
Abstract
Substantial lower-limb edema affects the majority of patients who undergo peripheral bypass surgery. Edema has impairing effects on the microvascular and the macrovascular circulation, causes discomfort and might delay the rehabilitation process of the patient. However, the pathophysiology of this edema is not well understood. The Cochrane Library and Medline were used to retrieve literature on edema following peripheral bypass surgery. Factors other than local wound healing alone are suggested in the literature to play a role, given the severity and duration of this edema. Hyperemia, microvascular permeability, reperfusion-associated inflammation and lymphatic disruptions are likely to facilitate the development of edema. Preventive methods could be lymphatic-sparing surgery, intraoperative antioxidative therapy and postoperative elevation. Successful treatment strategies to reduce postoperative edema are based on lymph massage and external compression. In conclusion, the pathophysiology of edema following peripheral surgery is not fully understood, although reperfusion-associated inflammation and lymphatic disruptions are likely to play a crucial role. When future less-invasive techniques prove to be successful, postoperative edema might be minimized. Until then, a careful lymphatic-sparing dissection should be executed when performing a peripheral bypass reconstruction. Postoperatively, the use of compression stockings and leg elevation are currently the golden standards.
Introduction
Endovascular techniques have been positioned prominently in the vascular practice over the last decade. However, some patients will still be subjected to peripheral bypass surgery when they do not qualify for endovascular treatment strategies. A peripheral bypass reconstruction should be reserved for patients suffering severe intermittent claudication, rest pain or loss of tissue (Fontaine stage II, III and IV/Rutherford category 3, 4, 5 and 6). 1 The occurrence of substantial postoperative lower-limb edema after peripheral bypass reconstructions is a recognized phenomenon. Lower-limb edema causes discomfort to the patient and may delay rehabilitation following an otherwise successful revascularization, resulting in a prolonged in-hospital stay or out-of-hospital care. Edema has an inhibiting effect on wound healing as it impairs the macrovascular and micro-vascular circulation. This review was performed to clarify the current insights in pathophysiological mechanisms that lead to edema following peripheral bypass surgery and to analyze the effects of known treatment methods to prevent and reduce this edema.
Methods
Overview of RCTs of treatment options to prevent and/or reduce post-revascularization edema
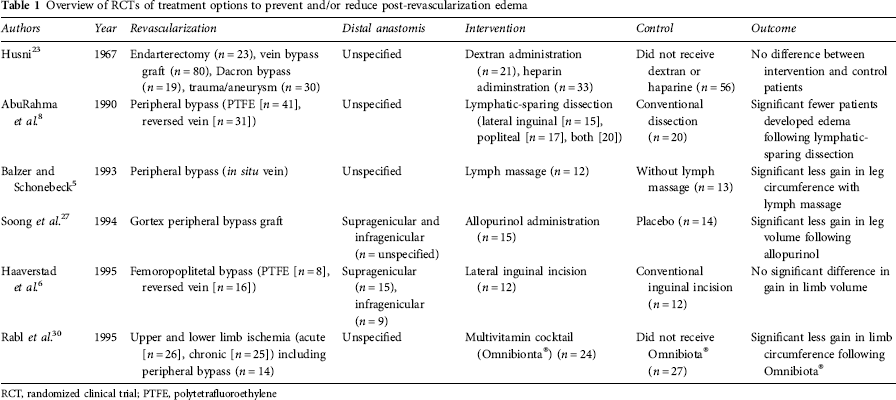
RCT, randomized clinical trial; PTFE, polytetrafluoroethylene
Pre-revascularization edema
Edema does often accompany peripheral arterial disease (PAD). This edema is assumed to be a combination of lymphatic and ischemic edema. Edema is caused by disturbances in the microcirculation in combination with a decreased perfusion pressure due to atherosclerosis of larger peripheral arteries. 2 Due to a decreased arterial pressure, the blood flow velocity in the capillaries is reduced. This mechanism makes the pre-capillary arterioles prone to collapse. Due to spasms, microthrombosis formation can occur in arterioles. Microthromboses can cause interstitial space fluid accumulation and swelling of endothelial cells. The capillary bed will eventually collapse, causing ischemia. Ischemia results in loss of smooth muscle tonus in the arteriolar wall and to loss of vasoconstrictive reflexes. Thus, in depending limbs, an increased capillary hydrostatic pressure can be achieved.3,4 This causes a typical relief in patients with ischemic rest pain, but will result in excessive capillary filtration that promotes further edema development. 3 A sequence of microvascular and macrovascular deterioration eventually causes muscle atrophy and ischemia. These events eventually trigger aggregation of blood platelets and leukocytes which activate the local immune system. Finally, the venous and lymphatic circulations are hindered as a result of a decreased arterial circulation and interstitial edema. Pre-revascularization edema is reported to be present in up to 80% of patients suffering from PAD Rutherford category 4, 5 and 6. However, due to coexisting muscle atrophy, this edema is easily overlooked. 5
Incidence and dimensions of post-revascularization edema
Occurrence of edema after peripheral bypass revascularization

MRI, magnetic resonance imaging
Pathophysiology of post-revascularization edema
A local inflammatory response to surgical trauma, together with the patient's immobilization, may account for some edema. However, the severity and duration of the swelling following peripheral bypass surgery suggest that other factors are involved. Five main pathophysiological mechanisms that might lead to postoperative edema have been formulated in literature: hyperemia, an increase of microvascular permeability, reperfusion-associated inflammation, and lymphatic and venous disruptions. In this review, we will discuss these possible mechanisms.
Hyperemia
A hyperemic response can be seen in the majority of patients following successful peripheral bypass surgery. This response has been suggested to be a cause of emerging edema. The mechanisms that prevent hyperemia from occurring in healthy persons are briefly discussed in this subsection, followed by mechanisms that might cause hyperemia.
The blood flow in a leg decreases by about 50% when changing posture from supine to standing in healthy persons. Reflex vasoconstriction that leads to a decrease in blood flow is affected by a local neurogenic mechanism with a small contribution of a local myogenetic response, in addition to a centrally elicited sympathetic component. 3 This auto-regulation mechanism is defined as the maintenance of a constant perfusion pressure with variations of arterial blood flow. 17 On the venous side, pooling occurs due to gravitational forces in a standing position. This results in increased autonomic activity, thereby increasing the vascular tone causing a reflex vasoconstriction at the arterial side. 18
Loss of the auto-regulation mechanisms is thought to contribute to a hyperemic response following peripheral bypass surgery. Malfunction of the auto-regulation mechanisms might be caused by damaged resistance vessels. Structural damage of resistance vessels could be caused by an elapsed ischemic episode. In studies by Simeone and Husni, Sumner and Folse 20 and Wellington et al., 21 it was found that both edema and hyperemia occurred after successful peripheral revascularization. In these studies, wash-out of 133Xenon was used as a flow indicator. Henriksen 17 demonstrated that auto-regulation mechanisms were lost in patients who suffer from severe PAD (Fontaine stage III). In healthy controls and in patients suffering from less severe stages of PAD (Fontaine stage II), this did not occur. A study by Jacobs et al. 2 revealed that patients who developed postoperative edema after peripheral bypass reconstruction had a lowered (peak) red blood cell velocity preoperatively found in the capillaries in the nail fold of the toe. According to the authors, these low flow velocities suggest a severely affected microcirculation. In the patients who developed edema, a significant increase in flow velocity was observed after revascularization compared with the situation prior to surgery. This phenomenon was not seen in patients without edema. The magnitude of the hyperemic response was found by several authors to correlate with the severity of the ischemia.4,19-21 Sumner and Folse 20 demonstrated that post-reconstructive hyperemic legs exhibited only a limited capacity to respond to stimuli which usually produce vasodilation or vasoconstriction compared with the normal legs. In view of the above findings, hyperemia is suggested to attribute to edema formation; however, no correlation was found between the disturbances in local blood flow regulation and edema using the 133Xenon technique in a study by Eickhoff and Engell. 4 Edema developed independently of hyperemia and was sometimes found without hyperemia and vice versa. Even so, Persson et al. 16 were not able to correlate the magnitude of ischemia to edema. Another objection to the ‘hyperemia theory’ is that it provides no satisfactory explanation for the rare occurrence of edema after more proximal aortofemoral revascularizations. On the other hand, edema is sometimes absent, or to a lesser extent pronounced after unsuccessful revascularizations, indicating that factors depending on a successful vascularization are important.16,19 The findings of Payne et al., 22 who measured limited edema development after percutaneous procedures, support this.
Microvascular permeability
It could be hypothesized that in patients with severe microcirculatory disorders, edema formation does not occur before surgery (because of the low arterial pressure), but that restoration of the circulation after revascularization leads to a rise in arteriolar and capillary pressure. When the capillary perfusion is restored following peripheral bypass surgery, edema may develop as a result of structural adaptations in the microcirculation. The occurrence of post-revascularization edema might be explained by loss of auto-regulation (and thus impairment of a vasoconstrictive response) that leads to an augmented increase in capillary hydrostatic pressure in low-pressure vascular beds. Husni 23 postulated that re-establishment of normal arterial pressure in a vascular tree adapted to reduced pressures produced overstretching of the vessels.7,19,24 This is supported by Junger et al., 25 who found increases in transcapillary transport of sodium fluorescein with the degree of ischemia in patients with lowerlimb ischemia. In a study by Campbell and Harris, 7 it was found that serum concentrations of total protein and albumin were reduced postoperatively, but in general fell within the reference range. A three-fold increase in albumin concentration was found in the operated leg after a peripheral reconstruction, probably accumulated in the interstitial spaces. 7 The loss of albumin might occur due to increased capillary permeability in ischemic vascular beds.
Reperfusion-associated inflammation
Generation of oxygen-derived free radicals during reperfusion might also attribute to edema formation.26,27 These free radicals induce the lipoxygenase pathway. 26 Lipoxygenase-derived products will injure cells by damaging the cell membranes. 28 Subcutaneous tissue especially, is rich in polyunsaturated fatty acids, making this tissue vulnerable to lipid peroxidation. 26 Oxygen-derived free radicals are also thought to activate the complement cascade. 28 The break-down products of complements are potent chemoattractants, which stimulate leukocytes and up-regulate adhesive molecules. 28 As a consequence, attracted leukocytes are thought to release more oxygen-derived free radicals and proteolytic enzymes, further damaging the endothelium, and thereby increasing capillary permeability. 29 In studies by Soong et al. 27 and Rabl et al., 30 increased parameters for lipid peroxidase activity were associated with the presences of post-revascularization edema.
Lymphatic disruption
Lymphatic damage has been postulated as a cause of edema. Based on lymphatic theories, there are two main lymphatic patterns in the occurrence of edema following peripheral bypass reconstruction: (1) interruption of the lymphatic circulation due to surgical damage; and (2) diffusion of the lymph outside the vessels without appreciable impairment of the lymphatic flow. Research on lymph disruption and function has been performed using lymph angiography and lymph scintigraphy. Compared with lymph angiography, lymph scintigraphy is a non-invasive technique to study both the morphology and the kinetics of the lymphatics.31,32 More recently, X-ray computed tomography (CT) and magnetic resonance imaging (MRI) techniques have been used as well to study anatomical characteristics of edematous limbs. Lymphatics are mainly responsible for the maintenance of the interstitial pressure in the subcutaneous compartment at a subatmospheric level, which is a vital factor in the prevention of edema. 33 During vascular surgery, lymph nodes surrounding the femoral artery and the popliteal artery are vulnerable to damage. Vaughan et al. 14 and Shishido et al. 34 found that only a few of the superficial lymphatic channels remained after peripheral surgery. Lymph vessels are especially prone to damage when a venous peripheral bypass is constructed. 11 Lymph angiograms showed a greater extent of disruption to the lymphatics when the saphenous vein was used compared with artificial grafts. 11 Rejoining of severed lymphatics occurs occasionally, but more frequently, the lymphatic function is re-established by the formation of newly formed channels and the enlargement of the remaining lymphatic channels.9,14,35
In studies by Porter et al. 9 and by Vaughan et al., 14 it was demonstrated that the magnitude of inguinal lymphatic damage correlated to the extent of postoperative edema by using lymph angiograms. Haaverstad et al. 6 found that larger lymphatic disruptions represent a larger volume increase postoperatively as compared with smaller disruptions. Based on lymph scintigraphy, Hannequin et al. 10 found that lymphatic flow was not different in patients suffering from edema versus patients not suffering from edema after a peripheral bypass operation. However, in this study, the presence of edema is judged on cut-off points, possibly resulting in arbitrary grouping.
Others also found that the presence of morphological abnormalities correlated with edema, based on lymph scintigraphy findings. 36 Morphological abnormalities (including diffusion) might be the result of dysfunction and increased permeability of the lymphatic walls. 34 Campbell and Harris 7 showed increased albumin content in limbs and a correlation with the presence of edema after peripheral bypass reconstructions. Fernandez found an increased wash-out of 125Iodine-labeled albumin in edematous limbs after peripheral revascularizations, indicating an increased lymphatic flow of the superficial lymphatics. 13
These results agree with Stranden and Kramer, 37 who found that intralymphatic pressures and the threshold pressure necessary to induce spontaneous lymphatic contraction were normal after peripheral reconstruction. Based on their findings, they could not prove that post-revascularization edema was caused by an insufficient lymph transport capacity. However, based on remarkable findings by Persson et al., 16 lymph damage as a cause of edema could not be ruled out. They witnessed the development of edema after only an exploration in the popliteal region, although not as pronounced as after successful revascularizations. Danese et al. 35 showed in an animal model that edema occurred within 24 hours after transection of lymphatic trunks in the thigh. Edema became the most pronounced 24 hours after surgery and disappeared by the fifth week.
Modern imaging techniques like CT and MRI make it possible to study anatomical characteristics of edematous limbs.37-41 MRI investigations have revealed that the edema was located around the entire circumference of the leg and restricted to the subcutaneous tissue. These findings correspond with previous CT studies. 38 In patients with chronic lymph edema, all edema was in the subcutaneous tissue as well. The similarities between chronic lymphatic edema and postoperative edema support the idea that edema formation after peripheral bypass surgery is, at least partly, caused by impaired lymphatic drainage, as most of the lymph originates in the skin and subcutaneous tissue. 42
Persisting edema is regularly seen in trauma patients. 43 It is postulated that a persisting immune response may impair lymphatic transport. Damaged lymphatic structures could also leak lymph-containing microorganisms that are ‘physiologically’ transported from the foot to the skin. 42 High levels of cytokines and chemokines might impair lymphatic transport as well. 43 Cytokines and chemokines released from resident and infiltrating cells are associated with dilation of lymphatics. Furthermore, heme-containing substances such as hemoglobin, oxyhemoglobin and myoglobin absorbed from the inflamed tissue inhibit lymph vessel contractility, as seen in normal lymphatics.34,44,45 It cannot be ruled out that tissue damage occurring during construction of a peripheral bypass revascularization triggers a similar cascade.
Venous disruption
Few authors have mentioned venous disruptions as a cause of post-revascularization edema. 6 However, it is unlikely that the removal of the greater saphenous vein alone caused edema of the leg.14,23 Urayama et al. 36 found no association between post-reconstructive edema and venous obstructions using radioisotope venography. AbuRahma et al. 8 also did not find a relation between deep venous thrombosis (DVT) and postoperative edema.
Nowadays, a DVT is very uncommon after peripheral bypass reconstructions in patients receiving anticoagulatory therapy. Due to impaired lymph drainage or hyperemia, venous flow is increased, which may decrease the risk of DVT formation. However, partial or complete obstruction of the deep venous system by a thrombosis was a common cause of postoperative edema of the leg. According to a study by Hamer et al. 12 in the 1970s, DVTs were found in 43% of patients who underwent peripheral revascularization and DVTs were correlated with a calf circumference increase in excess of 4.5 cm. Distal anastomosis of the vein graft to the artery are more often accompanied by venous thromboses than anastomosis above the knee joint. 12 The emerging thrombophlebitis might invade perivenous tissue, resulting in the development of lymphatic obstructions as a result of scar formation at the site where inflammation had subsided. 34
A condition in which edema is regularly observed is after a vein harvest, when the vein has to be used as a coronary artery bypass graft. 46 In these patients, an impaired venous drainage, as well as lymphatic and soft tissue damage, are hypothesized to contribute to the formation of edema, although this has not been studied in detail. 47 The contribution of venous impairments in emerging edema after peripheral bypass reconstructions is likely to be limited in the absence of an occlusion by a DVT. Phlebograms and venous pressure in groups of patients developing edema following vascular reconstructions have shown to be normal in most studies.8,11,23,48
Summary of pathophysiological mechanism
The pathophysiological mechanism of edema following peripheral bypass surgery is likely multifactorial. MRI studies have shown that post-revascularization edema is located in the subcutaneous compartment, similar to lymphatic edema. 6 Lymphatic disruptions should therefore be considered as a major factor in edema development. A large attribution of hyperemia was only demonstrated in animal models. 20 Hyperemia, reperfusion-associated inflammation and an increased capillary permeability contribute probably only to a limited extent to edema development following peripheral surgery. This is likely to be illustrated by the limited extent of edema development that occurs following endovascular revascularizations. 22 The attribution of venous disruptions are very limited as a cause of edema development in the absence of a DVT. 12
Treatment and prevention of edema
Treatment of edema, irrespective of the pathophysiology, should achieve a net absorption of fluid from the interstitial space into the vascular or lymphatic compartment. 33 In general, treatment strategies strive to improve microcirculation and arterial perfusion, to reduce discomfort to the patient and to promote the patient's rehabilitation process following surgery. The following treatment options to prevent and to treat postoperative edema will be discussed: lymph drainage, lymphatic-sparing surgery, compression stockings, antioxidative therapies and intermittent pneumatic compression (IPC) (Table 1).
Lymph massage techniques
Lymphatic disruptions are very likely to attribute to post-revascularization edema. Postoperative edema had been shown to be mostly absent following proximal arterial reconstructions4,7,20 or to be present in a limited magnitude following endovascular revascularizations. 22 In both these procedures, the inguinal lymphatics are spared. Lymphatics surrounding the femoral and popliteal artery are very vulnerable to damage. Facilitation of the lymphatic flow by applying lymph massage therapy has been proven to be an effective method to reduce post-revascularization edema. A reduction in leg circumference was noticed on the sixth day after surgery, versus on the 12th day in a control group, in an RCT by Balzer and Schonebeck. 5 Franzeck et al. 46 came to similar conclusions for the treatment of lymph edema, when patients were treated with manual lymph massage in combination with compression therapy.
Lymphatic-sparing surgery
The effects of lymphatic-sparing dissection when constructing a peripheral bypass have been investigated by two teams led by AbuRahma et al. 8 and Haaverstad et al. 6 AbuRahma and colleagues used lymph angiograms to conclude that the risk of postoperative edema after a peripheral bypass reconstruction was more than eight times larger when a conventional dissection was used, versus a lymphaticsparing dissection in the inguinal and popliteal region. The lymphatic-sparing dissection consisted of a lateral incision in the groin and at the site of the popliteal artery without mobilizing the neurovascular bundle. However, the results are in contrast to a study by Haaverstad et al. 6 In this study, a conventional medial incision was compared with a lateral incision in which attention was focused on the preservation of the lymphatic network. No significant differences were found in the amount of edema that occurred in the treatment groups. However, it was found that larger lymphatic disruptions do represent a larger volume increase postoperatively as compared with smaller disruptions. A shortcoming in the study by AbuRahma is that the analysis was based on cut-off points rather than on continuous data like the study by Haaverstad. This might have biased the outcome. Given the observations displayed in Table 1, it is very unlikely that edema did not occur in the study by AbuRahma. It would be more likely to assume that edema occurred to a lesser extent following lymphatic-sparing surgery. Based on these studies, it is very likely that post-reconstructive edema is associated with lymph damage and (adjacent) tissue trauma. However, the effects of a modified incision on the amount of edema remain questionable.
Compression stockings and elevation
External compression devices, such as stockings or bandages, are commonly used to treat edema. Compression stockings are reported to exert at least a pressure of 30 mmHg. 49 The use of compression stockings is mostly based on clinical experience. So far, a beneficial effect of the application of compression stockings following peripheral surgery has not been demonstrated. The aim of compression is to increase pressure on the interstitial space 33 and to augment the peripheral circulation by reducing peripheral arterial resistance. 49 At the arteriolar level, an increase in arterial flow is witnessed. This is the result of smooth muscle relaxation precipitated by the release of an endothelialderived relaxing factor, which has been shown to be nitric oxide. 50 Supplementary to compression therapy, leg elevation could be practiced. By elevating the leg, the hyperemic response could be subsided. Auto-regulation mechanisms normally cause reflex vasoconstriction on the arterial side, but are impaired in patients suffering from severe stages of PAD. 20 Leg elevation could slow down edema formation as it wanes the effects of impaired auto-regulation mechanisms and increased microvascular permeability.
Antioxidative treatment
It has been hypothesized that reperfusion-associated inflammation could be moderated with the administration of antioxidants. Successful edema prevention strategies with intraoperative administration of allopurinol and a vitamin cocktail during revascularization surgery have been reported by Soong et al.26,27 and by Rabl et al. 30 In both RCTs, a reduction of edema formation was found. According to Rabl et al., 30 the effect of a multivitamin cocktail resulted in a decrease in development of lipideperoxidase products and in reduced edema formation after revascularizations, after chronic and acute arterial occlusions. Soong et al. 27 found a 50% decrease in swelling after allopurinol administration, although the working mechanism of allopurinol remains unclear. The use of antioxidants did not become widespread in the vascular practice, even though the results of these trials were encouraging.
Intermittent pneumatic compression
Intermittent IPC has also been proven effective in edema reduction originating from orthopedic lower-limb surgery,51,52 lymphatic disorders53,54 and venous disorder.54,55 The use of IPC has been proven effective as a DVT prophylaxis 51 and for blood flow enhancements in arteries affected by PAD 56 60 . McGeown et al. 61 thought that compression emptied the terminal lymphatics, allowing drainage of fluids from the interstitium, and also possibly assisted in moving fluid from the interstitium to the lymphatics. IPC does not assist flow in the major lymphatics directly, nor does it transport fluid within the tissue directly. 62 It is assumed that with the use of IPC, proteins are cleared from the tissue as well.62,63 However, if it did not, edema would reoccur quickly and clinical results are generally satisfactory. 53 IPC of the leg generates an increase in arterial blood flow in both healthy subjects and in patients suffering from PAD.56,58,59,64 Blood flow in the calf can increase by a factor of four when using IPC.56,60 This effect has been demonstrated in native arterial blood flow, as well as in infragenicular peripheral bypass grafts. 59 The venous flow velocity in the common femoral vein increases during compression by a factor of 2.5 to 3, which indicates that venous emptying is facilitated.65,66 Blood is no longer cleared from the veins when patients are immobilized, due to an insufficient muscle pump function, which can result in venous hypertension. This allows fluids to move out of the capillaries and thus leads to edema formation. 55 The role of intermittent compression in chronic venous insufficiency is primarily to disperse edema in a similar way as in the treatment of lymph edema. The use of an intermittent pneumatic pump has proven effective to reduce edema and wound infections after coronary arterial bypass grafts in a study by Ho et al. 47 The device used compressed the foot, calf and thigh up to 70 mmHg pressure, in cycles of 15 minutes each, making it merely an external compression device rather than IPC. So far, the efficacy of IPC in the reduction of edema emerging after peripheral revascularization has not been investigated.
Conclusion
The occurrence of lower-limb edema is a well-known problem since the introduction of the peripheral bypass procedure in the late 1940s. Postoperative edema may extend the duration of in-hospital stay and out-of-hospital care. The exact pathophysiology of edema remains unclear, but is likely to be multifactorial. These factors probably consist of hyperemia, microvascular permeability, reperfusion-associated inflammation, lymphatic disruption and venous disruption. Lymphatic disruption, especially, is likely to play a crucial role. However, no consensus appears to be reached on effective lymphatic-sparing methods.6,8 Successful antioxidative treatment options have been published. Both lymph massage treatment techniques and the use of compression stockings are common. IPC strategies have been proven to be successful for edema treatment of other pathophysiology. When future less-invasive treatment techniques like remote endarterectomy, 67 percutaneous stenting and endovascular bypasses, 68 prove to be successful and (cost)-effective, postoperative edema might be minimized. Until then, careful lymphatic-sparing dissections should be executed when performing a peripheral bypass reconstruction. Postoperatively, the use of compression stockings and leg elevation are currently the golden standards.