
Abstract
Carotid artery stenting is considered to be an alternative to carotid endarterectomy for selected patients by many vascular specialists around the world. Acute stent thrombosis following the procedure, although very infrequent, can risk the survival of the patient. In this report, we present a case of acute stent thrombosis 24 hours following the procedure. After a slow deterioration of the clinical state of the patient, he was urgently subjected to thrombectomy with extraction of the stent, with eventual resolution of his symptoms. A review of the current literature is presented together with all the possible treatment options of this serious complication. In conclusion, several neurorescue procedures are available for the vascular surgeon who has to act urgently and, in some cases, aggressively, when stent thrombosis is diagnosed.
Introduction
Carotid artery stenting (CAS) is an integral alternative treatment for carotid artery disease. Its efficacy and safety have been consolidated especially following the results of the most recent, wide-range, randomized controlled trial. 1 The indications of the technique are more clearly delineated nowadays unlike the first years of its use. As for every method, complications related to the procedure may arise, the most common being cerebral embolization. Acute carotid thrombosis following CAS is a very rare complication which may be lethal for the patient without immediate treatment.
In this report, we present a case of successful surgical treatment of an acute stent thrombosis following CAS and a review of the existing literature on the management of this infrequent condition.
Case report
A 67-year-old male painter was admitted to our department after an episode of transient ischemic attack (TIA), in the form of right facial nerve paresis one month prior to his admittance. The patient underwent a series of imaging studies consisting of triplex ultrasound (U/S) of both carotid bifurcations, heart duplex examination, cerebral computed tomography (CT) scanning and CT angiography (CTA) of the aortic arch and supra-aortic vessels, in order to diagnose possible atherosclerotic lesions of the above vasculature, or cardiac arrhythmias. On CTA and triplex scanning of the carotid arteries, a preocclusive stenosis was revealed in the left carotid bifurcation and a 50% stenosis in the contralateral carotid artery. Cerebral CT did not reveal any infarct on the left cerebral hemisphere. One week before his admission to the hospital, the patient was started on low-molecular-weight heparin by his neurologist.
The patient was a heavy smoker consuming around 1.5 package/day for 37 years. In 2006, he was operated for thyroid cancer followed by regional neck radiation therapy due to lymph node metastasis, from which he had fully recovered. Three days before his admittance, the patient interrupted his anticoagulation therapy and initiated clopidogrel medication once daily. An endovascular carotid revascularization procedure was decided due to previous neck dissection and radiation.
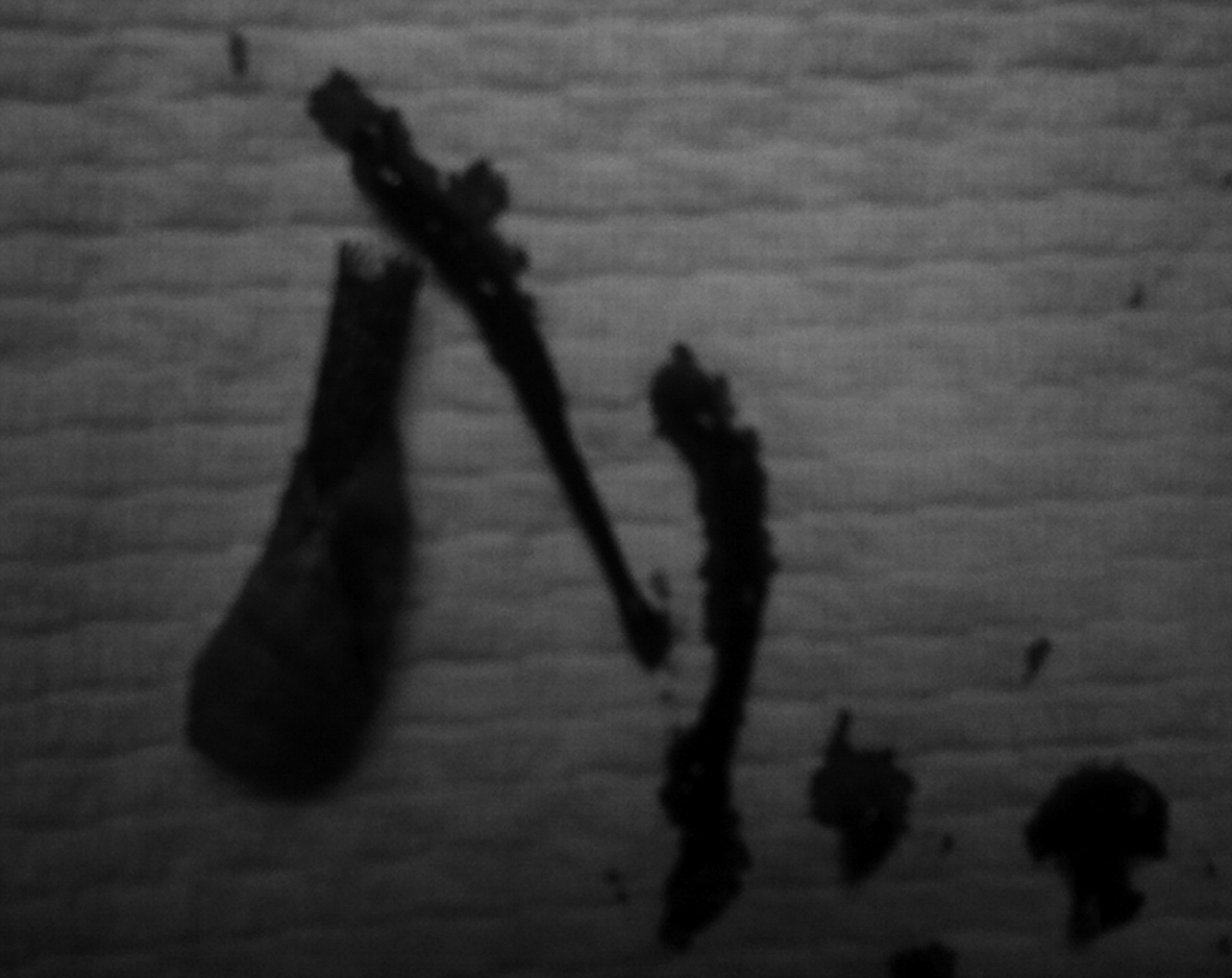
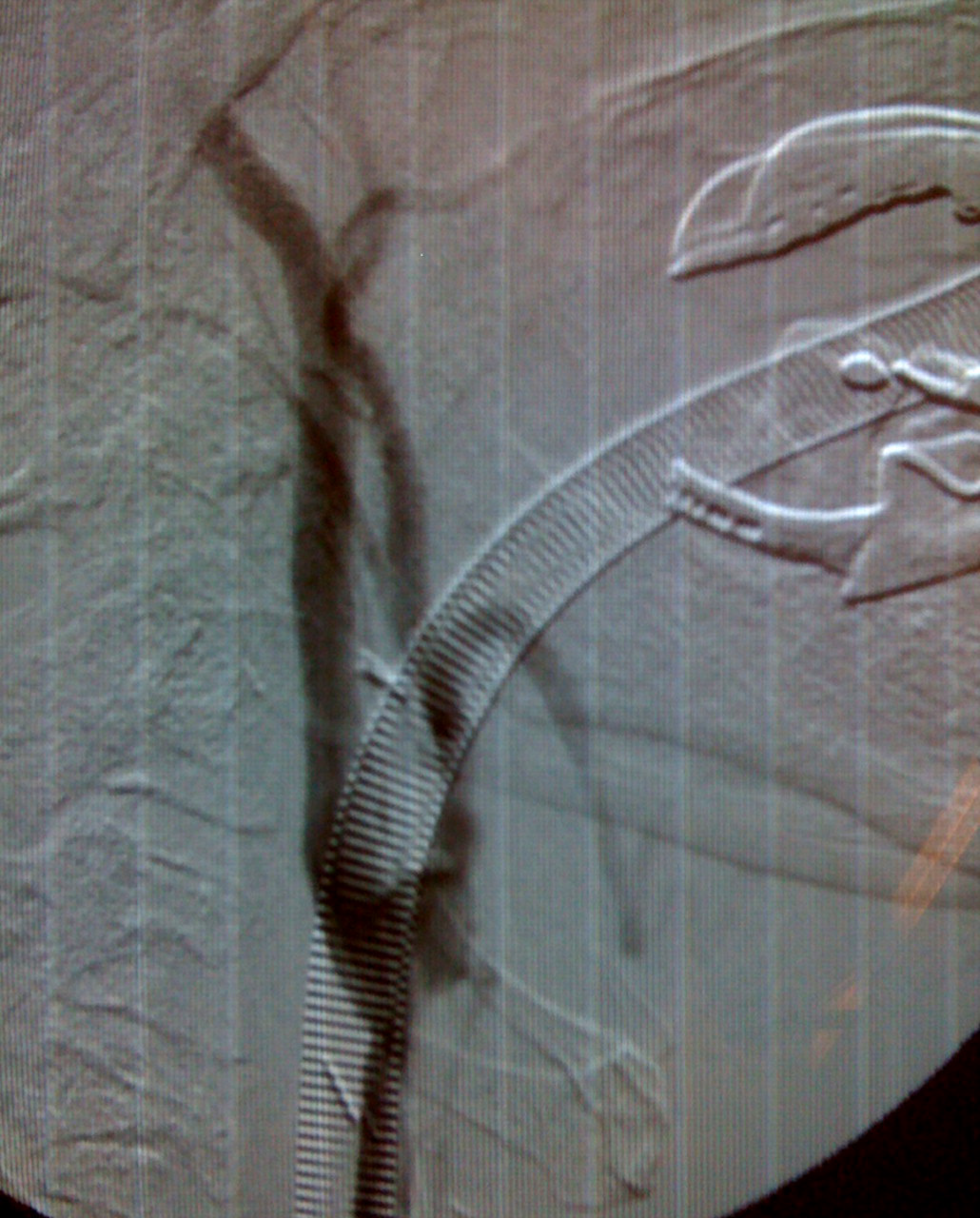
Routine right transfemoral CAS was performed, with the use of a cerebral protection filter (ANGIOGARD XP filter basket diameter 6 mm; Cordis, Johnson & Johnson, Waterloo, Belgium) and the deployment of a tapered, self-expandable, nitinol stent RX Acculink Stent System (6–8 mm; Abbott Vascular, Cedex, France) without predilation. Final angiography confirmed the correct position of the stent and the end result with complete dilation of the internal carotid artery stenosis (Figure 1). After recovery from general anesthesia, the patient returned to the ward without any neurological deficit. On the second postoperative day, the patient developed numbness with a mild weakness in his right arm. An urgent triplex U/S of the left carotid bifurcation revealed no flow in the left internal carotid artery and the portion inside the stent, a sign indicative of acute stent thrombosis. An emergent cerebral CT scan did not reveal any signs of intracerebral hemorrhage. The patient accidentally did not receive the dual antiplatelet medication which is routinely prescribed following CAS procedures. A bolus infusion of 5000 IU of heparin was instantly induced together with systemic heparinization (25,000 IU/24 hours) while the patient was set under close monitor surveillance of his vital signs and his neurological state. His clinical situation was stable following heparin infusion with no signs of neurological deterioration. On the third postoperative day, the patient complained of a further worsening of the muscle strength of his right hand and, in addition, of a difficulty of speech. Due to the worsening of the neurological situation despite the increased levels of heparin therapy, a surgical neck exploration was decided upon. The patient was urgently transferred to the operating room, where a standard neck dissection for carotid endarterectomy (CEA) was performed. After injection of 5000 IU of heparin and clamping of the common carotid and external carotid arteries, a longitudinal arteriotomy of the common carotid and the internal carotid artery was performed. The carotid stent was recognized, with fresh thrombus occluding its lumen, which was meticulously removed. After stent removal, no back bleeding from the internal carotid artery was observed. A number 2 Fogarty catheter was then cautiously introduced in the internal carotid artery for approximately 10 cm. After slow and delicate removal of the Fogarty catheter, a long portion of fresh red thrombus was extracted from the internal carotid artery followed by active back bleeding (Figure 2). The internal carotid artery was clamped followed by typical endarterectomy and primary closure of the arteriotomy (Figures 3 and 4). The patient was transferred to the intensive care unit and was extubated six hours following the operation after careful monitoring of his vital signs. After awakening and extubation, the patient was in a very good state, with marked improvement of his arm function and speech. The following day, the patient was discharged from the intensive care unit and stayed hospitalized for one week. He was discharged from the hospital with a minor numbness of three fingers of his right hand on dual antiplatelet therapy consisting of 75 mg of clopidogrel and 100 mg of aspirin.
Internal carotid stenosis before and after a successful carotid artery stenting procedure. No technical defects are detected The extracted stent with thrombus occluding its lumen and fresh red thrombus from the internal carotid artery Final angiographic result of the carotid bifurcation after primary carotid closure Final angiography of the cerebral vasculature showing no arterial defects after carotid thromboembolectomy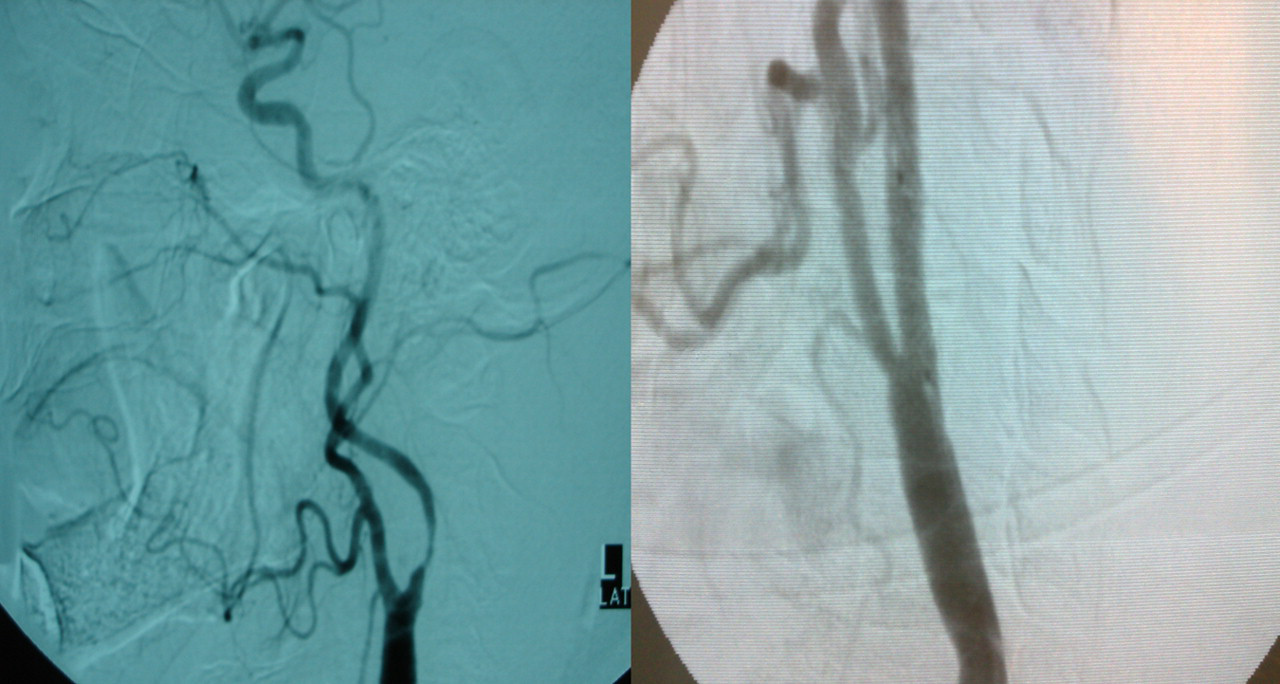

Discussion
We presented a case of successful surgical repair of an acute carotid thrombosis following CAS procedure with the use of thrombectomy with a Fogarty balloon catheter. Acute stent occlusion, like acute carotid occlusion after CEA, is a particularly rare complication which can have serious consequences to the survival of the patient. The direct and early diagnosis and treatment of this situation is of great importance for the prognosis and late morbidity of the patient. As soon as symptoms of neurological deficit at the side of CAS treatment appear, an imaging study in the form of triplex U/S should be conducted. If carotid thrombosis is revealed, aggressive systemic heparinization of the patient should be induced with bolus intravenous (intravenous) heparin, followed by continuous heparin infusion. Heparinization aims to suspend thrombus propagation in the vasculature of the cerebral tissue. For cases of severe deterioration of the clinical and neurological state of the patient, an urgent revascularization procedure should be decided upon. The dilemma rises when the patient is in a stable state with minimal signs of neurological deficit, as was the case of our patient. He was stable for 24 hours with no signs of worsening of his situation. This is why, at the beginning, we decided not to intervene urgently with any means of revascularization. At this point, we should point out the potential risk from various revascularization procedures, like clot dislocation from the thrombus with consequent cerebral embolization. This complication can be lethal and it is unjustified in a patient with minor symptoms, as in our case. Close monitoring of the vital signs of the patient together with frequent neurological re-evaluations are indicated. Upon any evidence of clinical and neurological worsening, an emergent revascularization procedure must take place.
Following a review of the literature in MEDLINE, since 2000, only 15 cases of treatment of acute carotid stent thrombosis after successful CAS, have been presented. 2–10 Various methods of revascularization are supported like percutaneous mechanical thrombectomy assisted by systemic abciximab infusion (n = 1), 7 thromboaspiration of fresh thrombus (n = 1) 2 and intra-arterial bolus injection of thrombolytic agent followed by continuous infusion in the clot (n = 5); 3,6,8 for one of the cases of Steiner et al., the thrombolytic agent was facilitated by abciximab injection and angioplasty of a previous in-stent stenosis. In addition, four cases of surgical thrombectomy with a Fogarty catheter together with extraction of the stent followed by routine CEA have been presented. In one of the patients of Setacci et al., 10 they managed to keep the stent in place following thrombectomy. Finally, Chaturvedi et al. 5 presented two cases of lethal carotid artery thrombosis, which stresses the severity of this infrequent complication.
In almost half of the patients presented in the literature (n = 8), with acute stent thrombosis following CAS, the underlying cause was failure in antiplatelet medication, either in the preoperative or the postoperative period. In all the other cases, several reasons were responsible, like metabolic and hematological disorders (thrombocytosis n = 3) and technical failure (dissection of the internal carotid distal to the stent, inappropriate stent position). Both patients that died from this complication were not under antiplatelet medication before or after the procedure. At this point, it is important to emphasize the importance of antiplatelet therapy in the perioperative period, as is clearly described in the European Society for Vascular Surgery (ESVS) guidelines for invasive treatment of carotid stenosis by Liapis et al. 11 Following CAS, the patient should be under dual antiplatelet medication with clopidogrel and aspirin for one month, followed by lifelong continuation of clopidogrel intake once daily. Our patient accidentally missed his doses after the procedure, resulting in stent thrombosis on the second postoperative day.
All the patients, except for the two lethal cases described, improved or resolved fully from their symptoms after successful cerebral revascularization. They were all treated within the first 48 hours of their symptomatology with aggressive systemic heparinization and various revascularization procedures. The results of all the cases presented so far in the literature are proof of the importance of direct imaging and aggressive treatment according to the clinical state of the patient. In our case, we favored Fogarty thrombectomy with stent removal, instead of mechanical percutaneous thrombectomy and intra-arterial thrombolysis, because we have great concerns regarding the possibility of clot fragmentation and cerebral embolization after restoration of flow from the carotid artery.
Conclusion
The above review of the literature underlines the fact that the use of classical vascular procedures like carotid thrombectomy can be helpful for neurorescue when we deal with infrequent, but sometimes lethal, complications, such as acute stent thrombosis. Direct diagnosis and urgent revascularization are the key elements for improvement of the symptoms because in these situations, ‘time is brain’.