
Abstract
The aim of this paper is to illustrate a rare case of primary aortoenteric fistula in the presence of disseminated infection and review the critical decision-making process. A clinical case was reviewed for its initial presentation, planning of treatment strategy and outcome. A secondary literature search for discussion on current accepted recommendations for primary aortoenteric fistula was then completed. Aortoenteric fistulas are rare pathologies with highly morbid potential. Their diagnosis requires a high index of suspicion and prompt intervention is critical to patient survival. In conclusion, aortoenteric fistula most commonly arises from large atherosclerotic aneurysms but can be caused by systemic infection. In the case of the latter, extra-anatomic repair appears to be the treatment of choice.
Introduction
Primary aortoenteric fistulas (PAEF) are connections between the gastrointestinal tract and the aorta without the presence of an implanted device. Though extremely rare with a reported incidence of 0.04%, PAEFs have the potential for disastrous outcomes, making early diagnosis and emergent intervention crucial in their management. 1 Unfortunately, the clinical presentation of abdominal pain, a pulsatile mass and large herald bleed is identified in only a minority of cases, making the diagnosis exceedingly difficult. 2 A large number of cases are not identified until the time of laparotomy.
The most common cause of a PAEF is secondary to a large atherosclerotic abdominal aortic aneurysm. A small minority of cases have been attributed to disseminated blood infections such as tuberculosis (TB) and syphilis. 1 Infectious etiologies have raised concern regarding the best method of repair at the time of surgery, specifically whether an anatomic or extra-anatomic bypass should be utilized for vascular reconstruction. We present a case of disseminated Mycobacterium bovis (bacillus Calmette-Guérin [BCG]) and a presumed mycotic abdominal aortic aneurysm, as well as a review of the literature.
Case report
A 62-year-old man presented to the emergency department with a one-week history of abdominal pain partially relieved by proton pump inhibitors. In addition, he reported two episodes of bright red blood per rectum that began the morning of presentation. He had had no prior history of bloody stools or prior abdominal surgery. His past medical history revealed a known infrarenal abdominal aortic aneurysm (AAA) of 2.8 cm at the time of his most recent imaging study. He also had a history of recurrent bladder cancer which was treated with intravesicular BCG in 2007. As a result of this therapy, the patient was subsequently found to have disseminated mycobacterium with granulomas noted in the bone marrow and liver. He had undergone treatment with one year's worth of antibiotic therapy, which had been completed over three months prior to the current presentation.
On physical exam, his vital signs were within normal limits (heart rate 86, blood pressure, 122/87) and the patient was in no distress. His exam was significant for a palpable abdominal aorta without any abdominal pain to palpation. He had no external hemorrhoids, but gross blood was identified on rectal exam.
A computed tomography (CT) scan of the abdomen and pelvis without contrast was obtained due to mild renal insufficiency. The CT scan identified enlargement of his previously noted AAA to 4.1 cm with an irregular contour. In addition, there was disappearance of the fat plane between the aorta and the third portion of the duodenum, raising concern for an aorto-enteric fistula (Figure 1).
Computed tomography (CT) findings raising concern for an aortoduodenal fistula. CT of the abdomen and pelvis without contrast, demonstrating irregular border of the abdominal aortic aneurysm (AAA) and disappearance of lucency between the AAA (note calcifications in AAA wall) and duodenum
The gastroenterology service was consulted for further evaluation of this patient's gastrointestinal bleed. The patient underwent an endoscopic gastroduodenoscopy that same evening which revealed a 2 cm area of discolored mucosa in the third part of the duodenum with an 8–10 mm size fresh clot seen in the middle of this area (Figure 2). The endoscopy was interpreted as being consistent with an aortoduodenal fistula.
Endoscopic findings raising concerns for an aortoduodenal fistula. Endoscopic gastroduodenoscopy demonstrating a 2 cm area of discoloration and adjacent fresh clot
Upon completion of the endoscopy, the patient was urgently taken to the operating room for definitive repair. In the operating room, multiple granulomatous lymph nodes were found throughout the small bowel mesentery. An area of adhesion between the third portion of the duodenum and the aneurysmal infrarenal abdominal aorta was identified. After proximal and distal control of the aorta was obtained, the duodenum was approached from its fourth portion and dissected from the upper aspect of the inflammatory aortic aneurysm. The area of the fistula was approximately 1.5 cm wide (Figure 3). The duodenum was noted to be thickened and scarred (Figure 4). It was debrided and repaired transversely in two layers. Next, the aorta was opened, and the wall was found to be grossly abnormal with concern for infection. The decision was made, therefore, to perform an extra-anatomic bypass and to ligate the aorta by oversewing both the proximal end below the renal arteries and the distal end at the aortic bifurcation. A large piece of omentum was harvested to cover the aortic stump at the level of the renal arteries. An axillobifemoral bypass graft using an 8 mm ringed polytetrafluoroethylene graft was then placed after the abdomen was closed.
Aortoduodenal fistula seen intraoperatively. Intraoperative view of the aortoduodenal fistula after the duodenum was dissected off the aorta with a visible tract between the two Intraoperative view of duodenum (third portion). After obtaining proximal and distal aortic control and separating the third portion of duodenum from the aneurysm, a 2 cm opening in the duodenum was demonstrated (end of left forceps spans duodenal opening), which marked the aortoduodenal fistula's location. A significantly thickened duodenal wall was noted and was excised before closing the duodenum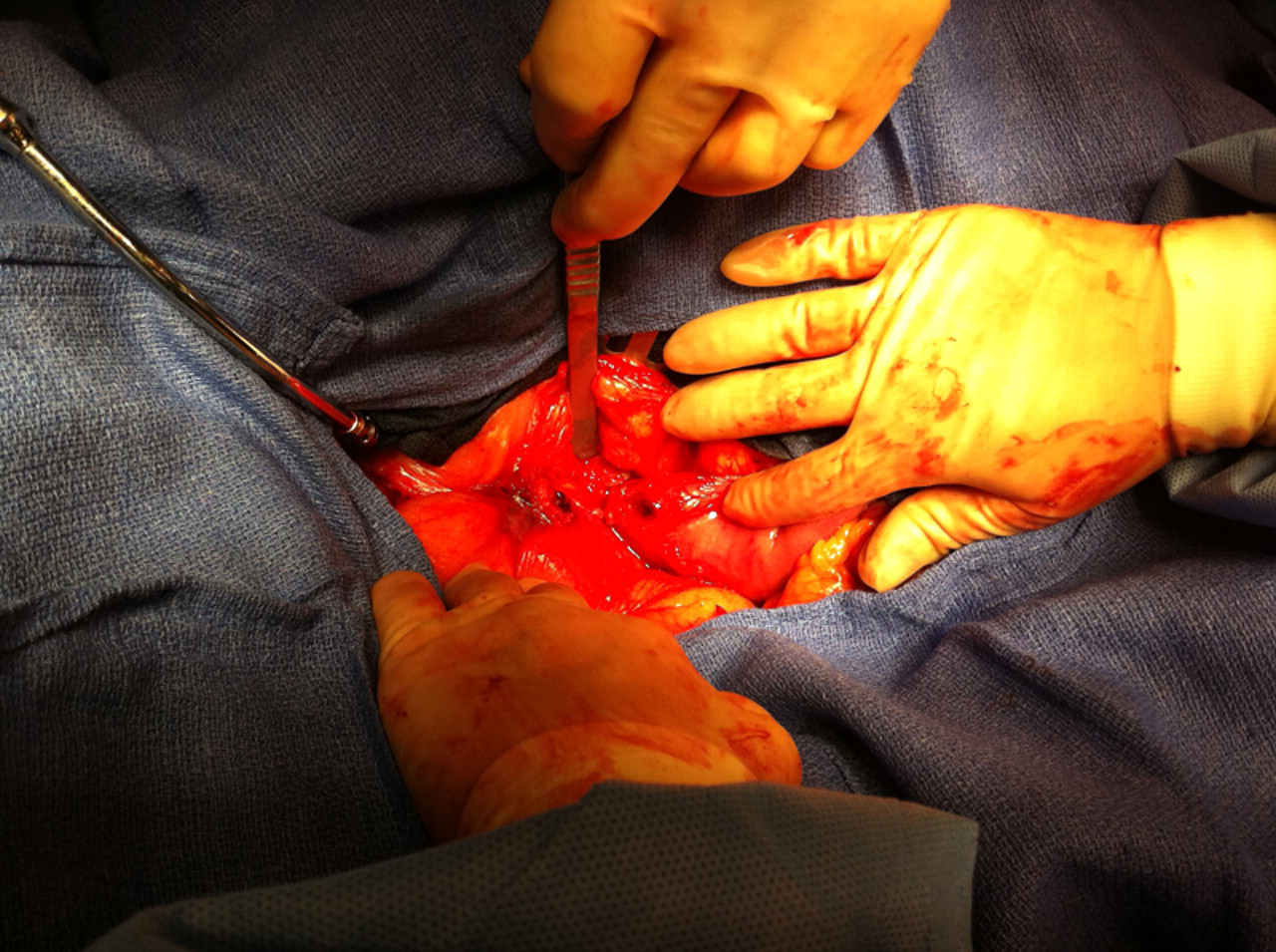

The patient was started on total peripheral nutrition postoperatively and closely monitored for several days. He maintained palpable distal pulses in both feet and remained afebrile and hemodynamically stable throughout his course. On postoperative day 10, the patient passed a gastrografin upper gastrointestinal study and was started on a clear liquid diet. He was subsequently advanced to a general diet without any difficulties.
Culture and tissue samples obtained from both the aorta and the adherent duodenum were negative for mycobacterium, fungus or bacterium. They did, however, demonstrate non-caseating granulomas with giant cells consistent with the patient's previous biopsy results. Tissue culture from the abdominal wall did grow Staphylococcus lugdunensis for which he was started on vancomycin for four weeks. Blood cultures were obtained postoperatively and were negative. He was also restarted on isoniazid, ethambutol, pyridoxine and rifampin for one year for presumed failure of his previous treatment for disseminated BCG. He was discharged on postoperative day 16 to a skilled nursing facility for completion of his intravenous antibiotic course.
Discussion
PAEF are exceedingly rare, with only around 300 reported cases in the literature. The majority are located in the third portion of the duodenum given its proximity to the aorta. 2 They are most commonly associated with an aortic aneurysm (mean size 6.2 cm) and are generally found to be atherosclerotic in nature. While aneurysms are the most common etiology, other causes such as mycotic aneurysm, radiotherapy and tumors have also been reported. 2 The classical triad of a gastrointestinal bleed, abdominal pain and a pulsatile mass are present in the minority of cases, making diagnosis extremely difficult. 2 A herald bleed is often reported but the duration between such a bleed and massive blood loss is highly variable. Additionally, with the multitude of more common etiologies of such symptoms, the possibility of a PAEF is often low on the differential diagnosis list.
The diagnosis can be challenging and a high index of suspicion is often required, particularly in a hemodynamically stable patient. Abdominal CT is the gold standard of diagnosis, though identification is quite difficult and confirmatory testing may be necessary. Some authors advocate a dual evaluation with CT scans and endoscopy as a means of ruling out other etiologies and for a thorough investigation of the duodenum. 1,3 Endoscopic evaluation proved to be integral in identification, as well as confirmation, of the diagnosis in our case.
This is a unique case of PAEF in that it was found to be secondary to disseminated BCG after intravesicular therapy for non-invasive bladder cancer. While other cases in the literature have been attributed to disseminated bloodstream infections, most commonly tuberculosis, our extensive literature review revealed only one other case of a PAEF after intravesical BCG therapy for bladder cancer. 4 Intravesical BCG is an effective therapy for bladder cancer with relatively low complication rates reported. 5 Disseminated BCG and BCG-related mycotic aneurysms have been discussed in the literature, although their rates of occurrence remain less than 1% of cases.
The question raised in our operative planning was whether to proceed with an in situ repair or if an extra-anatomical approach was necessary due to the concern for infection. As the aorta was opened, it was evident that the wall was abnormal and worrisome for infection. Prior literature has advocated avoiding an in situ graft when gross infection is identified. 1 An extra-anatomic bypass was determined to be the safest form of repair. As was found in our case, it is not uncommon for blood cultures to remain negative in disseminated BCG infection while non-caseating granulomas are found in liver and bone marrow biopsies. 5 Postoperative pathological review of the aortic and duodenal specimens confirmed the presence of non-caseating granulomas and validated our choice for repair.
With recent advancements in endovascular intervention for aortic pathologies, many practitioners have questioned its potential role in aortoenteric fistulas, especially as a bridging procedure to temporarily control bleeding in unstable patient populations. The mainstay of therapy has traditionally been open graft excision with either extra-anatomic bypass or in situ graft repair, both with concomitant duodenal repair. A few small series have looked at the effectiveness and outcomes of endovascular repair as compared with traditional open repair for aortoenteric fistulas. Baril et al. found similar complication rates between the two groups with shorter length of stay in the endovacular group. Unfortunately, the median survival rates in patients undergoing endovacular repair was significantly shorter when compared with those undergoing open repair, possibly due to their poorer clinical condition at presentation. 6 In their respective series, Burks et al. 7 and Danneels et al. 8 came to a similar conclusion that reinfection rates are high in endovascularly repaired AEF and that endovasular repair should be reserved for patients with no evidence of sepsis or used as a bridging technique to stabilize a patient with gross infection until a definitive procedure with duodenal repair can be performed. In our case, the patient was stable at the time of intervention and infection was a legitimate concern given his recent disseminated mycobacterium infection. As such, current literature would support a traditional open approach with extra-anatomical bypass.