
Abstract
The great saphenous veins are gaining wide popularity as acceptable native vascular grafts, but in terms of flow capacity, their small caliber may be unsuitable for immediate replacement of arterial flow. Ten peripheral vascular or central venous reconstructions were performed using superficial femoral vein free grafts for re-establishment of immediate high-flow patency. Seven of the patients were men with a mean age of 61.5 ± 17.9 years (range, 21–81 years). The majority of the patients were of preoperative or intraoperative critically ill statuses in that they had extensive infection (n = 5), bleeding (n = 4), renal failure (n = 3) or hepatic failure (n = 1). The mean preoperative physiology score of the vascular POSSUM was 24.1 ± 8.8 (range, 15–37), and the mean operative severity score was 18.4 ± 4.9 (range, 10–26). All patients survived and recovered from systemic infection or critical hemodynamic instability. During the mean 28.9 months of follow-up, complications such as aneurysmal dilation, recurrent infection, graft stenosis/occlusion, lower limb edema and other clinical problems that required attention were not observed. In conclusion, we determined that deep veins can be applied as ideal graft conduits for reconstructing the major peripheral vessels under complicated conditions in select patients.
Introduction
Generally, the ideal graft is of the appropriate size and possesses minimal tissue toxicity. It must also be resistant to infection and exhibit long-term durability. The ‘homograft’ fits these requirements, but its availability is limited, particularly in developing countries. Since the 1950s, the great saphenous vein (GSV) has gained wide popularity as a well-rounded graft conduit. 1,2 In some cases, however, a larger diameter of the vein should be replaced to secure sufficient blood flow through the distal portion. Overall, no ideal graft perfectly matches all clinical demands.
The superficial femoral vein (SFV) as a graft conduit, originally introduced by Schulman and associates, 3 has not been chosen as a primary vascular graft due to a more invasive harvesting procedure, a surplus diameter compared with that of the GSV, and concern about the potential for venous morbidity after harvesting. Sometimes, however, its long length, large caliber and infection-resistant autogenecity are great assets to select patients who have systemic infection or require immediate postoperative high blood flow (IPHF) restoration. These particular characteristics have enabled the SFV to be considered an excellent graft conduit for aortic grafts or replacement of infected aortas. 4,5 However, data from clinical applications and efficacy of the SFV graft used for peripheral vascular or central venous substitutes from other than the neo-aortoiliac system (NAIS) are limited. The aim of this retrospective study is to identify the efficacy of SFV grafts for peripheral vascular or central venous reconstruction in critical patients.
Material and methods
From January 2005 to June 2009, seven men and three women with a mean age of 61.5 ± 17.9 years (range, 21–81 years) underwent a SFV grafting procedure at our hospitals. After approval from the Institutional Review Board and Ethics Committee, medical records and angiographic data were retrospectively reviewed, and a brief summary is presented in Table 1. Operative rationales for the use of a SFV graft were based on IPHF restoration and slowing the proliferation of the infectious (or contaminated) state (n = 7), expectation of long-term patency without anticoagulation (n = 2) and prevention of recurrent stenosis (n = 1). Six patients had undergone previous causative surgery associated with late reconstruction, but the other four had never had surgical procedures. Four surgeries (40%) (cases 2, 5, 6 and 10) were performed under emergent conditions, and another four were urgent surgeries (cases 1, 4, 8 and 9). The majority of the patients had preoperative or intraoperative critically ill statuses in that they had extensive infection with or without sepsis (cases 1, 2, 4, 8 and 9), bleeding (cases 5, 6, 7 and 10), renal failure (cases 1, 2 and 4) or hepatic failure (case 9). The mean preoperative physiology score of the vascular POSSUM was 24.1 ± 8.8 (range, 15–37), and the mean operative severity score was 18.4 ± 4.9 (range, 10–26). General anesthesia was administered to four patients (cases 1, 3, 5 and 8), and spinal anesthesia was administered to the others.
Summary of cases
SFV, superficial femoral vein; AVF, arteriovenous fistula; ECMO, extracorporeal membrane oxygenation; HD, hemodialysis; PS, physiologic score; OSS, operative severity score; IPHF, immediate postoperative high flow; SCV, subclavian vein; IJV, internal jugular vein; CFA, common femoral artery; CVA, cerebrovascular accident; ARF, acute renal failure; MVR, mitral valve replacement; TAP, tricuspid annuloplasty; SVC, superior vena cava; SCA, subclavian artery; Cx, complication; DVT, deep vein thrombosis; UGI, upper gastrointestinal; LC, liver cirrhosis
The general SFV harvesting technique has been described in detail elsewhere, 6,7 but we would like to add additional information to better explain the procedure. Besides preoperative duplex ultrasound evaluation and detailed history-taking regarding previous deep vein thrombosis (DVT) and any lower limb disease, an intraoperative venogram is necessary to assess the entire venous pathway of the leg, including the size, length and patency of the GSVs and SFVs. A postharvesting venogram can demonstrate comprehensive venous drainage pathway, shape and venous pressure after deep vein harvesting. First, a small incision approximately 4–5 cm long is made over the inguinal ligament, and then the integrity of all vascular anatomic structures of this area – the common femoral vein (CFV), profunda femoris, saphenofemoral junction and GSV tributary – should be verified under careful dissection and direct vision. After looping the SFV, further harvesting is performed guided by intraoperative ultrasonography (US). We believe that precise preoperative estimation of the required graft length and intraoperative US can prevent excessive lower limb dissection. With this method, in our series, up to 18 cm of SFVs were secured across the adductor hiatus without popliteal vein dissection, and this is why we did not use the term ‘superficial femoral-popliteal vein (SFPV),’ but ‘SFV.’
Taking care to avoid neurovascular and lymphatic injury is essential, and this is allowed by sharp dissection and clipping instead of electrocauterization. The SFV graft segment was left in position until the anastomosis took hold, and any manipulation that had the potential to irritate the graft was strictly prohibited. Another important procedure during graft preparation is ‘venous valve and weakened tortuous wall excision.’ Our group data from other types of bypass surgery using the GSV, as well as data from other studies, suggest that the remnant venous valves and varicosity in the graft raise the problem of turbulent graft flow and may have a negative influence on long-term patency. 8,9 To prevent postoperative venous hypertension or leg edema at the donor site, carefully preserving the integrity of both the profunda femoris vein with the CFV and the GSV with the CFV is essential. The mean SFV harvesting time was 43 ± 11.9 minutes (range, 25–60 minutes). During the in-hospital period, application of compression stockings was mandatory, but anticoagulation was not used. Therapeutic movement and early active ambulation was conducted under the direction of rehabilitation specialists. Brief reviews of typical cases follow.
Case 1
A 74-year-old man with a 25-year history of diabetic nephropathy and hemodialysis (HD) was admitted to the emergency center with loss of an arteriovenous fistula (AVF). Until that time, he had undergone seven AVF operations in both arms, and HD was being performed through his left upper arm, 6-mm artificial graft AVF. In the fistulogram, the graft on the left side was occluded by multiple acute thrombi, and the right upper arm native AVF flow also rapidly diminished and collateralized on the right subclavian area. Both subclavian veins were nearly totally occluded (Figure 1a). Catheter-directed thrombectomy/thrombolysis and balloon dilation were initially successful, but graft occlusion recurred the next day. Furthermore, during HD, the patient experienced a sudden cardiac arrest. Active cardiopulmonary resuscitation with a percutaneous cardiopulmonary bypass system was introduced, and a femoral catheter for HD was inserted. Five days later, the patient recovered and was transferred to the general ward. However, high fever and leukocytosis with lung infiltration persisted for the next four weeks, and a very large retroperitoneal hematoma was identified on follow-up computed tomography (CT). Blood cultures from the retroperitoneal hematoma, femoral dialysis catheter and peripheral vein confirmed methicillin-resistant Staphylococcus aureus (MRSA). Despite a high vascular POSSUM score of 37 points, life-saving surgery was performed under general anesthesia. After retroperitonal hematoma evacuation through a small right lower quadrant oblique incision, about 12 cm of the left SFV was harvested. Resection of the non-functioning and possibly infected left upper arm artificial AVF graft was then performed. To save and utilize the right AV fistula remnant, a right subclavian to left jugular vein bypass using the SFV graft was performed. Intraoperative US confirmed that a large amount of shunt flow in the right subclavian vein was running along the left internal jugular and innominate veins and draining into the superior vena cava (SVC) (angiographic findings; Figure 1b). Three days later, fever and leukocytosis resolved and HD was successfully performed through the right AVF. During the follow-up period of 12 months, neither leg edema nor lower leg venous hypertension was demonstrated.
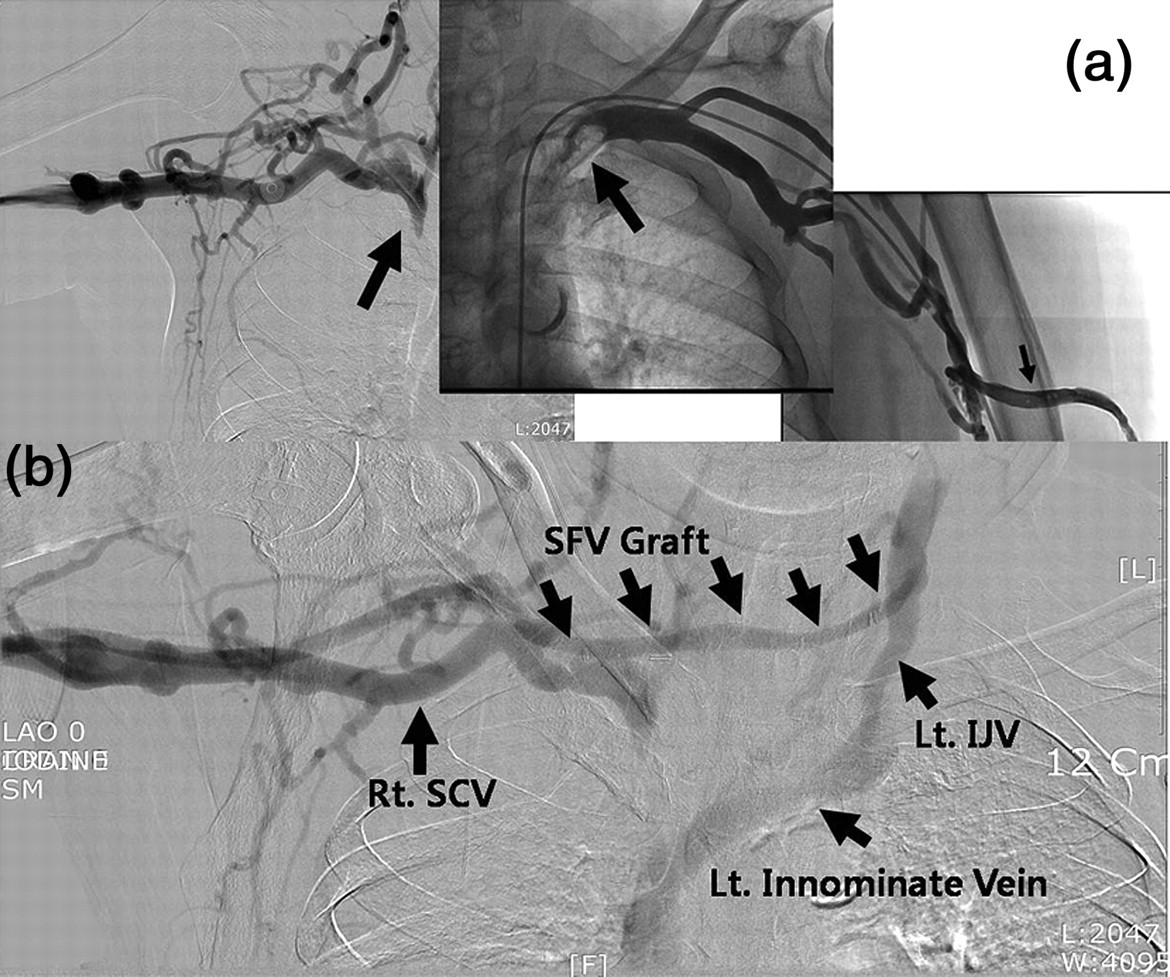
Case 1. (a) Angiographic findings demonstrated both SCV occlusion and near total stenosis (big arrows) and acute phase multiple thrombus in left arteriovenous fistula (small arrow). (b) Postoperatively, flow shunted from the right upper arm, entered the right SCV, passed through the SFV conduit and IJV, finally draining into the left innominate vein. Rt. SCV, right subclavian vein; Lt. IJV, left internal jugular vein; SFV, superficial femoral vein
Case 2
A 78-year-old man with a long history of diabetes and hypertension underwent transfemoral cerebral angiography. Three months later, he found an 8-cm pulsatile mass on his right femoral area; US revealed atherosclerotic femoral artery stenosis and previous catheter puncture site pseudoaneurysm. Aneurysmorrhaphy and patch angioplasty using bovine pericardium were performed, and the patient was uneventfully discharged three days postoperatively (Figure 2a). Careful follow-up was mandatory, but the patient refused to comply. One month later, he was re-admitted to the emergency department with high fever, hypotension and acute dehiscence of the femoral wound with pus and skin color change. Blood and wound cultures demonstrated MRSA. Surgery was performed under spinal anesthesia. Muscle necrosis and whitish yellow pus extended over the femoral area and up to the iliac lesion (Figure 2b). Infected thrombi filled the diseased iliac and femoral arteries, and no blood flow was detected (Figure 2c). After wide debridement of perivascular muscle tissue and resection of about 6 cm of the iliofemoral artery, the same length of the ipsilateral SFV was harvested and interposed on the resected iliofemoral artery segment (Figure 2d). After the surgery, he recovered from the sepsis and lower limb ischemia. An open wound dressing was applied for six weeks, after which time the patient was discharged.
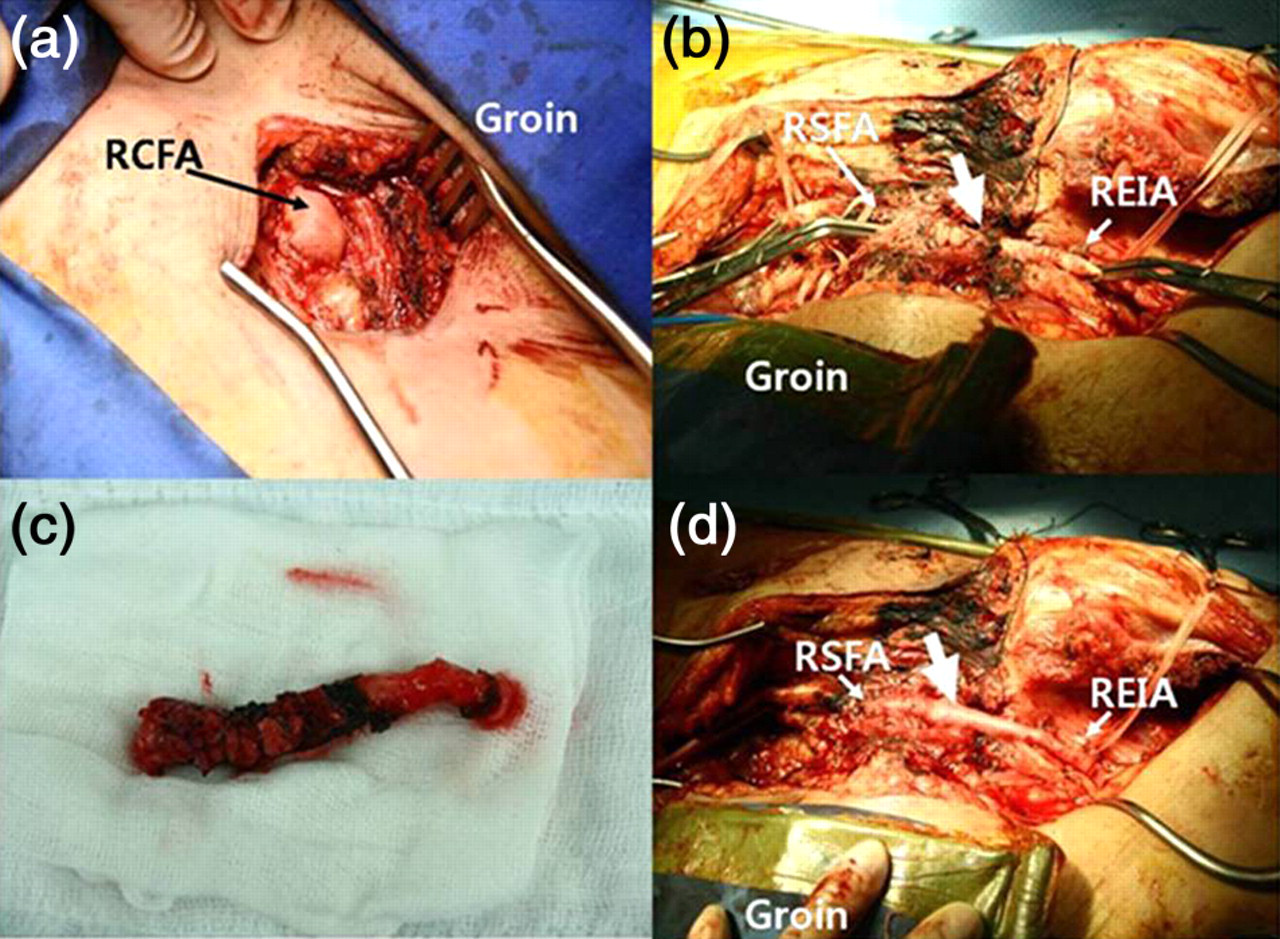
Case 2. (a) Photograph of right inguinal area during the first operation. Aneurysmorrhaphy and patch angioplasty using bovine pericardium was performed uneventfully. (b) The second operation. Blood and wound culture demonstrated methicillin-resistant Staphylococcus aureus (MRSA). Surgery was performed under spinal anesthesia. Muscle necrosis and whitish yellow pus was present on the femoral area and extended up to the iliac lesion. (c) Resected specimen revealed infected thrombi filling the diseased iliac-femoral artery; no blood flow occurred. (d) After wide debridement of perivascular muscle tissue and resection of about 6 cm of the iliofemoral artery, the ipsilateral SFV was harvested and interposed to the resected iliofemoral artery segment. RCFA, right common femoral artery; RSFA, right superficial femoral artery; REIA, right external iliac artery
Case 3
A 63-year-old woman underwent mechanical mitral valve replacement, tricuspid annuloplasty and a maze procedure due to infective endocarditis. 24F and 32F venous drainage lines were inserted for cardiopulmonary bypass. Securing a clear view of the mitral valve and associated structures during surgery was difficult due to a small left atrium and short SVC. Both the conventional left atrial approach and trans-septal incision were unsuccessful, and no choice remained but to cut the SVC. The SVC was then anastomosed using 6-0 prolene. However, the patient's face and upper arm became swollen after the surgery, and CT showed focal luminal narrowing and intraluminal thrombus formation. Redo exploration was performed five weeks postoperatively, which revealed that the SVC was pinched in at the midportion where the purse-string suture and end-to-end anastomosis for SVC repair had been performed. The narrowed lesion and thrombus were resected, and the SVC was reconstructed using 4 cm of the 8-mm polytetrafluoroethylene (Gore-Tex, W L Gore & Associates, Flagstaff, AZ, USA) graft. Despite redo surgery, however, the patient re-admitted for a SVC artificial graft thrombus that was detected on routine surveillance 12 months postoperatively. Upper body swelling was mild. However, due to the risks of pulmonary embolism and recurrent thrombus formation, re-redo sternotomy and artificial graft resection and SVC reconstruction were performed using 4 cm length of autologus SFV. In addition, due to a relative short graft harvesting of about 4 cm, a direct end-to-end anastomosis to repair the defective SFV was carried out. At 65 months postoperatively, neither restenosis nor thrombus formation was identified.
Case 4
This case was similar to case 2 in terms of clinical situation and surgical strategy. Please see Table 1 for a brief summary. At 12 months postoperatively, CT angiography demonstrated excellent vascular patency and no limb edema despite segmental absence of the left SFV (Figure 3).

Case 4. After the right common femoral artery interposition using the left superficial femoral vein, computed tomography angiography was performed 12 months postoperatively. Excellent vascular patency was demonstrated (a and c, arrows). No limb edema was present despite segmental absence of the left superficial femoral vein compared with the intact right side vein (b, arrows)
Case 5
A 21-year-old man who had been run over by a cultivator underwent emergency surgery on his right upper chest, shoulder and upper arm due to crushing injuries. He suffered a 20 × 8-cm skin defect and multiple fractures of the humerus, scapula and clavicle; in addition, his right subclavian artery and vein were torn to pieces. Especially considering the contaminated wound, his subclavian artery and vein were interposed using 4 cm and 3 cm length of SFV graft, respectively. No amputation was needed after vascular reconstruction.
Case 6
A 43-year-old woman injured her right knee while skiing. Acute bleeding occurred during arthroscopic surgery for a ruptured posterior cruciate ligament, immediately after the hole was drilled. About 4 cm of the popliteal artery was torn, and repairing this directly without tension was impossible. Due to the patient's young age and because this was a large vessel, 3 cm of the left SFV was used as a graft conduit, and popliteal artery interposition was performed. The patient was on no medications, including anticoagulation drugs.
Case 7
An 81-year-old woman with a long history of asthma and steroid medication was admitted to our hospital complaining of a two-month history of left pelvic and leg edema. Angiography verified May–Thurner syndrome. However, stent insertion into the left iliac vein was unsuccessful due to failed guidewire passage. Warfarin medication was begun. Instead of improvement, however, a massive, bleeding gastric ulcer developed one week later. Venous thrombectomy and a modified Palma operation using the contralateral SFV were performed under spinal anesthesia.
Results
In-hospital clinical outcomes
No in-hospital mortality occurred, and all SFV graft procedures resulted in their respective treatment goals. One patient (case 5) developed postoperative pneumonia, but had fully recovered by discharge. Two patients who developed preoperative acute renal failure also recovered during in-hospital treatment. All patients who developed preoperative sepsis (cases 1, 4 and 8) accomplished serological conversion within four days of surgery. Because we did not close the surgical wound at the end of surgery in cases with dirty infection or contamination on the surgical field, six patients (60%) required postoperative open wound dressings. Successful delayed primary wound closure was achieved in four patients. Two patients who had been in traffic accidents needed a skin graft (case 10) and pectoralis muscle rotation flap surgery (case 5), respectively. These factors resulted in extension of the treatment period, and thus the mean hospital stay time was 28.9 ± 12.5 days (range, 10–52 days).
Follow-up clinical outcomes
The mean follow-up duration was 28.9 ± 18.3 months (range, 10–65 months). Graft patency and patients' conditions were examined on a monthly basis by the outpatient department using physical examination and US. One patient died 13 months postoperatively due to aggravated hepatic failure. No patient showed or complained of harvested leg edema. One patient (case 7) developed edema distal to the left knee that was assumed to be post-DVT syndrome; however, the right lower leg where the SFV was harvested appeared normal. All SFV grafts maintained excellent graft flow, and no patients developed graft stenosis, aneurysmal dilation and ischemic symptoms.
Discussion
The authors applied SFV grafts to three categorized critical conditions in which patients required resistance to infection, IPHF restoration and long-term patency with or without anticoagulation. These were certainly our main goals and integral factors in the vascular surgeries. So far, the SFPV has been extensively used for NAIS reconstruction. 7,9–12 However, because initial main concerns surrounded the creation of the NAIS, the majority of studies were focused on SFPV, not on SFV. Therefore, unlike considerable data on SFPV grafts, SFV as a peripheral arterial or venous graft still has limited evidence, and more generally, is undervalued. We assume that this is mainly due to a ‘conceptual dogma’ regarding the SFV graft. Included in this dogma is that surgery using the SFV must be an extensive and dangerous operation. One expects that the creation of a NAIS requires not only an abdominal incision and dissection but also SFPV harvesting because it should cover, at minimum, the abdominal aorta and iliac artery. However, peripheral vascular reconstructions need a relatively shorter vascular conduit (SFV) and a smaller extent of peripheral dissection. This is neither ‘extensive’ nor ‘dangerous.’ In our series, despite rather high vascular POSSUM scores, zero mortality and little morbidity were observed; our data counter the ‘conceptual dogma.’ We believe that the benefits of SFVs originate from their natural characteristics (i.e. no tissue toxicity, infection resistance, long length and sufficient caliber) and that these merits can fully offset more invasive procedures, such as deep vein dissection.
The second misunderstanding is that this is a ‘time-consuming operation.’ However, a mean of 43 minutes of unilateral SFV harvesting time does not have a decisive negative effect on surgical outcomes. In addition to a skillful harvesting technique, the shorter dissection length of a SFV compared with a SFPV shortens the operation time because SFV harvesting does not require popliteal dissection across the adductor canal.
Note also that no patients suffered from postoperative lower leg edema or venous hypertension. Some studies have indicated that SFPV harvesting may impede venous outflow from the leg and induces relative venous hypertension in the harvested limb. 13,14 However, we suggest that postoperative limb edema can be minimized with meticulous surgical planning and appropriate strategies. According to Modrall et al.'s 14 observation, postoperative fasciotomy related to venous hypertension was performed in 20.7% of limbs after complete deep vein harvesting to a level below the adductor hiatus, but no fasciotomies were performed in patients undergoing subtotal deep vein harvesting ending above the adductor hiatus (P = 0.0023). Other studies found that routine preservation of the GSV during inguinal lymphadenectomy may reduce the incidence of wound cellulitis, wound breakdown and chronic lymphedema. 15 One other point claims our attention; postoperative limb edema cannot be fully explained by deep vein interruption alone, but appears instead to be associated with lympathic pathway blockade. 16–18 A Japanese group identified 8.9% limb edema and 17.8% leg swelling after unilateral GSV harvesting for coronary artery bypass surgery, and there were no statistical differences between normal and diseased legs in terms of maximum venous outflow, incidence of deep vein reflux and time constant. No significant differences were found between venous function and leg swelling. These findings were considerably associated with post-GSV resectional lymphatic obstruction. 19 Anatomically, in the leg, GSV branches are more numerous and communicate with many more accessory saphenous veins than in the thigh. Furthermore, near its termination, the GSV receives higher level veins, such as the superficial circumflex iliac, superficial epigastric and external pudendal veins. 20
Our technical strategy – precise preoperative estimation of the required graft length and use of intraoperative US, preservation of GSV and profunda femoris, and avoidance of popliteal dissection – is compatible with previous studies and prevents excessive lower limb dissection, resulting in maintenance of postoperative limb integrity.
Long-term patency and stability are also important characteristics of the ideal graft. Unfortunately, only a few studies have discussed patency of the SFV (or SFPV) graft in peripheral arterial or venous positions. 11,21,22 Also, our investigation is based on only 10 patients and contains a mean of 28.9 months of follow-up and thus further room exists for additional data power. However, the fact that no patients experienced lower limb ischemia or needed additional procedures enables us to expect favorable long-term results.
Conclusion
SFVs are excellent graft conduits for peripheral arterial and venous grafts in terms of feasible harvesting, resistance to infection, serving immediate high postoperative flow and long-term durability. Surgery using the SFV graft is neither time-consuming nor dangerous. A delicate preoperative and intraoperative surgical plan is mandatory, and future studies about long-term patency, appropriate clinical indication and safety issue of the SFV graft in peripheral vessel reconstruction are warranted.
Footnotes
Acknowledgments
Financial disclosure of authors and reviewers: none reported.