
Abstract
True aneurysm formation in arterialized autologous veins is an unusual complication. A saccular aneurysmal degeneration of 53 mm (maximal diameter) of a saphenous vein graft inserted for repair of a popliteal aneurysm, four years after implantation, is reported. The patient (with prior history of abdominal aortic aneurysm) had been initially treated through a posterior approach. A new saphenous vein bypass grafting (medial approach) was performed. Histological examination revealed myointimal fibrosis, medial degeneration and inflammation. In spite of the widespread use of the autologous saphenous vein as an arterial substitute, this complication is extremely rare and its etiology remains unclear. Atherosclerosis is considered to be the main cause of aneurysm formation in vein grafts, but current data suggest that additional etiopathogenic factors should be further investigated. We note the rarity of this finding and review the literature for true aneurysm formation within vein grafts used for bypass procedures.
Introduction
Popliteal artery aneurysms (PAAs) are the most common form of peripheral arterial aneurysms and the clinical presentation includes embolism, thrombosis and rupture. Treatment of PAAs involves either a conservative management protocol or a more aggressive intervention such as surgery. The presence of a suitable vein should be checked before deciding to operate and conventional aneurysm repair consists of either opening the aneurysm sac and interposing a bypass graft or aneurysm ligation combined with bypass grafting.
Compliance and caliber mismatch between native vessel and vein graft, as well as anastomotic line stress concentration, contribute toward unnatural wall shear stress. Degenerative changes of the saphenous vein grafts include endothelial desquamation followed by fibrin deposition or platelet adhesion, mural edema and extensive medial and adventitial degeneration. As a consequence, intimal hyperplasia (proliferative process of vascular smooth muscle cells) can occur after bypass grafting, particularly at outflow anastomoses, and it leads ultimately to graft flow reduction and thrombosis.
Non-anastomotic aneurysm formation in autogenous vein grafts, although rarely described, has also been uniformly associated with advanced atherosclerotic changes of the vein wall, although these changes (such as endothelial disruption, subendothelial cholesterol deposits, medial necrosis and fibrous proliferation) in venous conduits commonly take the form of occlusion rather than aneurysm. In general terms, aneurysmal dilation of saphenous vein grafts following infrainguinal revascularization mostly represents false anastomotic aneurysms, 1 with true aneurysms being an unusual complication. They have been more frequently reported in veins used for coronary artery bypass grafting, 2 at an estimated rate of <1% per year.
The management of vein graft aneurysms in lower limbs should be subject to the same criteria that apply to other aneurysms because once vein graft dilation occurs, it is followed by a rapid increase in size, which may lead to possible rupture. With proper diagnosis and surgical treatment of these true aneurysms after repair for a PAA, excellent limb salvage and postoperative function should become the norm.
Case report
We report the case of a 67-year-old man, with hypertension, a smoking habit and dyslipidemia on treatment (statins) as cardiovascular risk factors, and a prior medical history of chronic atrial fibrillation and Hodgkin's lymphoma treated with radiotherapy 20 years earlier (currently on complete remission). He had undergone an aorto-bifemoral bypass, because of an infrarenal abdominal aortic aneurysm (AAA) five years ago.
In the subsequent four-year period, he also underwent surgical repair of a bilateral PAA: the right one was repaired by posterior endoaneurysmorrhaphy and reconstruction with end-to-end anastomoses using an autologous great saphenous vein graft; three years after the contralateral repair, the left one (which extended above the Hunter canal) was treated by a medial approach using a reversed saphenous vein graft, with previous ligation of the PAA. The quality of the vein conduit was defined as not varicosed.
On follow-up, a minimum increase of diameter at the proximal portion of the right venous graft was revealed at a subsequent duplex scan (one per year). A first computerized tomography scan was carried out because of a new clinical finding at the fourth year: the presence of an expansive popliteal pulse at physical examination. It revealed a saccular aneurysm at the proximal portion of the right saphenous vein graft (Figure 1), with three distal outflow arteries. The aneurysm developed four years following the bypass procedure and it expanded 53 mm (maximal diameter). The graft was still patent when the patient was examined.
Three-dimensional reconstruction. Saccular aneurysm of the right saphenous vein graft (53 × 45 mm, maximal diameter) and patency of the graft were demonstrated. The total exclusion of the previous right popliteal aneurysm was proved. The proximal anastomosis is indicated (white arrows). The left femoropopliteal bypass was patent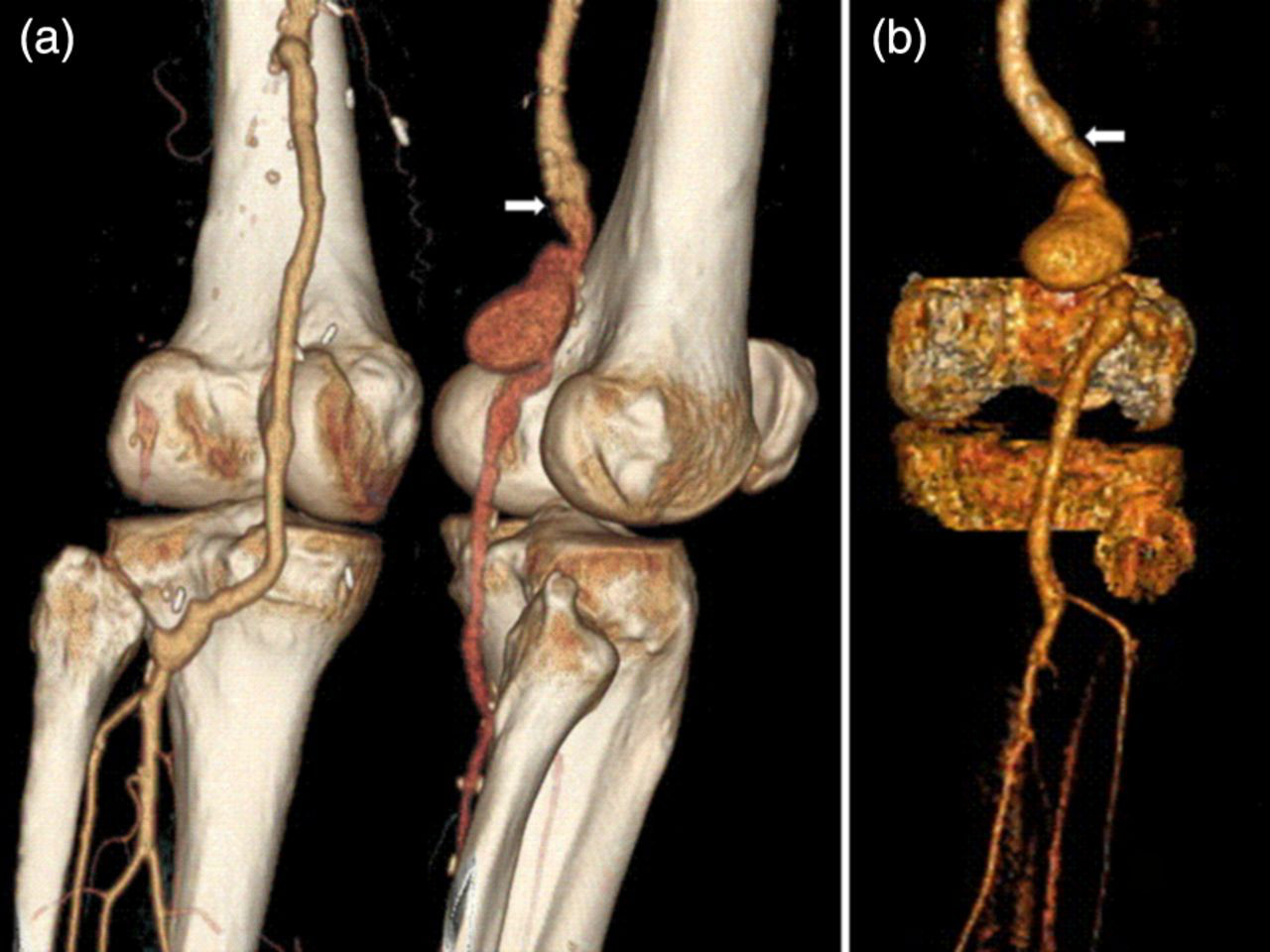
After this finding, he underwent surgery: a combined supragenicular and infragenicular incision at the medial side of the right leg was performed and the true aneurysm was exposed (Figure 2). The proximal suture line was intact, and so a differential diagnosis with false aneurysms was made. The patient received 5000 IU of heparin before the aneurysm was cross-clamped. Exclusion and ligation of the vein graft aneurysm was performed, with placement of a femoropopliteal bypass using reversed saphenous vein from the ipsilateral leg. The distal anastomosis was to the below-knee popliteal artery.
Intraoperative findings: the ectatic graft segment is shown. The proximal suture line was intact and the absence of a pseudoaneurysm was proved at surgery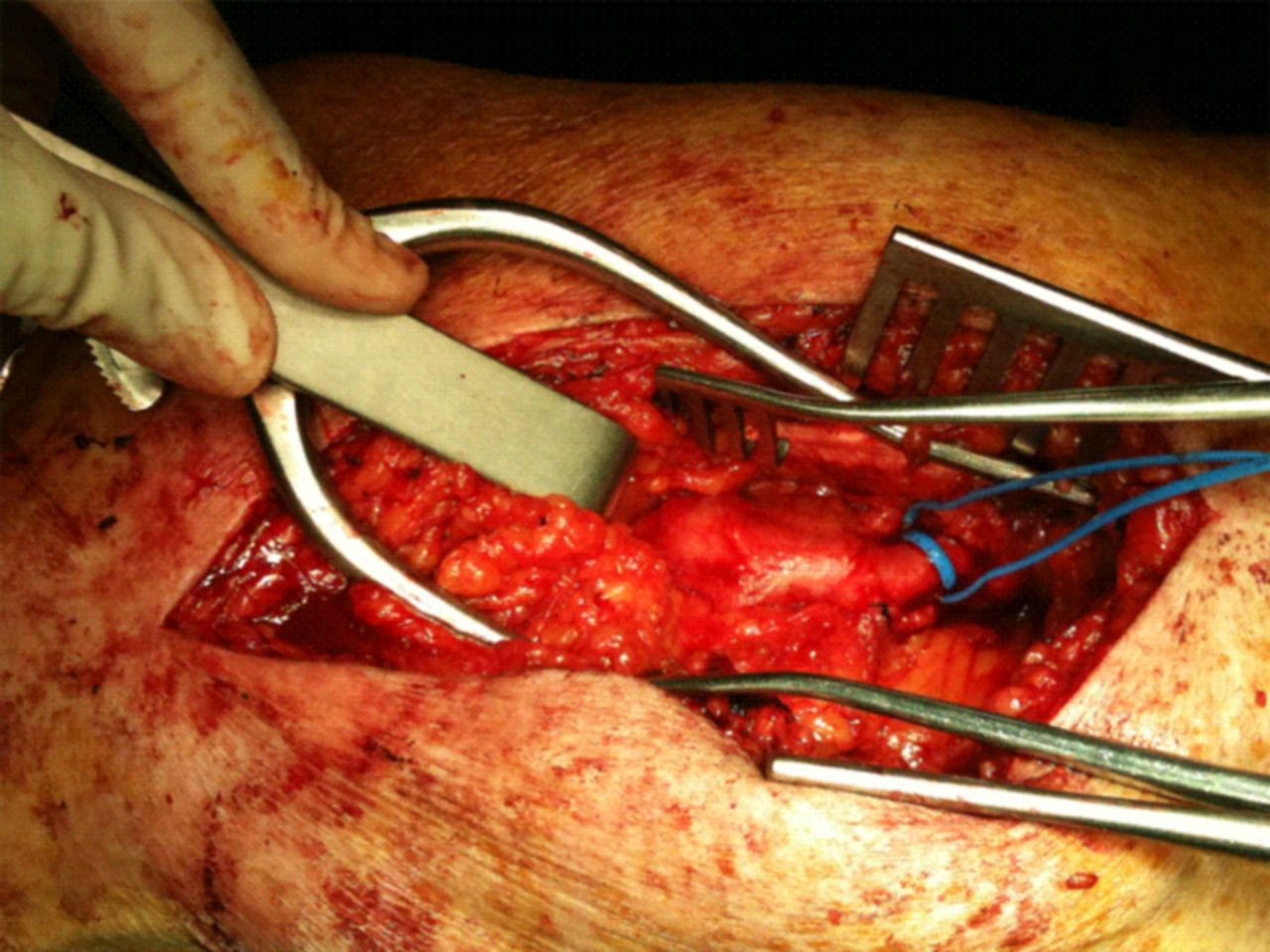
The histopathological examination of a segment of aneurysmatic vein graft revealed myointimal fibrosis, medial degeneration and inflammation. Five days after surgery, a duplex scan revealed a complete exclusion of the venous aneurysm with an excellent blood flow through the bypass and distal arteries, including dorsalis pedis. The patient had a full recovery and is currently asymptomatic two months after surgery.
Discussion
Great saphenous vein and endoaneurysmorrhaphy continues to be the gold standard for open repair of PAA. Elective surgical repair with the vein graft has patency rates more than 90% in a contemporary series and offers the most successful operative therapy. The 2-, 5- and 10-year primary patency rates were 94.3, 87 and 86% (saphenous vein graft) and 61.5, 57 and 50% (prosthetic graft). 3–5 Posterior and medial approaches have demonstrated similar long-term results with regard to restenosis and limb salvage, 6 but there are no data in the literature about a possible role for development of true aneurysms of saphenous vein grafts between the two approaches.
In general terms, arterialized autologous veins are at risk of degenerative changes because of histological differences with arteries. The thickness of the three layers (tunica intima, media and adventicia) varies greatly depending on the type of vessel. The tunica media is the layer of concentrically arranged smooth muscle, the autonomic control of which can alter the diameter of the vessel and affect the blood pressure. The tunica media of arteries is larger than that of veins of similar size and makes the veins more susceptible to aneurysmal degeneration. Moreover, the tunica adventitia is made chiefly of longitudinally arranged collagen fibers and tends to be much larger in veins than arteries.
The pathogenesis of true aneurysmal dilation remains speculative, with consideration given to peri-operative graft trauma, weakness at valve sites, ‘blow-outs’ at side-branches or progression of underlying atherosclerosis within the venous graft itself. Advanced atherosclerotic changes are commonly subendothelial cholesterol deposits, lipid-laden macrophages, fibrous proliferation, ulcerations and loss of elastic lamina. Traditionally, arterial infection has been a cause for saccular aneurysms, and treatment options include in situ grafting either with prosthetic or autogenous grafts or with cryopreserved allografts, resection of the aneurysm with remote bypass grafting and ligation. Nevertheless, although non-atherosclerotic saccular vein graft aneurysms after repair of PAAs have been reported, 7 as well as in the setting of infectious endocarditis, 8 a correlation between the morphological characteristics of these venous aneurysms and the etiopathogenic factors has not been revealed yet. In our patient, no clinical data of systemic or in situ infection were demonstrated.
The development of a true aneurysm following the repair of a PAA occurs infrequently (less than 1%) and massive aneurysm degeneration is even more uncommon. 9 It is usually asymptomatic and may occur especially in patients with hypercholesterolemia and hypertriglyceridemia; because of this reason, an optimal management of the hyperlipidemic state is mandatory in all vascular patients. 10 In situ or reversed saphenous vein grafts can be affected by aneurysmal degeneration, 11 and surgical repair (with a new venous or prosthetic graft) seems to be the optimal treatment in most cases, 12 although the use of eversion endarterectomized superficial femoral artery has been reported as a substitute interposition graft when no adequate vein is available. 13 The insertion of an expanded polytetrafluoroethylene-covered nitinol endoprosthesis has also been reported in a small number of cases, but long-term results are yet unknown. 14
Varicosities of saphenous vein usually also increase the risk of aneurysm formation. External reinforcement with a Dacron prosthesis seems to allow the use of autogenous saphenous veins (with varicose dilation) without compromising graft patency and limb salvage. 15 In modern vascular surgery, the use of a cryopreserved saphenous vein allograft or human umbilical vein is an alternative option. 16 Although a considerable rate of early thrombotic occlusions have been reported, excellent secondary graft patency and limb salvage combined with a tolerable rate of late aneurysmal degeneration justify the use of the human umbilical vein in femoropopliteal bypass surgery when autogenous vein is not suitable. 17 Dardik et al. 18 have updated their experience with 907 human umbilical vein bypass grafts, which suggests that ‘clinically significant’ aneurysms occur in only 6% of the grafts followed for five years. Aneurysmal rupture, however, is an extremely infrequent event. 19
It has also been hypothesized that vein graft aneurysms may be a manifestation of a systemic dilating process 20 (involving both arterial and venous dilation), although it has been described to be atherosclerotic in nature in a large number of cases. A generalized arteriomegaly (detected on abdominal aorta, iliac arteries, femoral and contralateral popliteal arteries) has been demonstrated in patients with PAAs. Moreover, saphenous vein grafts implanted in patients with PAAs have significantly greater diameters than grafts implanted in those with peripheral arterial occlusive disease. 21 In our patient, the size of the contralateral venous graft (which had been interposed only one year ago) had not increased yet. Perhaps more time is necessary for evidence of aneurysmal degeneration, as the venous graft affected by the true aneurysm reported had been interposed four years earlier: it highlights the importance of a continual surveillance of these bypasses over time.
We can see aneurysmal degeneration of the vein graft in patients with PAAs, but it can also occur in patients with arterial occlusive disease. 22 Autogenous vein used for infrainguinal reconstruction in aneurysmal disease demonstrates an altered adaptive response (and a higher five-year primary graft patency) compared with those patients who undergo reconstructive surgery for occlusive disease, potentially altering graft patency. These data suggested altered remodeling of vein grafts in patients with PAAs, which may have a beneficial effect on patency. 23
The popliteal artery is more susceptible for aneurysm development than other peripheral muscular arteries, but the etiopathogenic factors are unknown. The wall properties of this artery are affected by age and gender, with an increase in diameter and a decrease in distensibility; 24 this seems not to be the behavior of a true muscular artery, but of a central elastic artery (such as the aorta). These findings lend support to the view that there is a generalized dilating diathesis in patients with aneurysmal disease that may be unrelated to atherosclerosis. 25
It might have implications for susceptibility to arterial and venous dilation, as well as the association of aneurysm formation between the aorta and the popliteal artery. Despite our patient not having a connective tissue disorder or a previous family history of connective tissue disorder, his past medical and surgical history does not prove a causal relationship, but they do provide additional support for the hypothesis of a systemic dilating process. The histopathological findings suggest that progressive atherosclerosis is not the likely cause of aneurysm formation in this case.
Because of the high incidence of extrapopliteal aneurysm, patients with PAAs should undergo a thorough search for aneurysms at other sites. In 30–54% of cases, an AAA is associated. 26,27 Inflammatory and proteolytic processes have been involved in aneurysm growth. AAAs and PAAs are characterized by a marked activation of proinflammatory transcription factors (nuclear factor-kappa B and activator protein-1); hyperexpression of interleukins (IL-6 and 8); and increased matrix metalloproteinase (8 and 9) and cathepsin K, L and S expression and activation. 28 Current epidemiological associations between AAAs and PAAs suggest that these two clinical entities share common grounds and exhibit a general proinflammatory profile.
Long-term follow-up is recommended in patients following the repair of PAAs because of propensity for recurrence of aneurysms in the residual or contralateral popliteal artery and to rule out extrapopliteal aneurysm formation, such as AAAs or dilation of the saphenous vein graft when it had been used.
Declarations