
Abstract
The management of aortoiliac insufficiency has been improved considerably since the introduction of balloon-expandable stents in 1991. Although numerous studies have shown the safety and efficacy of balloon-expandable iliac artery stent placement, the procedure is not without potential complication. We report here a very unusual case of iliac artery stenting being complicated by deformation and elongation of the stent following balloon rupture at initial deployment with retention of the distal balloon marker and our successful approach to subsequent management with combined acetylsalicylic acid and clopidogrel. In conclusion, this conservative approach may be an alternative treatment of a partially deployed aortoiliac stent with a retained foreign body when further intervention is considered to be of high risk.
Introduction
Endovascular solutions to aortoiliac insufficiency are the primary treatment modality, initially by simple angioplasty with supplemental stent insertion in lesions with residual stenosis. Recently, however, aortoiliac stents have become accepted as the primary therapy in cases that are not suitable for treatment with angioplasty alone. 1,2 Although numerous studies have shown the safety and efficacy of balloon-expandable iliac artery stent placement, 3–5 the procedure is not without potential complication.
We report here a very unusual case of iliac artery stenting being complicated by deformation and elongation of the stent following balloon rupture at initial deployment with retention of the distal balloon marker and our conservative approach to subsequent management. The otherwise uncomplicated intervention left a retained foreign body attached to a partially unravelled stent sitting within the distal aorta with the perceived potential for subsequent thrombus formation.
Case report
A 63-year-old man presented to his general practitioner with sudden onset of weakness in both legs and deterioration in his walking distance to 200 yards. The patient was a smoker with a past history of deep venous thrombosis, recurrent bilateral leg ulcers and venous skin changes. On clinical examination, femoral, popliteal and pedal pulses were absent bilaterally. In the absence of femoral pulses, a computed tomography (CT) angiogram was undertaken and showed very heavy calcification throughout the aortoiliac segments with right common iliac artery (CIA) and left external iliac artery (EIA) occlusions: 49 and 12 mm, respectively, in length (Figure 1).
Computed tomography angiogram of the abdominal aorta with occlusion of the right common iliac and the left external iliac arteries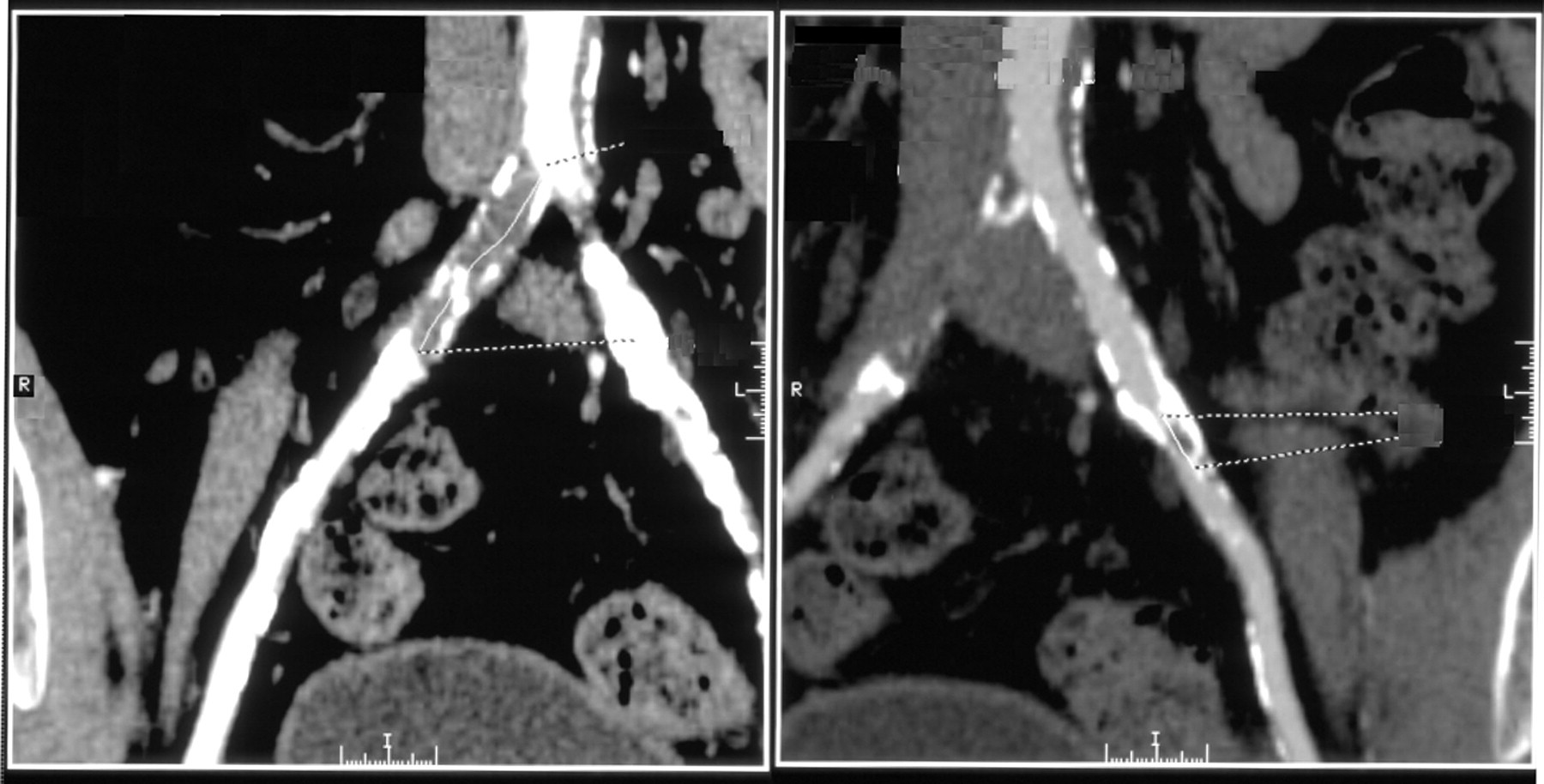
Discussion at the vascular multidisciplinary team meeting concluded that – in view of symptom deterioration – the patient should be offered angioplasty and stenting. The patient subsequently gave his informed consent. An intraprocedural angiogram through a standard bilateral femoral approach confirmed an occlusion at the origin of the right CIA and a short occlusion in the left EIA, with a normal left CIA. The left occlusion was stented with an 8‐mm Medtronic BridgeTM balloon-expandable stent (Medtronic, Minneapolis, MN, USA) without difficulty, with a satisfactory angiographic result. The right-sided stenting, with a similar 8‐mm stent, was complicated by balloon rupture during the inflation phase of the deployment process at a pressure of 8 atm. There was no resistance as the stent was advanced and the patient experienced no discomfort at the time of balloon rupture. Following placement, the catheter was advanced slightly in accordance with the manufacturer's instructions and without symptoms prior to withdrawal. Apart from the disrupted balloon and missing distal balloon marker, the catheter did not appear to be broken or damaged. Completion angiography following deployment demonstrated an apparently patent and stented right CIA.
Following the procedure, the patient was informed of the complication and a further CT angiogram confirmed patent aortoiliac segments with good placement of the left-sided stent. The cranial portion of the right-sided stent was partially unravelled and extended into the distal aorta, forming a central filling defect; additionally, the catheter balloon marker was noted to be attached to its upper aspect (Figure 2).
A poststenting computed tomography angiogram demonstrating successful stenting of both the right common and left external iliac arteries, with the partially unravelled cranial portion of the right iliac stent sitting in the distal abdominal aorta and the balloon marker still attached to its upper aspect (arrow)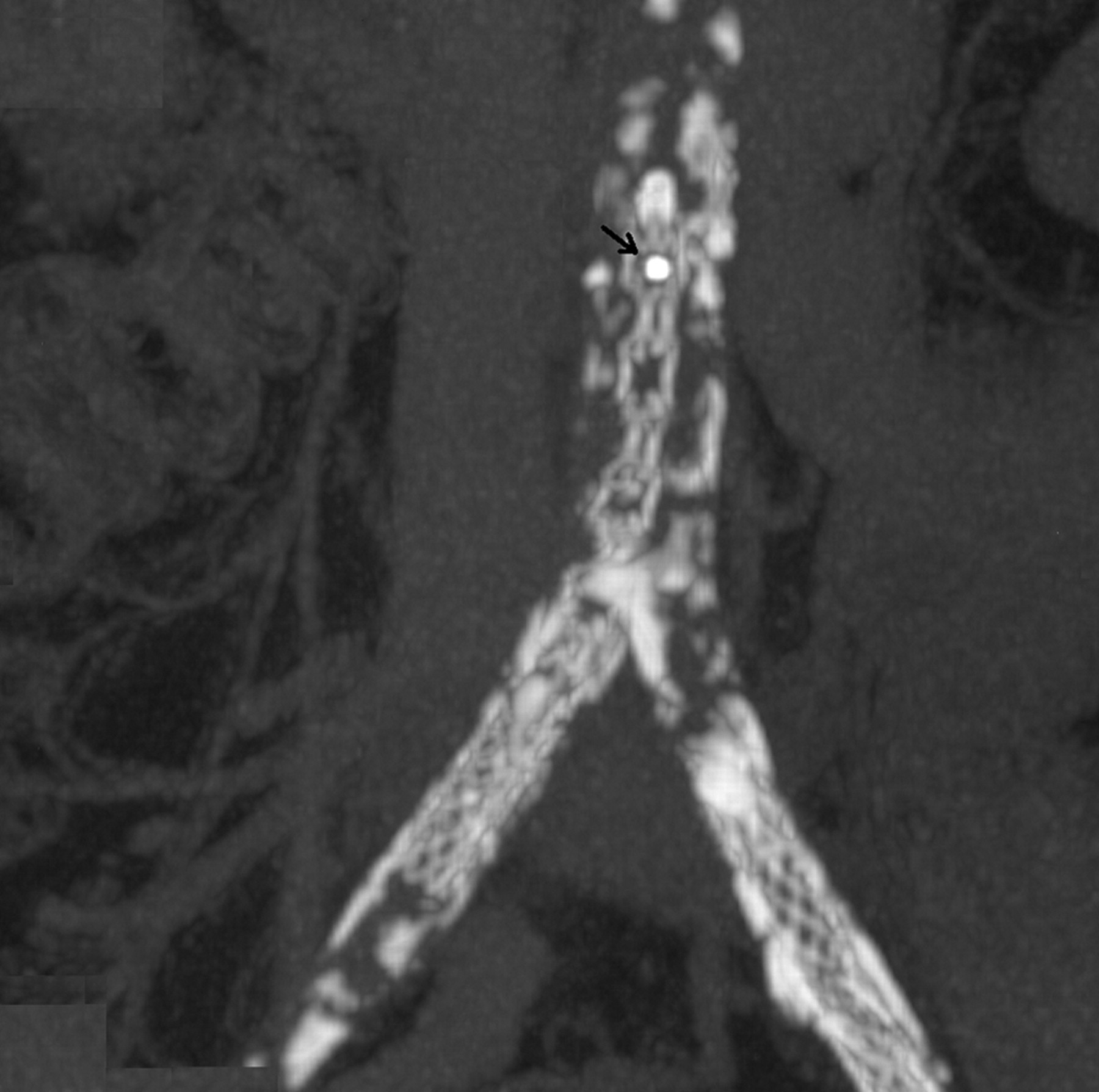
Clinically, the patient had an excellent result from the procedure with loss of symptoms and the return of normal resting pressures with no significant reduction after exercise. The manufacturers were asked to comment on the deformation and elongation of the stent.
On clinical discussion poststent placement, a repeat angioplasty to correct the stent deformity was considered, but it was concluded that conservative treatment in the form of a combination dual-antiplatelet therapy was the most sensible approach, as the patient's symptoms had resolved and that further intervention was felt only to add further risk to the patient. Acetylsalicylic acid and clopidogrel were hence commenced.
A follow-up CT angiogram at three months postdeployment showed no evidence of thrombus formation or any change in the CT appearance from the time of deployment. The patient continues to be well without symptoms and with normal ankle-brachial pressure indices until now, some five years postprocedure.
Discussion
Stent deformation is a recognized, but rare, complication of stent placement on long-term follow-up. 6,7 This case report demonstrates that it can occur during the initial deployment procedure and can subsequently be managed conservatively.
It would appear that deployment complicated by balloon rupture caused a portion of the disrupted balloon to become entangled with the stent, causing elongation when the catheter was further advanced prior to its removal. The postprocedure CT angiogram showing the radio-opaque balloon marker at the top of the partially unravelled stent supports this view.
The manufacturers commented that they had had no such similar reports and confirmed that there was no apparent fault in the returned catheter.
Although the occlusion in the right CIA has been resolved and the patient's quality of life has improved dramatically, there were initial concerns that the partially unravelled stent may result in turbulent flow and act as a nidus for thrombus formation. 3,8 Furthermore, there were concerns regarding the thrombogenic potential of the retained balloon marker and the attached portion of the disrupted balloon itself. Our concerns have until now not been realized. It may be that the high flow rate within the aorta is an important positive factor here.
Tan et al. 9 demonstrated that antiplatelet therapy in the form of acetylsalicylic acid plus clopidogrel is effective and safe in preventing restenosis following peripheral artery angioplasty and stenting when compared with anticoagulation therapy; however, no evidence in the literature describing a conservative approach to the complication above has been found. With the follow-up now at over five years, this conservative management appears to have been the correct approach to this unusual incident and suggests that a retained foreign body consisting of the balloon marker with an attached portion of the disrupted balloon and a partially unravelled stent are not necessarily thrombogenic and can be managed medically.
This case demonstrates that deformation and elongation of stents can occur at initial deployment together with balloon marker retention, but this occurrence does not necessarily result in a bad clinical outcome, where a conservative approach to management with combined acetylsalicylic acid and clopidogrel proved to be appropriate. Although unusual, such complications do develop, but are frequently under-reported. Interventional radiologists and vascular surgeons are therefore encouraged to report similar occurrences.
Footnotes
Declarations