
Abstract
The objective of the study was to provide an overview of the most common treatments for intermittent claudication and to determine the effectiveness in improving walking distance and quality of life based on a combination of direct and indirect evidence. We included trials that compared: angioplasty, surgery, exercise therapy or no treatment for intermittent claudication. Outcome measurements were walking distance (maximum, pain-free) and quality of life (physical, mental). We used a network meta-analysis model for the combination of direct and indirect evidence. We included 42 studies, presenting 3106 participants. The network meta-analysis showed that supervised exercise therapy (Δ = 1.62, P < 0.01), angioplasty (Δ = 1.89, P < 0.01) and surgery (Δ = 2.72, P = 0.02) increased walking distance significantly more than no treatment. Furthermore, supervised exercise therapy (Δ = 0.60, P < 0.01), angioplasty (Δ = 0.91, P = 0.01) and surgery (Δ = 1.07, P < 0.01) increased physical quality of life more than no treatment. However, in the sensitivity analysis, only supervised exercise therapy had additional value over no symptomatic treatment (Δ = 0.66, P < 0.01). In conclusion, this network meta-analysis indicates that supervised exercise therapy is more effective in both increasing walking distance and physical quality of life, compared with no treatment. Angioplasty and surgery also increase walking distance, compared with no treatment, but results for physical quality of life are less convincing.
Introduction
Intermittent claudication is a symptom of peripheral arterial disease and is described as an uncomfortable or painful feeling in the calves, buttocks or thighs that is experienced while walking and that is relieved by a short rest. 1 Survival of patients with intermittent claudication is decreased, mainly due to cardiac and cerebrovascular co-morbidity; 2 however, the prognosis of the leg is favorable. 3,4 In the vast majority of cases, intermittent claudication is not a limb-threatening condition. Nevertheless, it has a considerable negative influence on the patient's functional capacity, ambulatory activity and quality of life. 5–7 Therefore, treatment of intermittent claudication aims for functional improvement and increase in quality of life rather than limb-salvage.
Exercise therapy is the oldest suggested therapy for intermittent claudication. 8 More recently, surgical 9 and endovascular interventions 10 were described. Traditionally, studies evaluating invasive interventions for intermittent claudication mainly focused on results of increased blood flow rather than functional improvement and changes in quality of life. However, objective indices of peripheral arterial disease (e.g. ankle–brachial index, angiographic extent of the disease) only correlate weakly with functional capacity and quality of life. 11 More importantly, correlations between hemodynamic improvements and improvements in functional capacity, quality of life and symptoms are only modest. 12–14 This indicates that outcome measurements other than hemodynamics would be more valuable to describe the results of treatment for intermittent claudication. Furthermore, as was recently described by Cao and De Rango, 15 the discussion about the best treatment of intermittent claudication is ongoing and lack of evidence of more recent developed techniques was underlined.
The objective of this meta-analysis is to provide an overview of evidence of the most frequently used treatments for intermittent claudication and to determine their effectiveness in improving walking distance and quality of life.
Materials and methods
Selection criteria
All clinical trials that compared at least two of the following treatments for intermittent claudication: angioplasty, surgery, exercise therapy or no treatment were potentially eligible for inclusion in the meta-analysis. Additional inclusion criteria were presence of intermittent claudication (Fontaine stage 2/Rutherford stages 1–3), walking distance (assessed on a treadmill) and/or quality of life as an outcome measurement.
Exclusion criteria were a follow-up duration of less than three months and stages of peripheral arterial disease other than intermittent claudication. Furthermore, studies in languages other than English, German or Dutch were excluded.
Search strategy
We conducted a search in Pubmed and Embase until February 2009 with the following search terms: peripheral arterial disease, intermittent claudication, peripheral arterial obstructive disease, peripheral vascular disease, peripheral arterial occlusive disease, PAD and PAOD; angioplasty, exercise, walking, endarterectomy and bypass; and quality of life, QOL, short form 36, SF-36, Rand 36, euroqol, sickness impact profile, SIP, vascuqol and walking distance. The reference lists of relevant articles were hand-searched for additional studies.
One author (LMK) selected potentially eligible trials based on the abstracts. These studies were then independently assessed for suitability by two additional authors (LMK, JAWT). If necessary, a third reviewer (MHP) was asked for conclusive advice.
Interventions
Interventions were categorized into no treatment, non-supervised exercise therapy (non-SET), supervised exercise therapy (SET), angioplasty, surgery, conservative treatment or invasive treatment by two reviewers (LMK, MHP).
No treatment was defined as no treatment or the use of placebo tablets with or without treatment of vascular risk factors and without any advice to exercise. Non-SET was defined as a single or repeated advice and/or information on exercise. Supervision of exercise was considered to be present if a nurse or physiotherapist was present during the training sessions. Within the definition of angioplasty, both angioplasty alone and angioplasty with (primary or selective) stent placement or laser-assisted angioplasty were accepted. The surgical category consisted of bypass surgery as well as endarterectomy.
Conservative and invasive treatments are categories with mixed treatment modalities. Studies for which it was not clear as to what the exact treatment was or no differentiation was made between the various invasive or conservative treatments were categorized in a mixed category (e.g. angioplasty and surgery).
Outcome measurements
The primary outcome measurement was the absolute claudication distance (maximum walking distance) as measured by a treadmill test. A progressive treadmill test (constant speed, increasing slope) was preferred, but if not available a continuous treadmill test (constant speed and slope) was an alternative.
Secondary outcome measurements were the initial claudication distance (pain-free walking distance) and quality of life. The preferred quality-of-life assessment was the medical outcomes study 36-item short-form health survey (SF-36), but other quality-of-life instruments were also eligible. The SF-36 was summarized into a physical health component and a mental health component. 16 Alternative quality-of-life questionnaires were also summarized into physical and mental health components.
Assessment of quality of the reports
One reviewer assessed (LMK) and a second confirmed (SPN) the quality of each trial according to the criteria of Jadad et al. 17 Double blinding was not considered, because in trials comparing conservative and invasive treatments blinding is not possible. We gave each trial a summary score ranging from 0 to 3.
Data extraction and calculation
If available, from each treatment arm of each study, we extracted the number of patients, baseline standard deviation, baseline mean and follow-up mean for walking distance (absolute and initial claudication distance) and quality of life (mental and physical health). Data of the last assessment in the study were used for the analyses. If these data were not available authors were contacted. If authors did not respond to our request or did not have the requested data available, the data were, if possible, calculated based on other information presented in the articles using various methods. 18 A description of the calculations and methods used can be found in Appendix 1.
Statistical analysis
For all outcome measurements, the standardized mean change between the baseline and follow-up assessment for each treatment arm in the individual studies was calculated (i.e. mean at follow-up minus baseline mean, divided by the baseline standard deviation).
Direct evidence means a direct comparison of different treatments in a (randomized) controlled trial. Indirect evidence means that there is no trial that directly compares the different treatments. However, if two trials compare, for example, treatment B with, respectively, treatment A and C, something can be said about the effectiveness of A versus C. For example, if treatment A is more effective than treatment B and treatment B is more effective than treatment C, a logical conclusion is that treatment A is more effective than treatment C although no direct comparison is made.
The direct evidence about the relative effectiveness of one intervention compared with another was then expressed in terms of the difference between the standardized mean change values. These effect sizes were then meta-analyzed based on a random-effects model using restricted maximum-likelihood estimation when at least three effect size estimates were available (with only two estimates, a fixed-effects model was used).
For the combination of the direct and indirect evidence, we used an arm-based network meta-analysis model 19 for each outcome measure (the network of evidence for the mental health component of quality of life yielded two disconnected sets of interventions, which were examined separately). A single parameter for the random effects variance and a constant correlation of 0.5 between the random effects within a study was assumed, so that the amount of heterogeneity between all pair-wise intervention contrasts was constrained to be equal. 20 The models were fitted with restricted maximum-likelihood estimation. Based on the fitted models, a relative intervention effectiveness can then be obtained for any two interventions connected with each other via the network of evidence, even if no direct evidence is available to compare those two treatments. For the network meta-analysis, we also conducted sensitivity analyses, leaving out all studies with Jadad scores below 2 (all non-randomized trials).
Results
One hundred forty-three potential eligible articles were identified up to September 2008. We had to exclude 96 articles for the following reasons: no intermittent claudication (n = 9); cohort study evaluating just one treatment (n = 29); other treatments described than those included in the meta-analysis (n = 10); no treatment specified (n = 15); outcome measurement other than walking distance or quality of life (n = 13); duplicate publications (n = 10); follow-up less than three months (n = 7); and other reasons (n = 3), leaving 42 studies reported in 47 articles for inclusion in the meta-analysis. References of the excluded articles are listed in Appendix 2.
Description of the studies
The main characteristics of the included studies are presented in Table 1. Thirty-six articles reported results of randomized controlled trials, four articles concerned controlled trials and seven studies were cohort studies, presenting the results of a total of 3106 participants (no treatment 504, non-SET 531, SET 982, angioplasty 333, surgery 198, conservative 341 and invasive 217).
Characteristics of the included studies
Non-SET, non-supervised exercise therapy; SET, supervised exercise therapy; RCT, randomized controlled trial; CT, controlled trial; NA, not available; SF, short form; ACD, absolute claudication distance; ICD, initial claudication distance; SIP, sickness impact profile
Absolute claudication distance
Data for the absolute claudication distance at the end of the study were available for 35 studies. 8,9,21–53 The majority of the included trials compared SET with either non-SET (n = 14) or no treatment (n = 15).
Figure 1a presents the results using only direct evidence. The most obvious result is that SET is on average better in increasing the absolute claudication distance than both non-SET (P < 0.01) and no treatment (P < 0.01) based on 14 and 15 studies, respectively. The combined direct and indirect evidence is presented in Figure 2a – results for SET are robust. Furthermore, the combined analysis suggests that angioplasty and surgery increase absolute claudication distance more than non-SET and no treatment, although the comparison of surgery with non-SET just failed to reach statistical significance (P = 0.06).
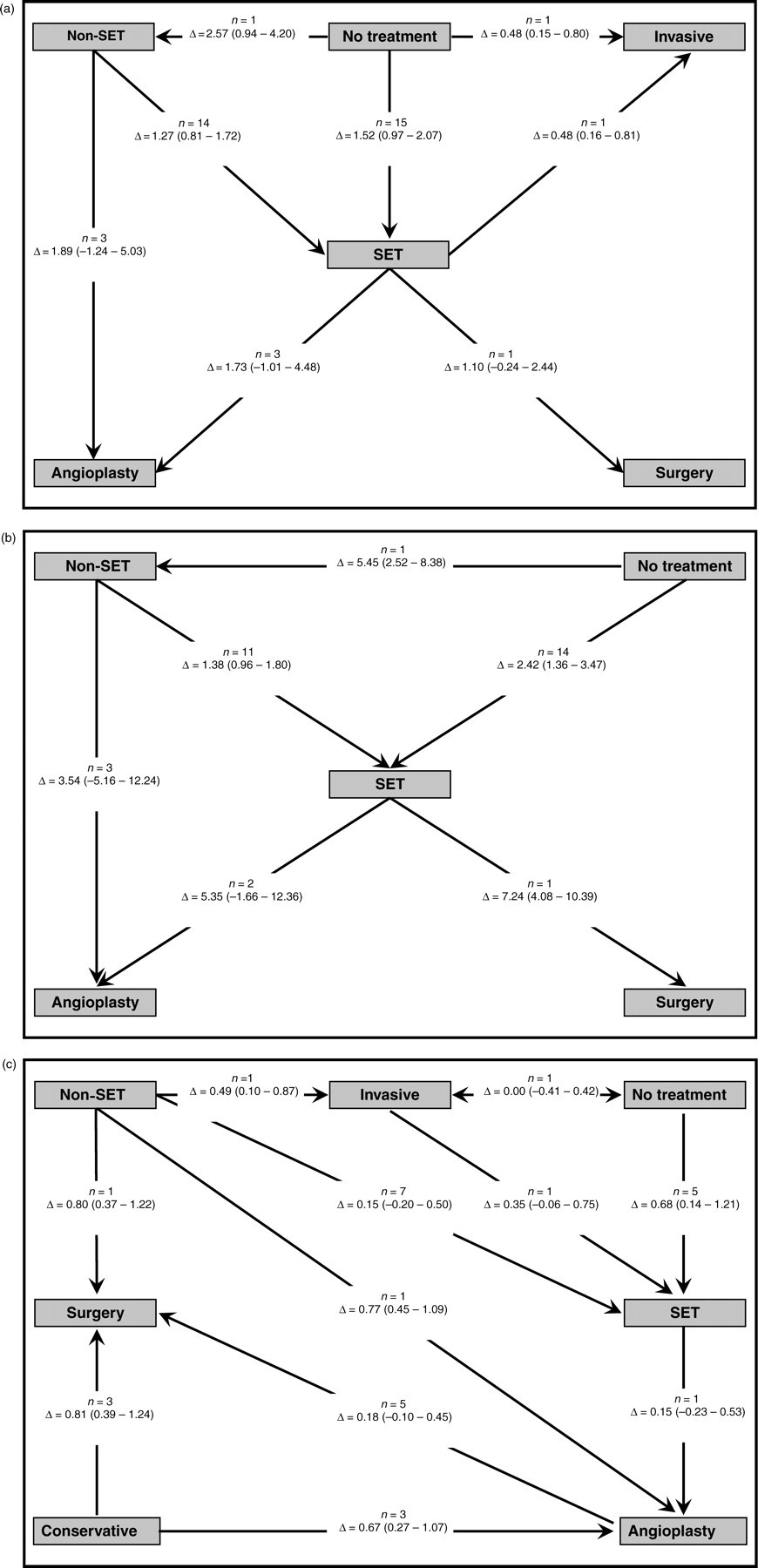
Results of the direct comparisons. In this figure only direct evidence is gathered for all outcome measurements. In the gray blocks, the different treatments are indicated. In the white blocks, the number of studies (n), the difference in standardized change (Δ) with a 95% confidence interval, and the P value are noted. The arrows indicate the direction of the effect and the head of the arrow points to the more effective treatment. (a), (b) and (c) describe the results of the absolute claudication distance, initial claudication distance and physical health. Non-SET, non-supervised exercise therapy; SET, supervised exercise therapy

Results of the network meta-analysis. In this figure, both direct and indirect evidence is combined for all outcome measurements. In the right blocks, forests plots are shown that compare the treatments with no symptomatic treatment as reference. Results are indicated as difference in standardized change (Δ) with a 95% confidence interval. In the left blocks, the other treatments are compared with each other. Results are indicated as the difference in standardized change (Δ) with the P value. A positive Δ indicates that the treatment modality in the column (bold) is superior to the treatment modality in the row (cursive). A negative Δ indicates the opposite. (a), (b) and (c) describe the results of the absolute claudication distance, initial claudication distance and physical health, respectively. Non-SET, non-supervised exercise therapy; SET, supervised exercise therapy
In the sensitivity analysis, 14 studies were excluded. Six of the excluded studies compared non-SET with SET and eight studies compared no treatment with SET. Combining direct and indirect evidence, the results for all comparisons remained. Results of the sensitivity analysis are presented in Table 2.
Results of the sensitivity analyses*
SET, supervised exercise therapy; non-SET, non-supervised exercise therapy
*Data are presented as difference in standardized change (δ) and 95% confidence interval. All data shown use no symptomatic treatment as referent treatment
Initial claudication distance
Data from 30 studies, reporting 32 comparisons on the initial claudication distance, were available (Figure 1b). 8,9,22–26,28–31,33–37,39–42,44,45,47–54 Most trials compared SET with non-SET (n = 11) or SET with no treatment (n = 14).
The most obvious result is that SET increases initial claudication distance more than both no treatment and non-SET. The results based on only the direct comparisons for initial claudication distance are depicted in Figure 1b.
Combining both direct and indirect evidence, SET, angioplasty and surgery are more effective when compared with no treatment in increasing initial claudication distance. Additionally, surgery performs better than non-SET, SET and angioplasty.
In the sensitivity analyses (Table 2), 14 studies were excluded. Six of the excluded studies compared non-SET with SET and eight studies compared no treatment with SET. Combining direct and indirect evidence, SET, angioplasty and surgery remain better in improving initial claudication distance compared with no treatment. Surgery is still more effective than non-SET, SET and angioplasty, although the comparison with angioplasty just failed to reach statistical significance (P = 0.06).
Physical health
Data from 19 studies reported 29 direct comparisons for physical health (Figure 1c). 21,37,39,45,47–49,52,55–65 Using only direct evidence, SET increases physical health more than no treatment (P = 0.01). Other direct results for physical health are presented in Figure 1c.
Combining direct and indirect evidence, SET, angioplasty and surgery are more effective in improving physical health when compared with no treatment. Furthermore, angioplasty and surgery are more effective than both non-SET and conservative treatment. The results of the combined direct and indirect evidence are presented in Figure 2c.
For the sensitivity analysis, eight studies were excluded, leaving 11 studies describing 12 direct comparisons. SET was compared with no treatment (n = 5), non-SET (n = 4), angioplasty (n = 1) and invasive treatment (n = 1). Furthermore, invasive treatment was compared with no treatment. In the sensitivity analysis, the results of SET compared with no treatment remain in favor of SET with a difference in standardized change of 0.66 (95% CI 0.20–1.13). All other treatments are not significantly different from each other, or comparisons are excluded from the analysis as part of the sensitivity analysis.
Mental health
Data from 14 studies reported 20 direct comparisons for mental health. 37,39,45,47,48,52,55–57,60,62–65 None of the included treatments differed significantly from each other in the direct, indirect and sensitivity analysis (data not shown).
Discussion
This network meta-analysis shows that SET, angioplasty and surgery are more beneficial in increasing pain-free and maximum walking distance as compared with no treatment. For physical health, SET has an additional benefit compared with no treatment. For angioplasty and surgery, improvements in physical health compared with no treatment are seen in the combined analysis. However, in the sensitivity analysis this was not a robust result. None of the studied treatments had any effect on mental health.
Moreover, no obvious differences in effectiveness were found when comparing SET, angioplasty and surgery with each other. Only for increasing pain-free walking distance, surgery seems more effective than SET.
Watson et al. 66 compared exercise therapy with other treatments and concluded that compared with no treatment, exercise therapy significantly improved maximum walking distance. Evidence for exercise compared with other treatments was limited.
A meta-analysis of Fowkes and Gillespie 67 compared angioplasty with non-surgical management. Two studies are included in this meta-analysis and with the non-SET-based study results, angioplasty was significantly better than non-surgical management. However, as in our meta-analysis, with the SET-based study results, no significant difference was found between angioplasty and non-surgical management. Spronk et al. 14 compared exercise therapy with angioplasty and found that both treatments brought about improvements in physical health-related quality of life. However, no differences between exercise and angioplasty were found.
One meta-analysis compared bypass surgery with other treatments for patients with chronic lower-limb ischemia. 68 The authors concluded that there was limited evidence for a superior effectiveness of bypass surgery compared with other treatments and that further large trials are required.
The results from the literature mentioned above are in line with the results of our current network meta-analysis.
A striking finding of this meta-analysis is the discrepancy between the number of trials studying the effect of exercise therapy (n = 43) compared with the number that studied the effect of angioplasty/surgery (n = 14). This imbalance had implications for the sensitivity analyses as almost no studies remained in the analyses to compare angioplasty and surgery with other treatments. Therefore, further research is needed to assess the functional and quality-of-life outcomes of especially angioplasty and surgery.
Limitations
To establish the effectiveness of an intervention, direct evidence from randomized controlled trials should be used whenever possible. However, due to the limited number of high-quality direct comparisons, indirect evidence was added to the current meta-analysis, bringing uncertainty to our results.
Another potential limitation is the inclusion of several non-randomized and cohort studies in the meta-analysis. Lack of randomization may result in biased effect size estimates, especially when patient characteristics play a role in selecting the treatment. To address this problem, we performed sensitivity analyses that excluded all non-randomized trials.
Finally, we used end-of-study data as the primary outcome instead of a fixed follow-up time for each study. The reason was that many studies differed in follow-up and that the number of studies was not sufficient to do the analyses for the different follow-up periods separately. Clearly, follow-up time could have an influence on the results of the different interventions (e.g. the time until maximum treatment effect for angioplasty is different than for SET). We examined this issue by including follow-up time as a potential moderator in the meta-analyses of the direct comparisons. However, no moderating effects of follow-up time were found.
According to the current meta-analysis, three treatment options for increasing walking distance in patients with intermittent claudication are effective, namely SET, angioplasty and surgery. However, not only the effectiveness of a treatment, but also the complication risks should be taken into consideration when making a treatment plan for an individual patient. SET is an effective, as well as safe, option to treat patients with intermittent claudication given that it is a non-invasive treatment. On the other hand, both angioplasty and bypass surgery are invasive treatment options with known morbidity and mortality. Taking the results from this meta-analysis plus the known complication risks from invasive treatment into account, the clinical implication should be that patients with intermittent claudication should first be treated with supervised exercise therapy. Accordingly, efforts should be made to make supervised exercise programs universally available for patients with intermittent claudication.
In conclusion, supervised exercise therapy is more effective in both increasing walking distance and physical health when compared with no treatment in patients with intermittent claudication. Angioplasty and surgery also increase walking distance, compared with no treatment, but results for physical quality of life are based on mostly non-randomized trials.
Large randomized controlled trials comparing supervised exercise therapy, angioplasty and bypass surgery in terms of walking distance and quality of life are necessary to establish the potential extra benefits of angioplasty and bypass surgery in the treatment of intermittent claudication.