
Abstract
The purpose of this study was to evaluate outcomes of the endovascular treatment of splenic artery aneurysms (SAAs) and pseudoaneurysms (SAPAs). From April 2003 to December 2009, 12 patients (mean age 46.8 years, range 29–58) with SAAs (n = 9) or SAPAs (n = 3) underwent endovascular treatment. Four patients were asymptomatic and three had ruptured aneurysms. Lesions were in the proximal splenic artery (n = 3), intermediate splenic artery (n = 3) and distal splenic artery (n = 6). Endovascular procedures included embolization by sac packing (n = 5), sandwich occlusion of the splenic artery (n = 4) or stent graft deployment (n = 3). Computed tomography (CT) was done before the operation, 3 and 12 months after the operation, then yearly. Endovascular treatment was successful at the first attempt in all 12 (100%) patients, with complete angiographic exclusion of the aneurysm at the end of the operation. The mean amount of contrast medium used was 165 mL (range 100–230), and the mean total procedure time was 92 minutes (range 55–160). No major complications occurred. Postoperational CT scans showed splenic multisegmental infarcts in eight patients (66.7%, 8/12) and among them postembolization syndrome developed in six patients, manifesting as abdominal pain and fever. The mean follow-up was 32 months (range 9–51). No patient demonstrated gross evidence of aneurysm sac growth, and no significant decrease in aneurysm sac size postintervention was noted on follow-up. The endovascular management of SAAs and SAPAs is safe and effective and may induce less mortality than open surgery. Regardless of the etiology, endovascular treatment can provide excellent mid-term results.
Introduction
Splenic artery aneurysms (SAAs) and pseudoaneurysms (SAPAs) are rare but clinically important because of the risk of rupture. Open surgical repair of these aneurysms remains the gold standard, yet with high perioperative mortality and morbidity rates. 1 Endovascular treatment of SAAs and SAPAs has been reported in recent years only from case reports and small series. 2–5 Our aims were to review the endovascular treatment of 12 consecutive patients in our center, and to retrospectively evaluate the effectiveness, immediate advantages and mid-term outcomes of this procedure.
Materials and methods
Patients
Between April 2003 and December 2009, 12 consecutive patients were admitted to our department for treatment of SAAs (n = 9) or SAPAs (n = 3). There were four men and eight women, with a mean age of 46.8 years (range 29–58). Among the SAA cases, three were probably atheromatous, and three had portal hypertension. For the three SAPA cases, the predisposing factors were chronic pancreatitis (n = 1), acute pancreatitis (n = 1) and surgery (n = 1). The diagnosis of SAAs or SAPAs was established in all patients by computed tomography (CT) with contrast medium injection. At presentation, 44% (4/9) of SAA patients were symptomatic, but all (3/3) SAPA cases were symptomatic. Three patients experienced rupture of their lesions; one presented with hemorrhagic shock and two presented with acute abdominal pain. The diameter of the lesions varied widely, with no obvious correlation to the clinical presentation: 2–4.5 cm for ruptured lesions, 3–6.5 cm for unruptured symptomatic lesions and 3–3.5 cm for asymptomatic lesions. Three lesions (two SAAs and one SAPA) were located in the proximal segment of the splenic artery; three (two SAAs and one SAPA) were in the intermediate segment and six (five SAAs and one SAPA) were in the distal segment. The main clinical data are reported in Table 1.
Clinical data, angiographic findings and outcomes of endovascular treatment in 12 patients with SAAs or SAPAs
A, aneurysm; NBCA, N-butyl-2-cyanoacrylate; PA, pseudoaneurysm; PES, postembolization syndrome; SAA, splenic artery aneurysm; SAPA, splenic artery pseudoaneurysm; SMA, superior mesenteric artery
Technique
All 12 patients underwent emergency or planned diagnostic angiography and underwent same-stage endovascular treatment. Endovascular access for all procedures was through the femoral artery (n = 8) or brachial artery (n = 4). A 6F sheath (n = 9) was used in most cases, and a 7F (n = 3) sheath was used in the rest. A shaped guiding catheter was used selectively in the ostia of the visceral vessel in instances where a sheath could not successfully be engaged. Selective angiography of the celiac trunk, splenic artery and superior mesenteric artery was performed at first.
In four patients, the splenic artery was embolized on either side of the aneurysm (‘sandwich technique’) to prevent retrograde filling (Figure 1). Embolization was achieved using a superselective coaxial technique with a 2.9F microcatheter (ProgreatTM, Terumo, Leuven, Belgium). Embolization was performed with detachable, 0.018-inch, soft, platinum, multiple-curled microcoils (Cook Inc, Bloomington, IN, USA) of various lengths and diameters.

Sandwich technique. (a) Embolization of the distal splenic artery with microcatheter and coils. (b) Embolization of the proximal splenic artery
In five patients, microcoils were deployed across the neck into the aneurysmal sac to embolize the lesions (‘packing technique’). A bare, self-expanding, nitinol stent (CordisTM, Johnson & Johnson, Miami Lakes, FL, USA) was placed in the splenic artery, in one SAA case with a wide aneurysm neck, to exclude coils placed within the aneurysmal cavity from encroaching and compromising the main artery (‘stent-assisted packing technique’) (Figure 2). In two other cases, before packing with microcoils, N-butyl-2-cyanoacrylate surgical glue (GlubranTM, GEM, Viareggio, Italy) mixed with ethiodized oil in a 1:3 ratio was embolized selectively and distally into the branches of the splenic artery supplying the aneurysm.

Stent-assisted packing technique. (a) Selective angiogram showing the aneurysm located in the distal splenic hilum with wide aneurysm neck. (b) A bare self-expanding nitinol stent was placed in the branch artery and the aneurysm cavity was packed with coils
In three patients, stent grafts (FluencyTM, Bard, Karlsruhe, Germany) were deployed to repair the aneurysms. In one SAPA case, the stent graft was placed in the splenic artery to exclude the aneurysm and spare the artery. In the remaining two SAA cases, the aneurysm sacs were located near the origin of the splenic artery (in one case, the splenic artery aberrantly originated from the superior mesenteric artery [SMA]) and there was not enough landing zone proximally for the stent graft or embolization (Figure 3). Therefore, stent grafts were deployed in the common hepatic artery and SMA, respectively, to exclude the orifice of the splenic artery successfully. Before stent graft implantation in these two cases, the splenic artery distal to the aneurysm was embolized with microcoils.
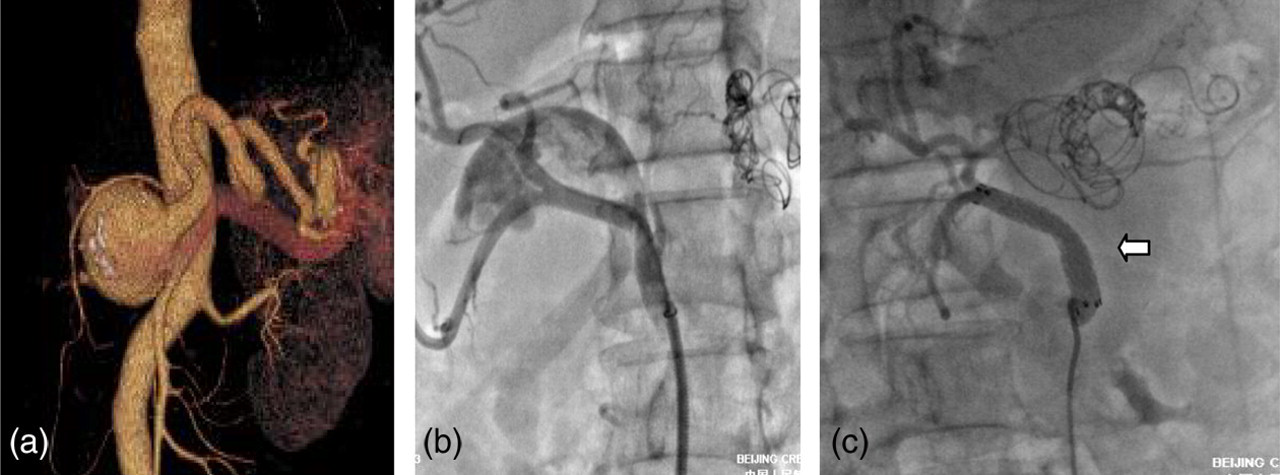
A 42-year-old woman with a history of portal hypertension and a diagnosis of ruptured splenic artery aneurysm. (a) Preoperational computed tomographic angiography showed an aneurysm arising from the root of the splenic artery. (b) After embolization of the distal splenic artery, the angiogram showed the common hepatic artery and the aneurysm. (c) A stent graft was deployed in the common hepatic artery (arrow), which excluded the aneurysm successfully
All procedures were performed by two experienced vascular surgeons. Preoperative antibiotic prophylaxis was not used routinely. The mean amount of contrast medium used was 165 mL per patient (range 100–230), and the mean total procedure time was 92 minutes (range 55–160).
Follow-up
Follow-up information was available for all patients. Clinical surveillance was complemented by a review of the medical records from the outpatient department. Postembolization syndrome was defined as fever, abdominal pain and slow bowel transit after splenic infarction. All patients underwent a follow-up CT scan within three months after the procedure, to evaluate the short-term results and complications. CT imaging was also available for 11 patients yearly; one patient was lost from follow-up 12 months later, with a mean follow-up of 32 months (range 9–51). CT images included unenhanced and enhanced images (arterial phase, parenchymatous phase) with multiplanar three-dimensional reconstruction.
Results
Endovascular treatment was successful at the first attempt in all 12 (100%) patients, with complete angiographic exclusion of the aneurysm at the end of the operation. The procedures ensured immediate control of bleeding and instant relief of pain in all three emergency patients with ruptured lesions. No major procedure-related complications and perioperative mortality were reported. After the procedure, four patients experienced mild abdominal pain and two experienced fever probably due to the splenic infarction. Thus, postembolization syndrome happened in 50% (6/12) of patients, yet none demonstrated significant hematological changes related to splenic insufficiency. Furthermore, all these patients recovered fully within a few days with symptomatic treatment. None required surgical repair, and no abscesses were detected by CT.
Postoperational CT scans showed multisegmental splenic microinfarcts in eight patients (66.7%, 8/12), including one lesion in the proximal segment of the splenic artery, two in the middle segment and five in the distal segment. Among these eight patients, six (two in the middle segment and four in the distal segment of the splenic artery) experienced postembolization syndrome. The other four patients who had no image defects were asymptomatic after the procedures. The initial splenic infarcts were unchanged in those patients in follow-up CT scans. Flow through the previously treated aneurysm sac was identified in only one patient three months after the ‘packing technique’ procedure; thus aneurysm exclusion was confirmed in 11 (92.7%) of 12 postoperative short-term studies. However, the flow disappeared on the six-month follow-up CT scans. No patient demonstrated gross evidence of aneurysm sac growth. In addition, no significant decrease in aneurysm sac size was noted on the postintervention follow-up.
Discussion
Aneurysmal lesions of the splenic artery are rare, yet account for about half of all cases of splanchnic artery aneurysms. 1,2 Predisposing conditions of SAAs include medial degeneration, fibromuscular dysplasia, pregnancy and portal hypertension, etc. 2 The common causes of SAPAs include mycotic infection of the arteries, trauma and pancreatitis. 1,2 The lesions are usually located in the intermediate segment or the distal segment of the splenic artery. 1–3 All these previously reported features were confirmed through our experience.
Although most SAAs and SAPAs are asymptomatic lesions that are discovered accidentally, their natural history usually involves expansion and eventual rupture. 4,5 Rupture should be suspected in those patients who experience acute pain in the left upper quadrant, a presentation seen in three of our patients. The diameter above which asymptomatic lesions should be treated is unclear, although 2 cm has been suggested. There has been no clear evidence of correlation between lesion size and rupture risk. 5–8 Treatment is also recommended in pregnant women, in women of childbearing age and in patients with symptomatic or expanding aneurysms. 7,9 Pseudoaneurysms of any size should be treated, since they have high rupture rates. 8
A CT angiography scan is crucial to confirm the diagnosis, evaluate lesion size and the morphology of the inflow and outflow artery before the operation. The CT findings determine whether or not angiography followed by endovascular treatment is required, and guide decisions regarding the therapeutic strategies, the diameter and length of stent grafts or coils. A radiological follow-up with a CT scan also helps detect early or delayed complications.
Therapeutic options available for patients with SAAs or SAPAs include conventional open surgery and endovascular treatment. 3,5,10,11 The mortality rate associated with the open procedure has been about 1.3% and the morbidity rate about 9%. 1,5,8,12 During the past decade, endovascular techniques including transcatheter embolization and stent graft placement were introduced as alternatives to conventional surgery. 5,8,13–15 These techniques can be used to treat most SAAs and SAPAs regardless of the etiology and location, especially when the site is difficult to access during conventional surgery or when the operative risk is high. Advantages over surgery also include the accurate localization of the aneurysm, the assessment of collateral flow and low risk for patients who are poor surgical candidates.
Three methods of endovascular therapy, including the sandwich technique, packing technique and stent graft placement, were applied in our series. The splenic artery was spared in half (6/12) of the patients. Preservation of the splenic artery is desirable, although not always essential. Collateral gastric, omental and pancreatic vessels usually supply enough blood to prevent splenic infarction. 8 The stent graft was supposed to be a good choice with regard to preserving the splenic artery while excluding the aneurysm. 14,16,17 But in most cases, this could be difficult owing to the tortuosity of the splenic artery, and it was impossible for the stent graft to reach the lesion. In our series, the stent graft was successfully used to exclude the aneurysm and spare the splenic artery in only one SAPA case. In two other cases, the aneurysms were located near the takeoff of the splenic artery, and there was not enough of the proximal landing zone. Hence, stent grafts were used to exclude the orifice of the splenic artery in these two patients.
In our series, multisegmental splenic parenchymal defects were noted in eight (66.7%, 8/12) patients at the postoperative CT scan. These infarcts were found in 33.3% (1/3) of aneurysmal lesions located at the proximal segment of the splenic artery, in 66.7% (2/3) of the middle segment and in 93.3% (5/6) of the distal segment. Therefore, it seemed that the likelihood of splenic infarction was higher towards the distal part of the splenic artery. This is probably due to the poorer collateral flow in the distal splenic artery. No patient sustained a delayed aneurysm rupture during long-term follow-up, and no patient demonstrated evidence of aneurysm sac growth. Conversely, aneurysm sac shrinkage was also not observed on postoperative surveillance.
Our study has various limitations. Inherent to its retrospective design, we are unable to draw conclusions regarding the treatment paradigms for SAAs and SAPAs or regarding optimal modes of ablation. A longer-term follow-up with larger patient cohorts and randomized trials are necessary to elucidate the ultimate role of endovascular therapy in the treatment of SAAs and SAPAs.
Conclusion
This series shows very low mortality and morbidity rates and confirms the potential advantages of endovascular repair, with regard to open surgery. The mid-term results of endovascular treatment of SAAs or SAPAs are excellent and deserve more experience.
Footnotes
Acknowledgments
Financial disclosure of authors and reviewers: none reported.