
Abstract
Most surgeons make their decision to amputate or perform limb salvage of a mangled extremity based on scoring systems and grading of acute ischemic limb. We report on a child in whom limb salvage was achieved in spite of a clinical picture of irreversible ischemia with high mangled severity scores. Attempts to revascularize the mangled extremity of children are recommended, regardless of their severity scores and condition of the foot.
Introduction
The decision to amputate or perform limb salvage of a severely injured mangled extremity remains a difficult dilemma for vascular and orthopedic surgeons. 1 Multiple scoring systems 2,3 and grading of acute ischemic limb 4 have been developed to assist surgeons in making this decision. Advances in vascular and orthopedic reconstruction have made it is possible to manage many severely injured limbs with salvage procedures. We report a case of an eight-year-old child with crush injury of the lower limb. Assessment of the patient revealed a clinical picture of irreversible ischemia with high mangled severity scores. The limb of the child was salvaged after successful revascularization.
Case report
An eight-year-old boy was referred from a remote hospital to our vascular unit 20 hours after a motor car injury of his left lower extremity. This time was spent in resuscitation, clamping of the femoral artery and transport. On arrival at the hospital, there was an open Gustilo type IIIc injury of the mid-femur with circumferential loss of most of the skin and muscles. There was also a loss of about 5 cm of the superficial femoral artery and femur. The femoral vein and sciatic nerve were contused. The left leg was bluish, mottled and cold with rigor of the muscles (Figure 1). An examination revealed absent sensation, motor power and Doppler signals over the left leg. The mangled extremity severity score (MESS, a point system based on injuries to skeletal soft tissue, limb ischemia, age and shock)
2
was 10 and the mangled extremity severity index (MESI, a point system based on injuries to the four major tissue systems: integument, nerve, vascular and bone)
3
was 29. There was controversy in the management among surgeons between salvage or amputation. Due to the presence of the intact sciatic nerve and age of the patient, the final decision was to revascularize the limb, observation and subsequent early amputation if required. A shunt was inserted between the two ends of the artery to restore the blood flow to the limb. Femoro-femoro-tibial external fixation was performed. Interposition saphenous vein graft from the other limb was used to repair the superficial femoral artery (Figure 1). Four-compartmental fasciotomy was performed. The child received strong broad-spectrum antibiotics (piperacillin sodium and tozabactam plus metronidazole, then vancomycin hydrochloride was added, and then meropenem replaced piperacillin), hydration and prophylactic anticoagulant (enoxaparin). The circulation was restored to the leg and there were good pedal pulses. There was a stormy post-operative period (fever, tachycardia, hypotension for more than two weeks). The patient developed severe wound infection and sloughing of areas of the epidermis (Figure 2). Multiple surgical wound debridements were performed. There was also hypoalbuminemia, and a highly elevated level of serum myoglobin (6164ng/ml) and creatine Phosphokinase (>19697 units/1). However, there was no myoglobinuria. All these laboratory results were back to normal within 10–14 days. Two months later, the wounds were covered with healthy granulation tissue and a split thickness skin graft was applied (Figure 2). Three months postoperatively, the external fixation was removed and intra-medulary nails were inserted. Six months following the injury, all wounds were healed and the child was able to elevate his leg and walk with knee-ankle orthotics without crutches (Figure 3). The protective sensation was regained by most of the leg.
(a, b) Extent of damage of skin, muscles and femur at mid-thigh, (c) Mottled leg. (d) Saphenous vein interposition graft (arrow) (a) Severe wound infection. (b) Sloughing of the epidermis of the leg and foot, (c, d) Split thickness graft (a) The child can stand with knee-ankle orthosis without crutches, (b) All wounds were healed and the child was able to elevate his leg. (c, d) X-ray showing anteroposterior and lateral views of the left femur (6 months postoperatively) with intra-medulary elastic nails and good callus at the fracture site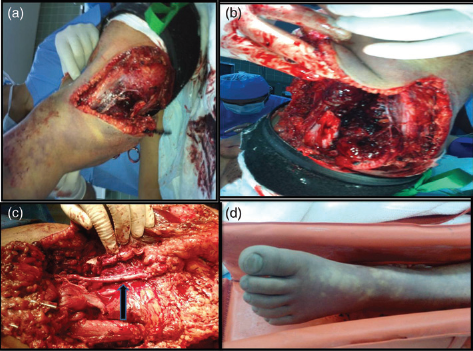


Discussion
Amputation of a mangled extremity, especially in children, is usually horrible for both the patient and the surgeon. The two lower-extremity severity scoring systems 2,3 that have been developed in the last few decades may provide objective criteria to assist surgeons to determine the fate of a mangled extremity. The value of these scores has been shown in children5,6 and adults. 7 If MESS is more than 7 or MESI is more than 20, the amputation rate is expected to be 100%. However, MAE previously showed that these severity scores are not predictive of limb salvage. 8 The same results were confirmed in other reports.9,1010 The difference between these conflicting reports may be due to the cases that had primary amputation. They were included in the analysis of the former studies whereas in the latter ones they were excluded. The number of cases with a MESS >7 was very low in the former studies compared with the latter ones.
Revascularization of a severely ischemic limb causes reperfusion injury which causes more damage than ischemia alone locally and initiates a remote organ injury. 11 Although there was high serum myoglobin in our patient, there was no myogloninuria or significant sequelae of reperfusion syndrome. We performed prophylactic fasciotomy, which prevented compartmental syndrome from developing. Sepsis and other infectious complications were reported in our case and most previous studies. 12 There was controversy about the incidence of death from infectious complications in primary and delayed amputation in severely injured limbs. Some showed a higher rate after primary amputation. 13 Others reported a higher rate with delayed amputation. 12 In our case, extensive wound debridements and strong antibiotics prevented local and systemic complications of sepsis.
The presence of ischemic rigor traditionally represents irreversible local damage to muscle in the adults and is an indication of limb amputation.4,14 However, in the present case and others, 14 limb salvage was reported in pediatric patients despite the presence of a severely ischemic limb with muscle rigor.
In conclusion, limb salvage should be attempted for severely injured lower limbs of children with intact sciatic nerves, regardless of their severity scores and condition of the foot.