
Abstract
The aim of this paper is to report an unusual case of a patient with an abdominal aortic aneurysm (AAA) and a hydronephrotic horseshoe kidney (HSK) that was repaired by endovascular means. An 81-year-old male patient with a known HSK was found to have hydronephrosis and an AAA. The patient's aneurysm was treated with an endovascular stent graft which required the covering of accessory renal arteries. He had an uneventful recovery with complete resolution of the hydronephrosis evident on a computed tomography scan performed seven months after the surgery. In conclusion, endovascular aneurysm repair is a feasible therapeutic option for an AAA coexisting with an HSK and may be considered as a valid alternative to open repair when concomitant hydronephrosis is present.
Introduction
Coexistence of an abdominal aortic aneurysm (AAA) and a horseshoe kidney (HSK) is an uncommon finding and treatment of these patients is challenging. Open surgery has traditionally been considered the standard of care for repair of the AAA. This is often technically demanding due to the presence of accessory renal arteries, along with the presence of the overlying isthmus.
Endovascular aneurysm repair (EVAR) has been described in sporadic reports as an alternative method for treatment when morphologically feasible and when renal function is normal. We report a case of an AAA with a coexistent hydronephrotic HSK. Our patient was treated with an endovascular stent graft followed by aneurysm sac size reduction and complete resolution of the hydronephrosis.
Case report
An 81-year-old male patient was known to have an HSK since early childhood. A computed tomography (CT) scan obtained for biliary disease revealed an AAA of 5.8 cm in diameter and the HSK with hydronephrosis of the left kidney. His renal function was normal with a glomerular filtration rate (GFR) of 91.3 mL/minute. A CT angiogram (CTA) demonstrated the AAA, a large and dominant right kidney and a partially enhancing left kidney with significant hydronephrosis (Figure 1a). In addition, accessory renal arteries were seen supplying the right kidney and the renal isthmus (Figure 1b). An aortogram demonstrated a large 6-mm main right renal artery and a smaller 4-mm left renal artery. In addition, two accessory renal arteries were seen: a 2-mm right accessory artery originating from the top of the aneurysm and a 3-mm accessory artery originating from the aortic bifurcation supplying the lower pole of the right kidney and isthmus (Figure 1c).
(a) Preoperative computed tomography angiogram (CTA) demonstrating abdominal aortic aneurysm-horseshoe kidney and left hydronephrosis (arrow). (b) Preoperative CTA demonstrating accessory right renal arteries (short arrow) and perfused renal isthmus (long arrow). (c) Preoperative aortogram demonstrating a 3-mm accessory renal artery originating from the aortic bifurcation supplying the lower pole of the right kidney and isthmus. (d) Postoperative CTA at one month demonstrates the stent graft in place (short arrow) and the segment of the isthmus and the right kidney lower pole that had undergone infarction as a result of coverage of the accessory renal artery (long arrow). (e) Postoperative CTA at seven months demonstrates resolution of the left hydronephrosis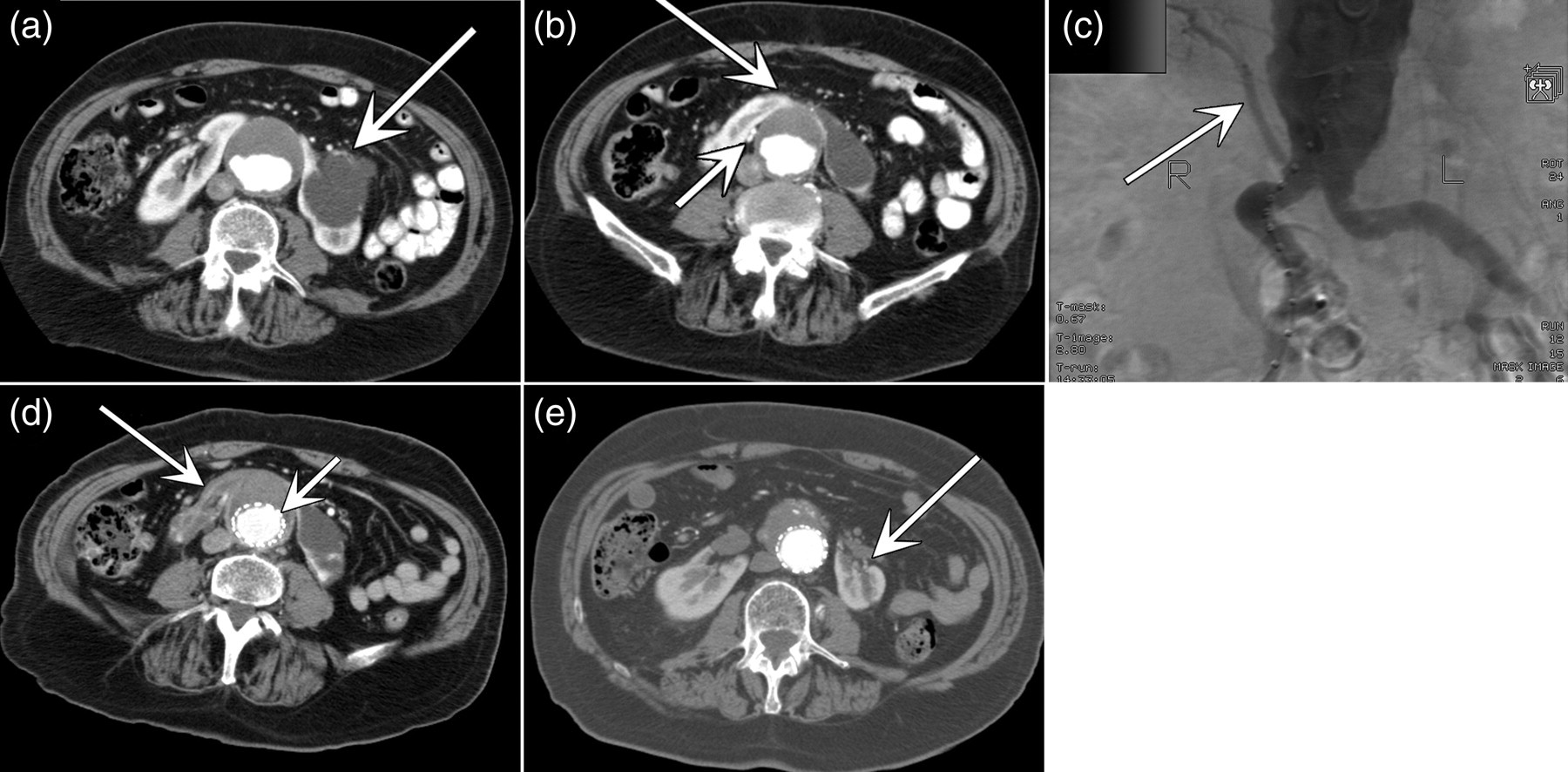
A renal scan revealed a contribution of 92% of the total renal function from the right kidney and only 8% from the left. EVAR was opted for repair. Consideration was given to preoperative drainage of the hydronephrotic left kidney. This was not performed since the left kidney contributed relatively little to the overall renal function.
The patient underwent an endovascular repair for his AAA using a bifurcated Zenith stent graft (Cook, Bloomington, IL, USA). This procedure required covering the accessory renal arteries with the stent graft and therefore sacrificing the vasculature to the lower pole of the right kidney and the isthmus. Based on the preoperative imaging, we anticipated that this would not have a significant deleterious effect on the overall renal function. The patient had an uneventful operative and postoperative recovery and his renal function remained stable in the postoperative period with a GFR of 71 mL/minute.
A CTA performed one month postoperatively showed that a small segment of the isthmus and the right kidney lower pole had undergone infarction as a result of coverage of the accessory renal artery (Figure 1d). No endoleak was present. On a repeated CT scan performed seven months after the surgery, the aneurysm sac had shrunk in size to 4.9 cm diameter. The left hydronephrosis had completely resolved (Figure 1e). On a follow-up CT done three years postoperatively, no endoleaks were present. The aneurysm sac diameter was 4.7 cm, and the left kidney was well perfused with no evidence of hydronephrosis. It was smaller compared with the right kidney but had grossly unchanged in size from three years prior. The patient's overall kidney function remained normal with a GFR of 71 mL/minute.
Discussion
HSK is the most common congenital abnormality of the kidney, with a reported incidence of one per 400–800 live births, and a male predominance of 2:1. 1 It results from a fusion anomaly of the embryonic renal tissue in which both kidneys fuse together at their inferior pole at a region traditionally called the isthmus. The isthmus typically lies anterior to the aorta and the inferior vena cava, and is primarily composed of functioning renal parenchymal tissue, but occasionally can be composed of fibrous tissue. It is typically asymptomatic and is frequently found as an incidental finding on imaging studies. Several complications accompanying this anomaly can occur, among them, ureteropelvic junction obstruction. This results in significant hydronephrosis in as many as one-third of individuals. 1 The high insertion of the ureter into the renal pelvis, its abnormal course anterior to the isthmus and the anomalous blood supply to the kidney may individually or collectively contribute to this obstruction.
HSK is known for its high variability in blood supply. Various classifications of aberrant vascularization associated with HSK exist, including Papin, Eisendrath, Crawford's and Boatman's. Crawford's classification is based on the origin of the renal arteries, in which he describes three types of vascularizations: Crawford I, two renal arteries with normal origin; Crawford II, two normal and 1–3 anomalous renal arteries originating from the infrarenal aorta or iliac arteries; and Crawford III, all renal arteries have an anomalous origin.
AAA in combination with an HSK is uncommon and presents in 0.12% of patients undergoing AAA repair. 2 The initial investigative modality of choice to assess an HSK-AAA entity and thus plan for surgical repair is a CTA. 3 This provides information regarding the wall, lumen and caliber of the aortic aneurysm, as well as the anatomy of the renal malformation, its parenchyma, and the morphology of its collecting system. The angiographic portion aids in assessment of the aortic lumen, origin of the principal renal arteries and the caliber of the accessory renal vessels.
Although open repair of AAA-HSK malformations is considered the treatment of choice for AAA-HSK, EVAR has been described as an alternative modality for treatment, when technically feasible and when renal function is normal. 3 EVAR is considered to reduce operative time, trauma and pain, avoids technical difficulties and promotes rapid recovery.
Review of available literature reveals possible complications of EVAR for AAAs combined with HSKs, including segmental renal infarcts, worsening of renal function, transient hypertension and type II endoleaks, which involve retrograde flow from collateral branches such as the lumbar, testicular, inferior mesenteric and hypogastric arteries. 4,5
In the case of EVAR, where accessory renal arteries need to be covered by the stent graft with no option for reimplantation, there is general consensus regarding which of these can be sacrificed without sequela. Accessory arteries of ≤3 mm may be covered, usually without significant sequel, as long as the main renal vascular anatomy can be preserved and the patient has otherwise normal renal function. 3,5
Preservation of accessory renal arteries originating from the distal aorta or iliac arteries is usually not possible. Since accessory renal arteries can be considered terminal arteries, with few exceptions, type II endoleaks are not commonly expected. 5
Regarding the hydronephrosis, if unilateral and asymptomatic, with no compromise of renal function, there is usually no need for immediate intervention. In our case, it is reasonable to assume that the AAA was the cause for the obstruction by compressing the isthmus, further complicating the abnormal course of the left outflow tract. Aneurysm sac size regression most probably relieved the compression of the left outflow tract, resulting in resolution of the hydronephrosis. Regression of hydronephrosis is a well described phenomenon following EVAR for the treatment of inflammatory AAAs, and can be appreciated in 38% of the patients treated for that entity. 6
Conclusion
EVAR of AAAs in the presence of an HSK is a feasible alternative for open repair. It is essential that a complete assessment of the HSK and its vasculature be done prior to proceeding with surgery. In case of associated hydronephrosis, regression of the hydronephrosis may be anticipated following repair providing there has been regression in the size of the aneurysm sac.