
Abstract
We present a case of atypical acute limb ischemia in a non-diabetic patient, with ankle–brachial pressure index of 0.6 and rest pain localized exclusively over the gastrocnemius muscle, sparing the foot. This uncommon presentation was attributed to an impaired perigenicular collateral network. Thrombolysis restored adequate perfusion only temporarily and was followed by thromboembolectomy. The ischemia presentation in our case underscores the importance of the adequacy of the perigeniculate collateral network for the perfusion of the tibial muscles and, especially, the gastrocnemius muscle.
Introduction
A key point in the diagnosis of critical limb ischemia is the presence of ischemic rest pain, typically localized in the distal part of the foot, most commonly occurring with an ankle pressure below 50 mmHg. 1 We present a case of atypical presentation of acute limb ischemia with diagnostic pitfalls and subsequent management.
Case history
A non-diabetic 83-year-old man with a history of chronic atrial fibrillation presented to the Emergency Department with severe calf pain on the right, having started suddenly 14 days ago. The palpation of the calf was barely tolerated. On the contrary, there was neither pain nor sensory/motor deficits in the foot. No palpable pulses below the popliteal level were detected and the ankle–brachial pressure index was 0.6 (anterior tibial artery, ATA: 60 mmHg, no audible signal over the posterior tibial artery, PTA). Thus, the suspicion of critical ischemia was remoted and the patient was further managed in the Department of Internal Medicine. The duplex ultrasound performed excluded deep venous thrombosis. However, the pain did not subside and the need for further consultation was brought up again.
The findings of the diagnostic angiography were consistent with popliteal embolism (Figure 1a). Only the ATA and the medial superior genicular artery were visualized (Figures 1a and b). Electively positioned catheter thrombolysis followed (Figure 1c) and the popliteal artery was visualized again, along with the supra- and infragenicular collaterals (Figure 1d). Although the tibioperonial trunk remained occluded, the mid- and lower segments of the PTA were visualized again (Figure 1e), through an ‘unofficial’ collateral network (Figure 1f).
The right supragenicular popliteal artery with the medial superior genicular artery (a). Only the anterior tibial artery is visualized as run-off vessel (b). Intra-thrombotic placement of a catheter for thrombolysis (c). After one hour of thrombolysis (Alteplase, Actilyse®, Boehringer Ingelheim, Ingelheim, Germany), the popliteal artery restored patency. The superior medial (white arrow), inferior medial (black arrowhead) and superior lateral (white arrowhead) genicular artery are visualized after the thrombolysis, as well as the medial sural artery (black arrow) (d). The middle part of the posterior tibial artery (e) is visualized through a collateral network of perforators (white arrowhead), derived from the perforating branches. The peroneal artery appears occluded (white arrow) (f)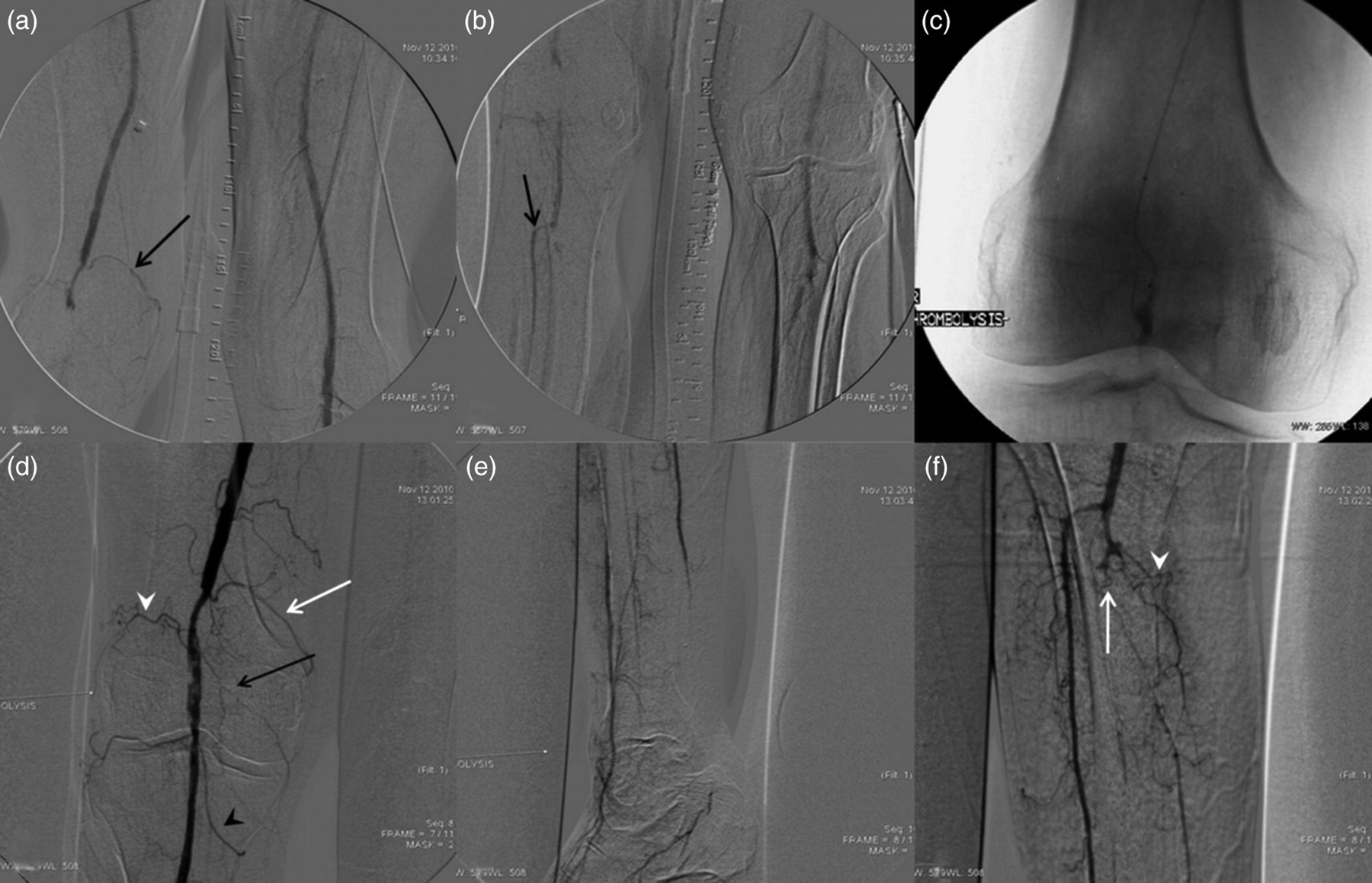
The patient marked instant remission of pain, rendering the palpation tender no more. Unfortunately, the thrombolysis was abandoned early because the patient was stressful and agitated and soon thereafter the popliteal artery was occluded again. This time the origin of the ATA was not spared, the Doppler signal over the dorsalis pedis disappeared and the foot presented with a mottling appearance with excessive motor and sensory impairment, rendering the need for operative management urgent. A thromboembolectomy was performed successfully and blood flow was immediately restored through the ATA and PTA (100 and 50 mmHg, respectively). The sensory and motor function was unimpaired and the gastrocnemius muscle was non-tender in palpation. Fasciotomy was not performed in order to avoid additional morbidity based on a clinical impression that the compartmental pressure was normal. The patient was released three days later on anticoagulation therapy in good health and remains fully ambulant up to now for six months.
Discussion
Typically, the ischemic rest pain is localized in the distal part of the foot or in the vicinity of a gangrenous toe or ischemic ulcer. 1 In our case, the localization was rather atypical, since the only complaint was a tenderness and mild swelling, strictly localized over the gastrocnemius. Along with the pressure measurement over the ATA, no criterion fulfilled the typical diagnosis of critical ischemia according to the guideline criteria of the Inter-Society Consensus for the Management of Peripheral Arterial Disease. 1 The setting of the ischemia in our case underscores the importance of the adequacy of the perigeniculate collateral network for the perfusion of the tibial muscles and, especially, the gastrocnemius muscle.
Since the exact anatomic description of the vascular interconnection in the muscular departments of the tibia is considered unclear by the majority of the clinicians, the thorough description provided by the angiosome model as first introduced by Taylor in the plastic reconstructive surgical field may delineate the unique characteristics present in our case.
2,3
The blood supply of the posterior calf comes from the superficial sural artery and the musculocutaneous perforators from the medial and lateral sural arteries.
3
The gastrocnemius is divided into three territories. Its supply arises in the popliteal fossa, not above it, having a relatively poor connection with other vessels of the leg.
3
Its proximal part is supplied by the sural (medial and lateral) arteries. Before entering the muscle, these also send small branches to supply both heads of the muscle. Distally, the medial and lateral aspects of the muscle receive perforating branches from the PTA and the peroneal artery, respectively, passing through the soleus and entering the deep surface of the gastrocnemius.
3
Throughout the thrombolysis, the PTA was not visualized retrograde via the ATA and through the plantar arch (Figure 1e), so we assume that the perforators of the perigeniculate network provided adequate gastrocnemius perfusion, being sufficient to dramatically relieve the painful symptoms of the muscle. The efficiency of the perigeniculate collateral network (Figure 2) (sural, superior and inferior genicular arteries) has been repeatedly proven to suffice for the viability of the foot, even in the absence of infrapopliteal run-off vessel, provided that the proximal inflow is unimpaired.
4–7
Schematic drawing of the perigenicular branches. SFA, superficial femoral artery; DGA, descending genicular artery; Art branch of DGA, articular branch of DGA; SMG, superior medial genicular artery; SLG, superior lateral genicular artery; ILG, inferior lateral genicular artery; Pop A, popliteal artery; sural a, sural arteries (medial and lateral); IMG, inferior medial genicular artery; Ant Tib Rec a, anterior tibial recurrent artery; ATA, anterior tibial artery; PTA, posterior tibial artery; Musc Perf a, muscular perforators; Per A, peroneal artery
Since the localized discomfort over the gastrocnemius was puzzling, we performed angiography, which showed almost total absence of a sufficient perigenicular network and PTA, leading us to perform thrombolysis. Recent reports favor the use of thrombolysis as an effective way of treating acute limb ischemia caused not only by thrombotic occlusion but also by an acute embolic event. 8,9 Despite the conventional perception of considering an old embolus as a clot too organized to respond sufficiently to thrombolytic therapy, this hesitation seems over-estimated. 10
Had the patient been more compliant, the result of the thrombolysis could have been more satisfactory and permanent. 11,12 Unfortunately, thrombosis of the ATA followed the early treatment failure, causing severe ischemia to the foot, which led us to the operation room, where an embolus and fresh thrombus were removed with subsequent restoration of perfusion. Overall, localized interruption of the collateral network supplying specific muscular territories may provide an explanation of pathogenesis in variable clinical syndromes, where blood perfusion through typical vessels is compromised. Interventional efforts to preserve the integrity of the perigenicular collaterals are justified, even in the absence of intact run-off tibial vasculature.
Conclusion
This case reaffirms that the foot is not the sole ‘end-organ’ in the leg; this is not an uncommon scenario even though it may not have been highlighted in the existing literature. The junctional zones between the angiosomes, represented by anastomotic sites within the muscles of the lower limb, can be helpful for explanation of pathogenesis in variable clinical syndromes, where blood perfusion through typical vessels is compromised or interrupted. Interventional efforts to preserve the integrity of the perigenicular collateral network should be justified, even in the absence of intact run-off tibial vasculature.