
Abstract
The aim of this study was to report the five-year incidence of incisional hernia after vascular repair of abdominal aortic occlusive (AOD) and aneurysmal disease (AAA), and to determine the factors associated with the development of this complication. Consecutive patients who underwent AAA and AOD at the University of Manitoba, Canada, between January 1999 and December 2002, were recruited and evaluated by clinical examination one week, one month and six months after the surgery, and through medical records review thereafter. The development of postoperative incisional hernia was recorded and analyzed. Two-hundred four patients, with a mean age of 70.1 years, provided consent for the study. The overall five-year incidence of incisional hernia was 69.1% and the overall median failure time was 48 months. The median failure time was 48 months for AOD and 36 months for AAA (P < 0.01). The urgent and ruptured AAA repair had a higher five-year incidence of incisional hernia as compared with AOD or elective AAA repair (P < 0.01). A history of bilateral inguinal hernia was significantly associated with incisional hernia (P < 0.05). Men and patients who were 65 years and older had a higher five-year incidence of incisional hernia (P < 0.01). Age ≥65 years, male gender, hypertension and past bilateral inguinal hernia repair double the risk for the development of incisional hernia (hazard ratio = 2.1. 2.2, 1.7 and 2.8, respectively). In conclusion, the five-year incidence of incisional hernia after vascular repair of AOD or AAA is 69.1%, and tends to occur late after vascular repair.
Introduction
Incisional hernia is one of the common complications after laparotomy, with incidence varying from 5 to 15%. 1 It is higher in postaortic reconstructive surgery, with a reported incidence of 21.1%. 2 The reported incidence of incisional hernia postabdominal aortic repair is 28.1%. However, there is considerable variability in the reported incidence of incisional hernia, ranging from 10 to 37% for abdominal aortic aneurysmal disease (AAA) and 3 to 17% for abdominal aortic occlusive disease (AOD). 3–7 The enhanced activity of metalloproteinases and a decrease in the ratio of collagen I/III in patients with AAA make them prone to hernia than those with AOD. 8,9 The follow-ups of the patients in previous studies are quite variable, from 12 to 48 months, and less than 50% of incisional hernias occur in the first year after surgery. Because of this, the true incidence of incisional hernia may be under-reported. This study was conducted to report the five-year incidence of incisional hernia after vascular repair of AOD and AAA, and to determine the factors associated with the development of this complication.
Methods
Consecutive patients who underwent AAA and AOD at the University of Manitoba, Canada, between January 1999 and December 2002, were recruited for the study. Consenting patients were divided into two groups: Group A included 156 patients who underwent open AAA repair and Group B included 48 patients who underwent AOD repair.
Demographic data were recorded, including: age, sex, history of ischemic heart disease, chronic obstructive pulmonary disease, hypertension (defined as systolic >160 mmHg or diastolic >95 mmHg), diabetes mellitus (patient on a diet, on oral hypoglycemic agents or on insulin), chronic renal failure, smoking (active, quitted or never smoked), abdominal wall hernia (unilateral inguinal, bilateral inguinal or umbilical inguinal), type of repair (tube, aorto-iliac, aorto-bifemoral or axillo-bifemoral) and type of fascial closure.
All patients provided consent using institutional review board-approved consent forms prior to their enrollment in the study and were operated on by the same group of surgeons through midline incision and transabdominal approach. The abdominal closure was performed with mass closure of the fascia with a loop using polydioxanone, which is a slow absorbable monofilament type of suture. All patients were examined at follow-up after one week, one month and then every six months for the presence of incisional hernia at midline incision. The development of incisional hernia after six months was ascertained through a medical records review for up to five years postoperatively. Incisional hernia was defined as any abdominal wall gap with or without a bulge in the area of the postoperative scar, perceptible or palpable by clinical examination or imaging (e.g. magnetic resonance imaging [MRI]). In this study, the diagnosis of incisional hernia was based on clinical examinations performed by the assigned operating surgeons during the patients' follow-ups at the outpatient clinics, as documented in the patients' medical records.
Univariate and bivariate analysis, namely Kaplan–Meier curves, and multivariate analysis employing Cox's proportional hazard modeling were used to determine the median time to failure (development of incisional hernia by 50% of the patients). Log-rank test was used to compare the predictor of five-year incisional hernia. Hazard ratio (HR) and its 95% confidence interval (CI) were calculated for each of the predictors of incisional hernia based on the multivariate models. Results were considered statistically significant when P value was <0.05.
Results
Two-hundred four patients, with a mean age of 70.1 ± 10.4 years, provided consent for the study. Seventy-four percent were men. The follow-up period was 3–60 months (median = 24 months). The demographic characteristics of our study population are shown in Tables 1 and 2. The AOD group was significantly younger than the AAA group (P < 0.0001). There were significantly more men who had AAA than women (P < 0.0001). More patients who had AOD were active smokers than patients who had AAA (P < 0.0001) (Table 1). AAA patients had significantly more urgent and ruptured surgeries than AOD patients (P = 0.035). Furthermore, AAA patients had significantly more of the tube and aorto-bi-inguinal bypass types of repair than the AOD group (who had more of the aorto-bi-femoral bypass type of repair) (P < 0.0001) (Table 2). There were no statistically significant differences for any of the clinical variables between the two groups (Table 1).
Patient demographics, risk factors and incidence of abdominal wall hernia (AOD versus AAA group)
AOD, aortic occlusive disease; AAA, abdominal aortic aneurysm; SD, standard deviation
Urgency of surgery, type of repair and abdominal closure (AOD versus AAA group)
AOD, aortic occlusive disease; AAA, abdominal aortic aneurysm; ABI, aorto-bi-inguinal at bypass; ABF, aorto-bi-femoral bypass; Ax-Bifem, axillo bi-femoral bypass; PDS, polydioxanone
The five-year cumulative incidence of incisional hernia for the two groups combined was 69.1% (Figure 1). The overall median failure time (50% development of incisional hernia) was 48 months (94% CI = 39.6 months) (Figure 2). The median failure time was 48 months (95% CI = 37.6 months) and 36 months (95% CI = 25.5 months) for occlusive and abdominal aortic aneurysm groups, respectively (P < 0.01) (Figure 3). There was no difference when the operative procedure was considered (P < 0.05). The urgent and ruptured AAA repair had, however, a higher five-year incidence of incisional hernia compared with occlusive or elective AAA repair (P < 0.001). In addition, a past history of bilateral inguinal hernia repair was associated with incisional hernia (P < 0.05). There was no correlation in the five-year incidence of incisional hernia with smoking history (P > 0.2), repair type (P > 0.1), closure type (P > 0.6) and development of postoperative wound infection (P > 0.7). Male gender (P < 0.005) and patients who were 65 years or older (P < 0.05) had a higher five-year incidence, respectively.
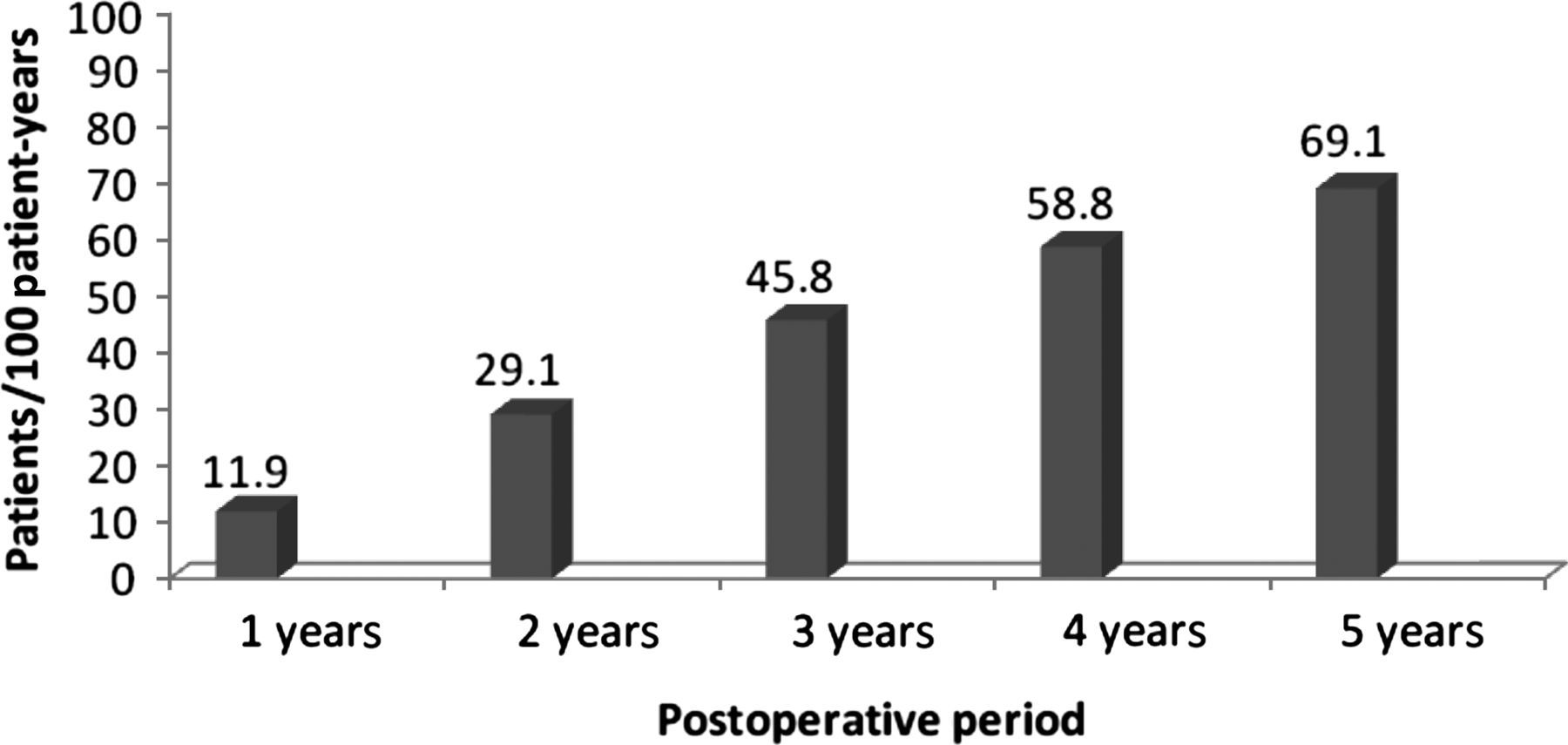
Cumulative annual incidence of incisional hernia postaortic repairs
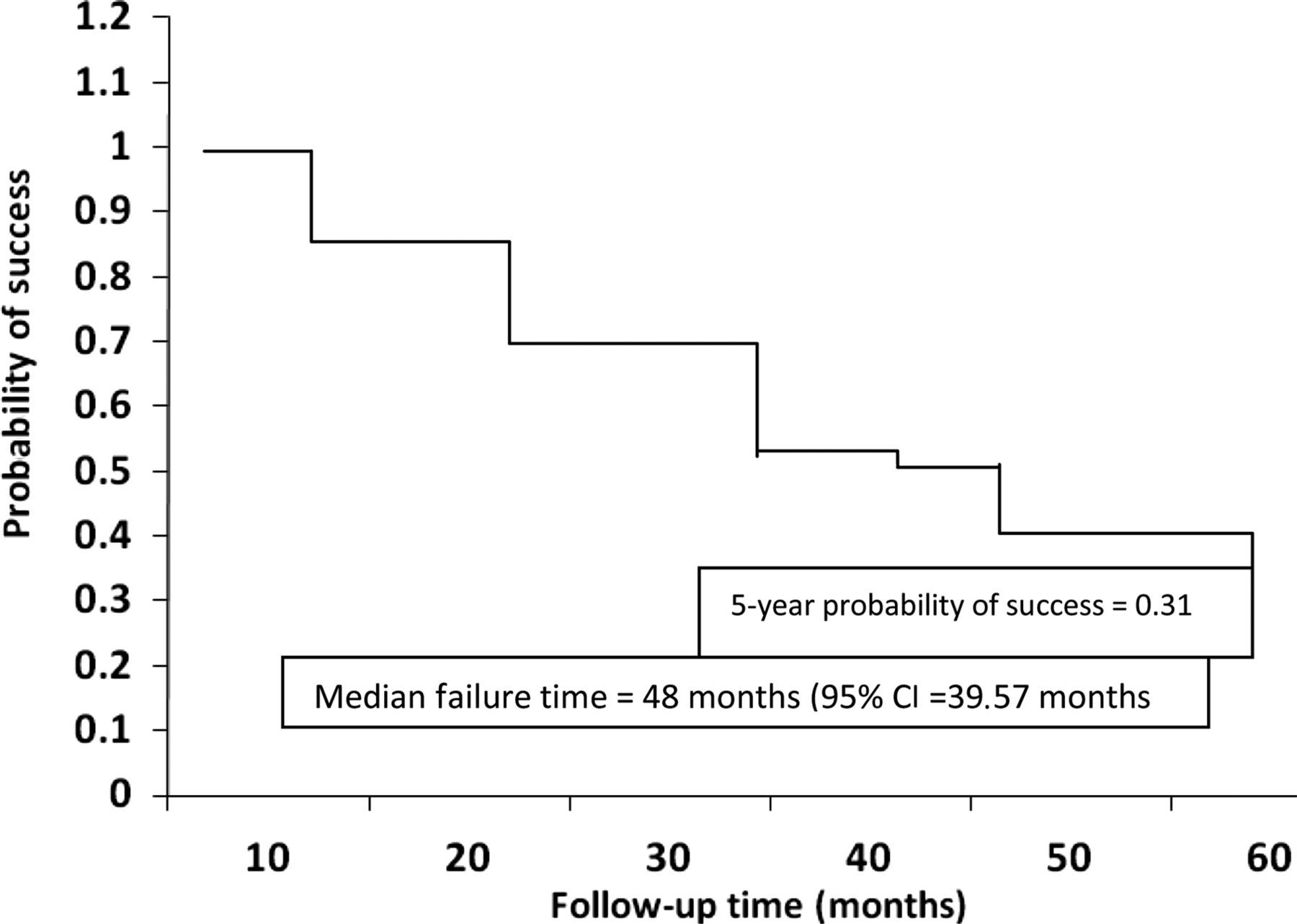
Kaplan–Meier curve representing five-year development of incisional hernia (failure) postaortic repair
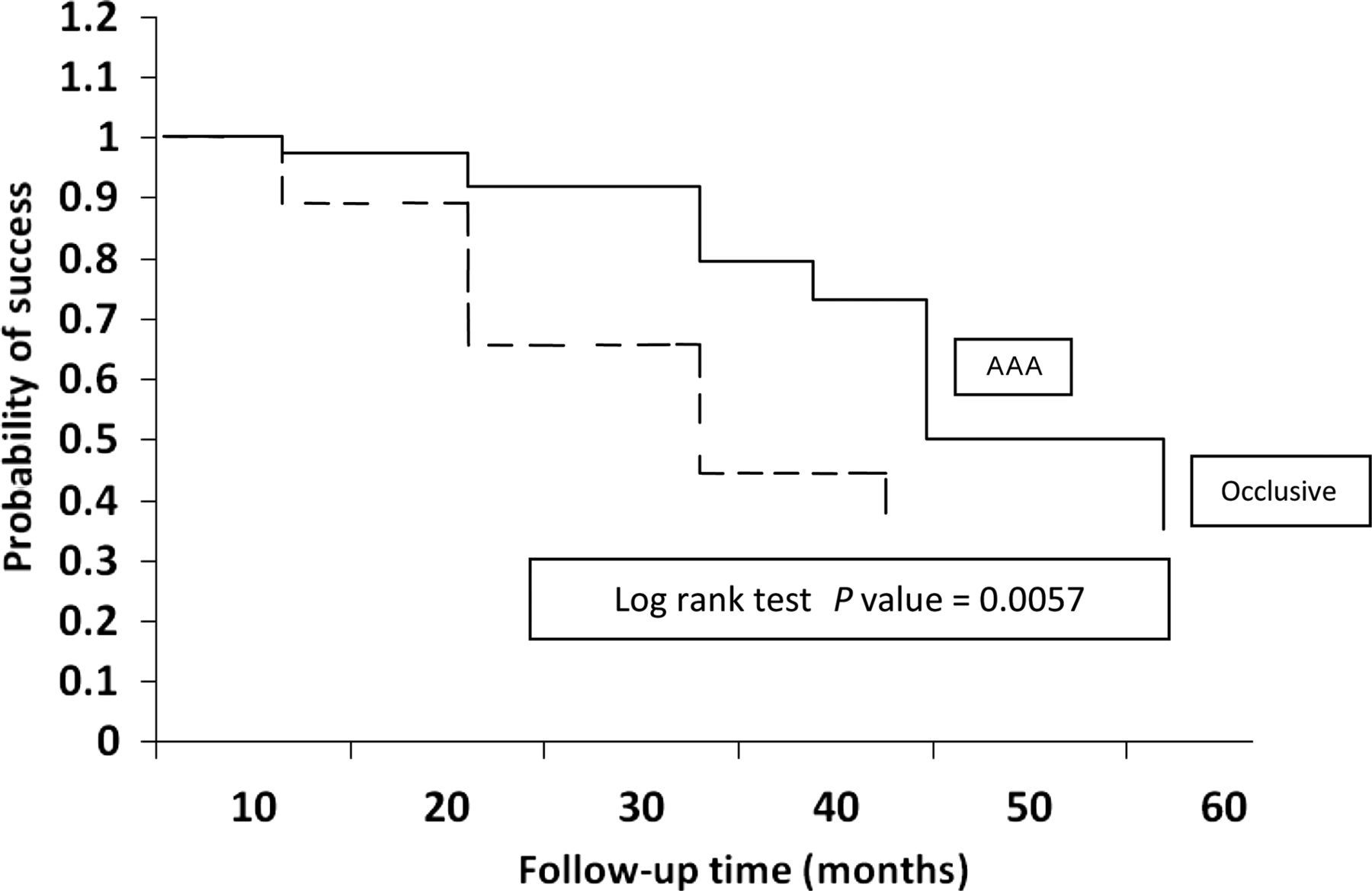
Kaplan–Meier curve representing five-year development of incisional hernia (failure) by type of aortic disease
The Cox's proportional hazard model identified male gender, hypertension and age more than 65 years as significantly associated factors in the incidence of incisional hernia (P = 0.0152, 0.0207 and 0.0234, respectively). Male gender more than doubled the risk for incisional hernia (HR = 2.2, 95% CI = 1.5–4.3), hypertension (HR = 1.7, 95% CI = 1.1–2.8) and age more than 65 years (HR = 2.1, CI = 1.1–4.1) (Table 3). However, the difference between AOD and AAA after controlling for potentially confounding variables such as age, gender, hypertension and a past bilateral inguinal hernia repair in the analysis, was statistically insignificant.
Cox's proportional hazard model predicting five-year incidence of incisional hernia
HR, hazard ratio; CI, confidence interval
Discussion
The incidence of incisional hernia after midline incision postaortic reconstructive surgery is a common long-term complication, with a variably reported incidence in the literature of 7 to 28%. 6,7 Although this incidence seems high, especially if it is compared with the incidence of incisional hernia postlaparotomy for other pathology (1–15%), we think that the incidence is higher than that. It is more common after AAA than AOD, with a reported incidence in a recent systemic review study of 21.0 and 9.8% at follow-up periods of 27.2 and 29.3 months for AAA and AOD, respectively. 10
In this study, we report an incidence of incisional hernia of 29.1% at 24 months of follow-up and a five-year incidence of 69.1%. This is higher than what has been reported in the literature. 6–11 The follow-up period, as well as diagnostic methods for incisional hernia, can affect the incidence of incisional hernia and explain the variability of reported results. Most of the studies reporting incidences of incisional hernia postaortic reconstructive surgery had less than a five-year follow-up. The majority of significant incisional hernia develop in the first two years following surgery, 12 with an increase in incidence of up to 35% 5–10 years following surgery. 11 This can explain the low incidences of incisional hernia in previously published reports. Furthermore, the diagnosis of incisional hernia was mostly based on clinical examinations in most of the reported literature, which is subjective and surgeon-dependent. 3,4,6,13,14 Diagnostic imaging, especially MRI, can be helpful in the diagnosis of incisional hernia. In fact, a high incidence of incisional hernia can be diagnosed – up to 31.4% for AAA and 17.5% for AOD – just by using clinical examinations and MRI. 15
Reports have suggested that up to 40% of these hernias would require operative repair because of persistent abdominal pain or incarceration. 16 Given the high incidence of incisional hernia and its long-term morbidity, surgeons need to look for an effective and safe option to reduce the incidence of incisional hernia. We think that prophylactic use of mesh is a potentially effective way to reduce the incidence of incisional hernia, especially in high-risk patients. 17 Use of a prophylactic mesh is a safe and effective method to decrease the incidence of incisional hernia after AAA repair. 18
Furthermore, in this study, a past history of bilateral inguinal hernia was associated with incisional hernia (P < 0.05). It nearly tripled the risk of development of incisional hernia (HR = 2.8). Literature has suggested that the systemic proteolytic effect and the increased turnover of type III collagen might be important in the development and association of aortic aneurysm and abdominal wall hernia formation. 19–21 Of the other recognized factors for increased risk of incisional hernia, age greater than 65, male gender and hypertension were found to increase the risk of development of incisional hernia by at least two-fold.
Declarations