
Abstract
Popliteal artery entrapment syndrome accounts for an important part of correctible causes of claudication and limb ischemia in young people. It is caused by an abnormal relation between the popliteal artery (PA) and the medial head of the gastrocnemius muscle. The diagnosis should be considered in any patient under 50 with calf claudication. The mainstay of treatment is prevention of PA fibrosis because if left untreated, the syndrome leads to irreversible damage to the PA with thrombosis and limb ischemia. We describe two cases of different types in 21- and 27-year-old males, respectively, and we review the literature about the presentation, diagnosis, classification and management of this entity.
Keywords
Introduction
Vascular entrapment syndromes are caused by an anomalous relationship between a vessel and surrounding tissues. When the popliteal artery (PA) is compressed with neighboring musculotendinous structures, most frequently with the medial head of the gastrocnemius muscle (MGH), PA entrapment syndrome (PAES) ensues with irreversible PA damage and ischemic-related symptoms in advanced cases. The syndrome is seen in a non-atherosclerotic ground in young healthy individuals. This outlines the importance of proper management to avoid impairment in quality of life.
We report two cases of PAES of different types, a bilateral type III case presenting with acute critical limb ischemia on one side and a unilateral type II case with intermittent claudication.
Case 1
A 21-year-old man with a history of active smoking was admitted to the emergency department for acute right foot pain associated with motor deficit of his toes. Four days prior to this event, he noticed progressive pain in his right calf as well as pain and paresthesia in his right foot occurring on moderate effort. The pain gradually increased and became constant on rest with a pale and weak foot. On physical examination, we noticed a cold right foot, with absent distal pulses and paresis of his toes. He underwent an urgent computed tomography (CT) angiography that showed total occlusion of the PA with medial deviation and compression against the medial femoral epicondyl (MFE) (Figure 1a). We also noted proximal occlusion of the tibialis posterior artery and distal occlusion of the tibialis anterior. PAES was suspected, and in view of the obstruction of his crural arteries and the fact that the motor deficit was restricted to the toes, the patient was transferred to the angio suite for urgent thrombolysis (Figure 1b). Successful lysis of the thrombus revealed an underlying severe stricture of the PA lumen, as well as marked medial deviation (Figure 1c). The contralateral PA, although normal, was also slightly medially deviated, and with dorsal flexion of the foot, a dynamic total occlusion could be induced (Figure 1d). A repeat angiogram 24 hours later showed complete lysis of the popliteal thrombus with restoration of distal flow through the tibialis posterior but incomplete dissolution of the tibialis anterior emboli. The patient was fully anticoagulated with heparin and followed by clinical surveillance and serial ankle-brachial index (ABI). Two days later, he underwent a magnetic resonance imaging (MRI) of both knees that confirmed bilateral type III PAES with compression of the PA by an accessory tendinous ligament originating from the MGH and having a proximal insertion over the lateral femoral epicondyl (Figure 1e).
(a) Computed tomography angiography showing right popliteal artery (PA) occlusion (arrow head) with its entrapment between accessory musclotendinous fibers from the medial head of the gastrocnemius muscle (MGH) (black arrow) and medial epicondyl of the femur (MFE). (b) Digital angiography showing complete occlusion of the right PA with marked medial deviation. (c) After thrombolysis, the right PA shows severe stricture. (d) Complete dynamic occlusion of the left PA with forced dorsiflexion of the foot. (e) T1-weighted magnetic resonance imaging showing right PA impingement (black arrow) between the MFE and accessory fibers of the MGH (white arrow), left PA (white arrow head) trapped between fibers of the left MGH and MFE
The following day, the patient was operated on for a popliteal bypass between the distal superficial femoral artery and the infrageniculate PA through a medial approach using his ipsilateral great saphenous vein (GSV) in a reversed position. The postoperative course was uneventful, the ABI was normal and the patient was discharged home. Two months later, he was admitted for a preventive entrapment release procedure on the left side using a posterior approach. The accessory musculotendinous ligament was resected and the PA freed from extrinsic compression. The patient was discharged home four days following his intervention with no complications. One year later, the patient was doing fine with distal palpable pulses.
Case 2
A 27-year-old healthy man presented to our outpatient clinic with a four-month histoiy of intermittent claudication of 800 m in his right calf. His past medical histoiy was relevant for obesity and an active smoking state (10 pack-years). Three weeks prior to presentation, he noticed worsening of his symptoms, with a reduced walking distance to 100 m and the apparition of right calf edema.
On physical examination, the right foreleg was slightly enlarged compared with the contralateral side. Popliteal, tibialis posterior and pedal pulses were absent on the right side.
He first underwent a duplex scan that revealed thrombophlebitis of the small saphenous vein and occlusion of the PA, with the absence of any cyst or aneurysm at this level. The ABI was 0.72 on the right side and 1.07 on the left. An arteriogram of the right lower limb showed a 5 cm occlusion of the PA at the level of the knee joint. PAES was suspected and the patient underwent an MRI of both knees. Type II PAES was confirmed on the right side where the MGH was compressing the PA against the MFE (Figure 2).
(a) Axial T2-weighted magnetic resonance imaging (MRI) of the knee showing popliteal artery (PA) (white arrow) occlusion and entrapment between the medial head of the gastrocnemius muscle (MGH) and medial epicondyl of femur (MFE). (b) Sagittal view showing the position of the PA between the MGH and MFE. (c) MRI angiography demonstrating right PA occlusion
The patient underwent a short bypass between the distal superficial femoral artery and the PA through a medial approach using the ipsilateral GSV that was harvested from the mid-thigh. The postoperative course was smooth; the duplex scan showed a patent graft. The right ABI was normal and the patient was discharged four days following his surgery. At six months, he was doing fine with normal distal pulses and has since been lost from follow-up.
Discussion
PAES accounts for an important part of correctible causes of claudication and limb ischemia in young people. In fact, it represents the second most common cause after atherosclerosis in patients younger than 50 years. The first description of the disease was in 1879 by a medical student (Anderson Stuart), 1 but it was not until 80 years later that the condition was recognized as a medical entity and the first surgical treatment was performed (myomectomy of MGH and PA endarterectomy). 2 In 1969, Love and Whelan 3 gave the disease the name ‘popliteal entrapment syndrome’.
It was once believed to be a rare condition, until Bouhoutos and Daskalatis 4 reported an incidence of 0.165% of young men entering the Greek army.
Young athletes suffering from claudication will have PAES as an underlying cause in 60% of cases. 5
There is a net male predominance with a 9:1 ratio. 6 Bilateral involvement occurs in about 25% of cases. 6 Four types have been described based on embryology; they are the result of an abnormal early development of the PA by the fusion of the posterior and anterior tibial arteries. This fusion, which normally occurs after the migration of the MGH, will lead to the occurrence of the first three different types of PEAS depending on the stage of MGH migration. Type I (50%) is associated with a marked medial course of the PA in the popliteal fossa with a normal position of the MGH. The PA fusion occurs very early in development and is later on pushed medially by the medial migration of MGH.
Type II (25%) occurs when the PA lies medially to an abnormally placed MGH. Is this case, the MGH could have variable attachments to the lateral aspect of the MFE, the intercondylar area or the lower aspect of the femur. The fusion of PA occurs at a stage after the MGH has started to migrate but not reached its normal definitive position. The prematurely formed PA arrests the migration of the MGH, resulting in this type of PAES.
In type III (6%), the PA is entrapped between the accessory slip of the MGH or even a double MGH. This happens when the fusion of the PA occurs during MGH migration.
Entrapment of the PA deep to the popliteus muscle independently of the MGH results in type IV PAES; this represents the least common type but is the most aggressive to the PA. 7 This type is found with persistence of the axial primitive PA deep into the popliteus muscle.
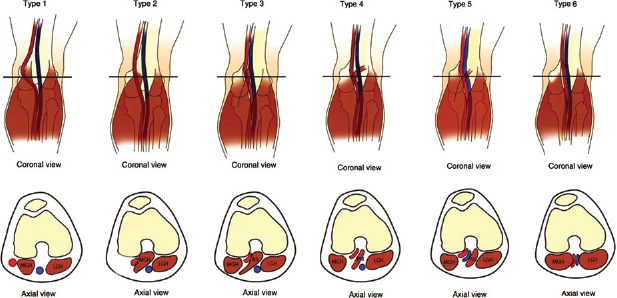
Two other types have been described: type V when any of the four types includes entrapment of the popliteal vein and type VI which occurs without anatomic abnormalities and is often called functional PAES (Figure 3).
Coronal and axial views of different types of popliteal artery entrapment syndrome (PAES) (LGH, lateral gastrocnemius head; AS, accessory slip of MGH; PM, popliteus muscle). Type 1: normal attachment of MGH, medial course of PA. Type 2: lateral attachment of MGH, PA medially deviated. Type 3: PA between accessory slip of MGH. Type 4: PA posterior to PM. Type 5: any PAES involving popliteal vein (type 3 in this case). Type 6: hypertrophied gastrocnemius muscles entrapping normally localized PA (with permission from Kim et al.)
11
The most common symptom is calf claudication 7 as was seen in our second case. Foot blood supply can still be ensured via collateral vessels that reinject the distal PA and prevent critical limb ischemia. The latter is a rare presentation and occurs with distal embolization. 7 The emboli result from a focal thrombus formation at the entrapment site or from poststricture aneurysm formation. 8 This was the case for our first patient who most probably had worsening of his symptoms with emboli shedding into the distal crural vessels.
Angiography is the classical investigation tool. It may demonstrate medial deviation of PA, signs of irregularities or occlusion and evaluate distal runoff. While angiography gives indirect findings suggesting PAES, dynamic CT angiography and MRI are better used for identifying the anatomical relation between the PA and MGH; they also recognize adventitial cysts which mimic PAES, and are equivalent to angiography in identifying occlusions. 8 All these tests should be performed with forced dorsiflexion of the foot with a fully extended knee to demonstrate the abnormality. This was typically seen on the asymptomatic side of our first patient.
Since the pathology is encountered in both legs in 25% of cases, bilateral knee imaging is mandatory.
With time, progressive fibrosis of the PA occurs and leads eventually to occlusion or aneurysmal formation. For that reason, surgery is advised in all diagnosed anatomical types (I–V). This process also explains why bypass of a fibrotic PA with GSV has better long-term outcome than repair or patch plasty.
All anatomical PAES should be surgically treated. 5 Treatment strategy depends on the level of PA degeneration. When the PA is undamaged and patent or represents stage 1 degeneration (scaring of the adventitia alone), exploration of the artery and resection of the entrapment mechanism is recommended. This requires, in most cases, an MGH myotomy with or without medial implantation. Excellent long-term follow-up is reported without any functional morbidities.
In stage 2 (medial) and 3 (intimai) fibrosis, replacement of the PA with a GSV bypass is advised. 9 While patch repair could be attempted in some minor abnormalities, marked thickening, aneurysm formation distal to entrapment site and luminal irregularities are better treated with a bypass. Once the artery is occluded, repair is almost always inappropriate. 7 Both our patients had severe stricture not amenable to repair.
Type VI PAES should not be treated unless symptoms occur. Treatment consists of surgical myotomy of the MGH. 9
Both medial and posterior approaches could be used. The former is better used in case of long occlusion where a long bypass is needed. 7 This was the case for our second patient with a 5 cm occlusion, adding the advantage of avoiding anesthetic morbidity of a prone position in an obese patient. Other advantages include more rapid return to activity and better harvest of the GSV. For this reason, we also opted for a medial approach in the first patient. The posterior approach gives a better exposure of structures and appreciation of anatomy with a less prominent scar but at the expense of greater surgical morbidity. 6 It is better used when repair of the artery is planned or in case of short occlusions. We preferred this approach on the asymptomatic side of our first patient since he only needed resection of the musculotendinous band to release the PA.
With GSV bypass, excellent long-term results are expected, with almost 100% patency rate at 10 years versus 67% for thromboembolectomy and patch plasty of the PA. 10
Conclusion
The diagnosis of PAES should be considered in any patient under 50 with calf claudication, especially in individuals without cardiovascular risk factors. Once PAES is diagnosed, treatment should always be considered in all types I to V and in symptomatic type VI.
Vein bypass is the preferred choice of therapy in most symptomatic cases. Prophylactic PA release is always indicated in asymptomatic anatomical cases.