risk for component separation, development of type III endoleaks and aneurysm rupture. 17 As such, we feel that the use of aortic cuffs does not provide a durable repair in the treatment of migrated endografts. While arterial flow can be excluded from the prior endograft in cases of an AUI repair, this procedure mandates additional intervention in the form of a femorofemoral bypass with contralateral iliac occlusion. Furthermore, the documented success of traditional EVAR with bifurcated devices is far superior to the results of aortic cuff repairs and AUI reconstructions as discussed above.
In this series, we were able to successfully treat four patients who presented with endograft migration and major endoleaks with placement of a bifurcated Zenith device. In all cases, there was sufficient length for placement of a Zenith main body device. In one case, a single renal artery was intentionally covered after a failed attempt with a surgeon-modified fenestrated device. The distal landing zones for the iliac limbs during the secondary intervention were chosen in each case to be beyond the previous repair. All cases were able to be completed with a technical success rate of 100%. While there was one death at five months and development of a type I endoleak in another patient after two years, the overall survival of this small cohort likely is superior to what may be seen if the major endoleaks were not treated or if the patients underwent open-surgical intervention. However, further follow-up is necessary to determine the durability of this type of repair.
Conclusions
Endograft migration with major endoleaks is a possible complication of EVAR. Endovascular salvage is possible with the use of aortic cuffs and AUI reconstructions. However, these are associated with significant failure rates. While the need for adequate length for placement of a bifurcated device may limit its application, treatment with a bifurcated endograft is a viable alternative for endovascular salvage in the treatment of endograft migration with or without major endoleaks.
Footnotes
Acknowledgments
The authors disclose that Dr Sanchez is a consultant for the following: Cook, Medtronic, Endologix, Gore, Aptus Endosystems and Trivascular II.