
Abstract
Purpose
We report our experience of a paediatric orthopaedic network, based on a ‘hub and spoke’ model, covering the South West of the United Kingdom. We identify the areas of most clinical concern, the effect of the network on stream-lining patient management and the benefits of the network to the clinician.
Methods
Prospective data were collected from the minutes of the bi-annual meetings of the South West Paediatric Network (UK) between November 2006 and May 2012. Data collected included details of the condition, previous treatment, problems, complications and advice given. Cases continue to be followed up in subsequent meetings.
Results
In total 131 cases were included and hip conditions were discussed most frequently (35.1%). The most common indication for discussion was to support and confirm the local management plan. In total, a mean average of 8.75 cases in total were presented per consultant during the study period, with those within ten to 12 years of starting independent practice presenting the majority. The clinical outcome for patients discussed in this forum was local provision of care in 74%, with transfer to the regional centre in 15.7%. Following advice, 14% of direct referrals were given appropriate advice and avoided a journey to the tertiary centre.
Conclusion
The network has enabled local provision of care, reduced the burden of travel on patients and prevented unnecessary referrals to the tertiary centre. Additionally, it provides a mechanism to reassure and educate clinicians.
Introduction
Pressures on paediatric orthopaedic services have been increasing over recent years. 1 Although outcomes, length of stay and healthcare costs are improved in paediatric orthopaedic subspecialty led units,2,3 this rising demand is set on a backdrop of limited resources4,5 and mandate the development of more efficient programmes of service delivery. 6
The British Orthopaedic Association advocates the establishment of managed clinical networks for elective orthopaedic conditions. 7 National health authorities, such as NHS England and the Royal College of Paediatrics and Child Health, have supported networks as a way to improve patient referral pathways and distribution of services.8,9
Clinical networks have been widely used in other paediatric subspecialties to promote research and education. These have largely focused on the treatment of rare conditions or collection of large amounts of demographic data, but have not shaped service provision across a region.10–12
When paediatric orthopaedic care is centred in tertiary referral units that provide high-quality care, convenience and access for patients can be challenging. These patients often have to travel significantly further than adult patients to receive comparable care. 13
A paediatric orthopaedic network has existed in the South West of the United Kingdom for over 20 years. The impact of this arrangement was studied to determine the areas of most clinical concern, the effect on the patient journey and the rationale for discussion of complex cases within the network.
Materials and methods
All paediatric orthopaedic consultants from South West England and South Wales contribute to the South West Paediatric Orthopaedic group (Fig. 1). 14 This involves 13 hospitals, serving over five million people. 15
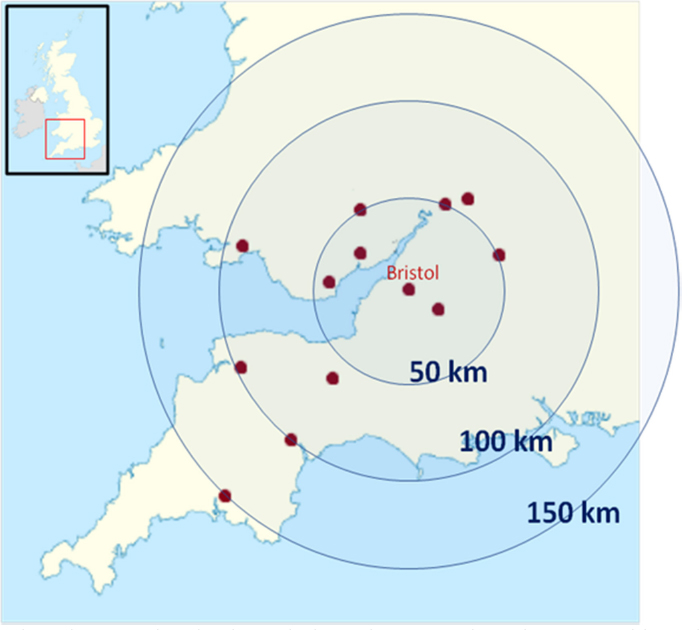
Map of the South West United Kingdom showing the distance (blue circles) of the peripheral centres (red dots) to the tertiary referral centre in Bristol. Adapted with permission. 14
The network is based on a ‘hub and spoke’ model,16–18 with the principle hub being The Royal Hospital for Children, Bristol and major spokes in Plymouth and Cardiff.
Data collection
The data in this observational cohort study were prospectively recorded between November 2006 and May 2012, using an anonymised electronic database of the minutes of the twice annual network meetings. The data had patient identifiable information removed and included the patient's age, diagnosis, relevant medical history, previous treatment, the consensus advice from the meeting and the subsequent clinical outcomes. The number of years of experience of the named consultant was documented. The patient notes and investigations were reviewed by the local consultant, ensuring accuracy of the recorded data.
Data analysis
The data were analysed to determine the frequency that each condition was discussed, requiring consensus opinions from the paediatric orthopaedic consultant group. The diagnoses were categorised into areas (Table 1) of which the most common involved hip conditions, primary bone lesions, post-traumatic complications and infection.
Frequency of conditions, problems and recommendations
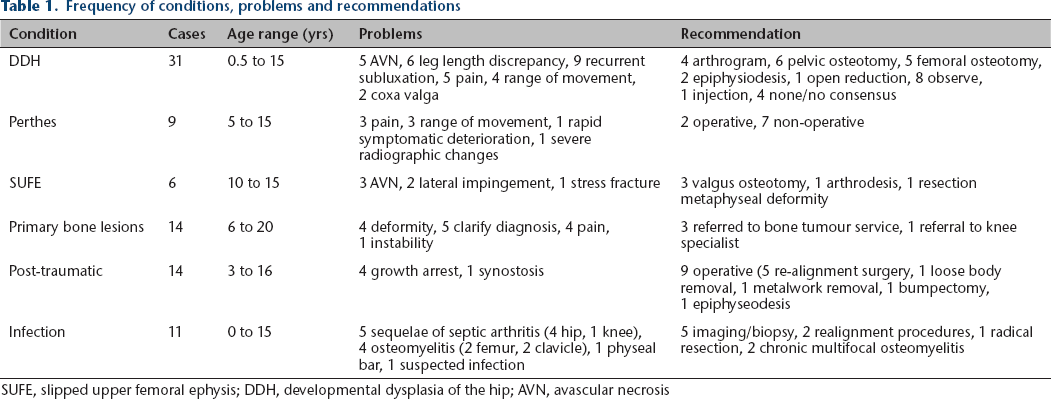
SUFE, slipped upper femoral ephysis; DDH, developmental dysplasia of the hip; AVN, avascular necrosis
The advice given by the network was reviewed to determine how it affected management. We identified whether the patient underwent treatment locally or required onward referral, and if non-operative or operative treatment was necessary. The patient was followed up at subsequent meetings and the clinical outcome was assessed by the network's consultant body.
Microsoft Excel 2007 (Redmond, Washington) was used for data analysis, descriptive statistics and graphs.
Results
There were 131 cases discussed, 70 of which had detailed follow-up at the time of analysis. We estimate that there are a total of 48 000 paediatric orthopaedic outpatient attendances in the area covered by the network. 19 At each meeting, six to 16 cases were discussed (mean 10.1 standard deviation (sD) 3) by seven to 22 clinicians (mean 13.9 SD 4.1) for an average of 16.8 minutes each. The majority of attendees were consultant orthopaedic surgeons, radiologists and rheumatologists. Orthopaedic trainees who were interested were invited to attend, but attendance was not mandatory as discussions were too detailed for the disinterested trainee. In general, the children themselves did not attend the meetings, except for two cases.
Conditions which were discussed are shown in Figure 2. The broad categories of hip conditions, bone lesions, post-traumatic deformity and infection were the most common, and had sufficient data for discussion.
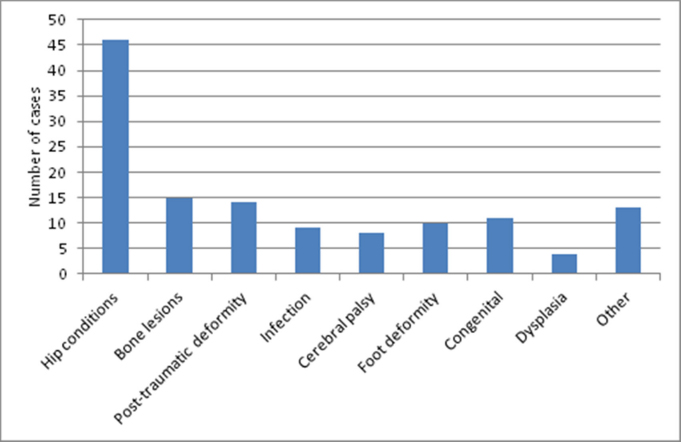
Category of cases discussed.
Hip conditions
Hip conditions were the dominant category (35.1%) of all cases discussed (Table 1). The most common was developmental dysplasia of the hip (DDH), with 31 cases presented; eight children suffered from bilateral DDH. Before discussion, a surgical procedure had been undertaken in 28 patients (90.3%) (Fig. 3). Just over half had had an open reduction alone with femoral and pelvic osteotomies being the next most frequent procedure. The most frequent clinical problem was recurrent subluxation or dislocation (Fig. 4) and there were five cases of avascular necrosis.
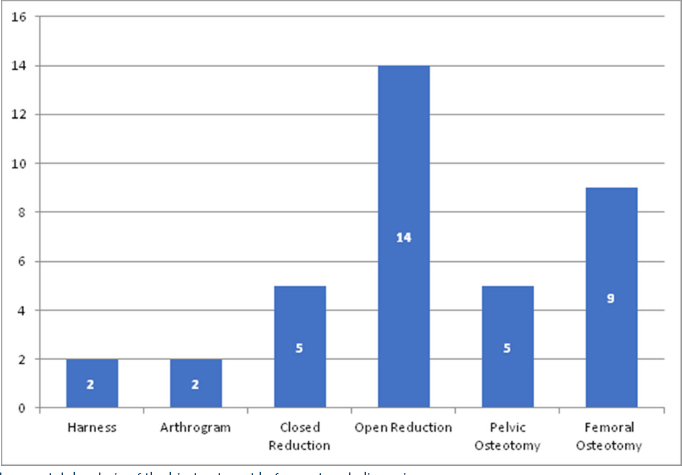
Developmental dysplasia of the hip treatment before network discussion.
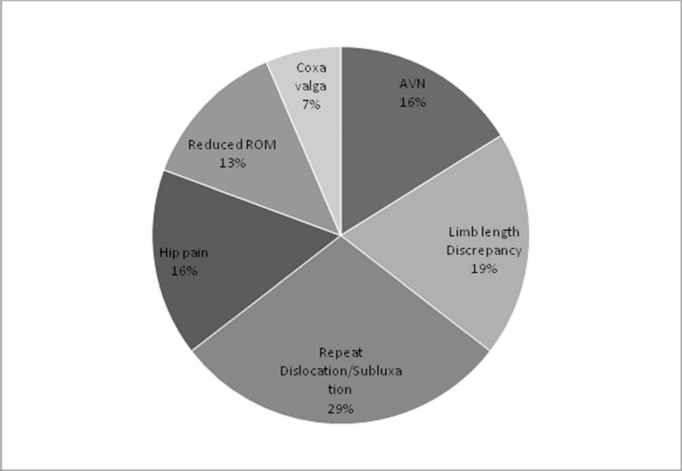
Developmental dysplasia of the hip complications (ROM, range of movement; AVN, avascular necrosis).
Perthes’ disease was discussed in nine cases and previous osteotomies had been undertaken in 33% of these children. Pain and range of movement were the most common reasons for discussion. One patient was discussed due to a rapid clinical deterioration in the fragmentation stage, one asymptomatic patient was discussed at the reossification stage, but the majority of children (five out of nine) were at the healed stage. Chronic pain and stiffness were the commonest problems. Operative management was recommended for two children and both were managed locally. For the remainder, the advice was to observe.
Six children were discussed with slipped upper femoral epiphysis and all had late complications. Five patients (83%) were advised an operation. Further MRI imaging was suggested for two patients.
Primary bone lesions
The 15 patients with painful presumed benign bone or muscle lesions were discussed. Three patients had potential malignancy and were referred to the extra-regional bone tumour service. One child was referred to an adult knee specialist. The remaining 71% were benign lesions managed locally.
Post-traumatic complications
In total, 14 patients were presented with complex problems after a traumatic injury. Eight cases were associated with a deformity from malunion, four cases were associated with growth arrest and there was one synostosis. Parental litigation was specifically raised as an issue in one case. The question of operative management of post-traumatic deformity was queried in 13 cases, but the network advised operation in only nine cases, with five for realignment surgery. Three cases were referred out of the region: two complex malunions and one hip labral tear.
Infection
Nine cases relating to infection were discussed: divided evenly between sequelae of septic arthritis and osteomyelitis (Table 1).
Further investigation was recommended for five cases, resulting in one diagnosis of juvenile rheumatoid arthritis and three patients were recommended an operation (Table 1). An infection-like presentation was seen in two children and these were subsequently referred to the paediatric rheumatologists.
The patient journey
Patients and parents were informed that their case would be discussed and the outcome explained at their next clinic appointment. In general, the patients did not attend the meetings to minimise distress and the burden of travel. Two patients did attend a meeting, both with complex multilevel problems (due to cerebral palsy and dysplasia) and did not describe any distress, either at the meeting or subsequently to the local consultant.
After discussion with the network, of the 70 patients with complete documented follow-up, 72.8% underwent local management, while 18.6% needed referral to the tertiary centre and 8.6% were referred to a national specialist (Fig. 5). Consultants from the spokes presented 20% of cases for direct face-to-face referrals, anticipating that the child would travel to the hub. However, after the meeting only 17.1% needed to make this journey.
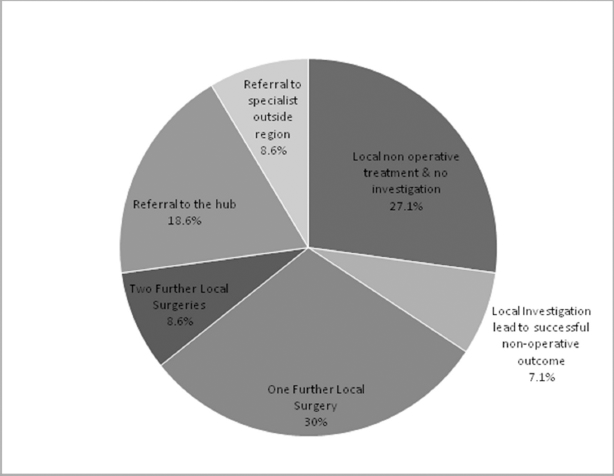
Outcome of patient journey.
After the network meeting, the clinical outcome of treatment was reported back to the group as successful in 68.6% of cases, based on patient feedback. There were 24 successful cases of non-operative treatment and 19 good results after one further operation. Some patients required further input from the network after the initial recommendation, including five good results achieved after two further operations. Of these complex cases, 5.7% were noted to have poor outcomes, even after consensus advice and management.
Rationale for cases discussed with the network
The consultant body chose patients for presentation for at least one of a variety of reasons (Fig. 6). Gaining a consensus opinion to confirm the local management plan was the most common reason, with the proposed local management being non-operative in 31.6% and operative in 11.8%. The next most common reason was to receive new guidance to plan a new operative treatment locally (19.7%). In all, 18.4% of cases were presented as a face-to- face onward referral to another consultant in the network. Another 18.4% were presented to teach and share a learning point and, of these, 79% were presented by senior colleagues with at least 12 years of experience.

Rationale for cases discussed.
There was a mean average of 8.75 cases presented per consultant over this period (SD 4.86). The most cases were presented by consultants within ten to 12 years of commencing their post (Fig. 7).
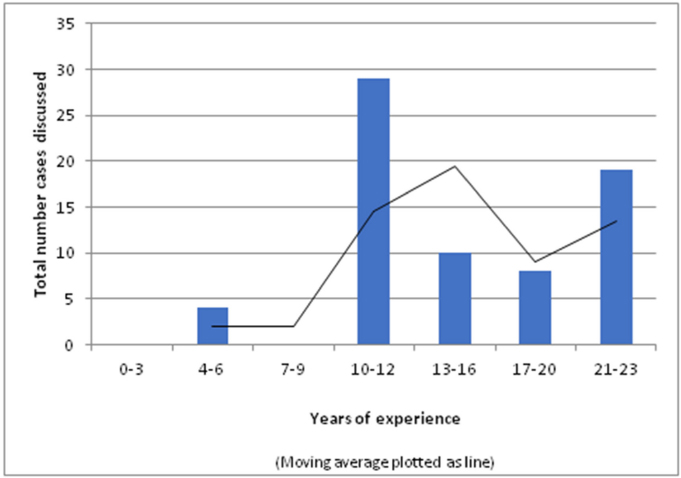
Histogram of cases presented by experience of consultant.
Discussion
Clinical networks are an effective mechanism for the integration of care, creating a climate of continual learning and development, and delivery of care as locally as possible for the patient.8–9,18 A review of paediatric service development by the Nuffield Trust recommends a move towards networks of care. 20 The role of regional networks has been clarified by the success of the major trauma networks. 21
There are few published data on this complex paediatric orthopaedic case-load, the interaction between secondary and tertiary care centres and their subsequent management. The data from this study of the network serve to highlight which conditions produce difficulties in clinical decision-making. Furthermore, it illustrates the impact of the meetings on the patient journey and why these cases need further discussion.
Areas of clinical concern
The cases discussed were those which gave particular concern to the treating consultant and their distribution reflects the paediatric workload (Fig. 2).
DDH was the most common condition discussed, with recurrent subluxation being the most common complication. Many of the cases discussed had presented beyond the at-risk screening programme. The outcomes for later operative intervention are known to be less favourable 22 and it is consistent that these gave the network the most concern.
In patients with Perthes’ disease, the majority of cases were discussed in the healed stage, with concerning radiographic features. In cases where there is concern regarding radiographic findings in asymptomatic children, the consensus was to observe. The rationale was that remodelling and physiotherapy would enable resolution of symptoms.
Fewer cases of malignant bone tumours were discussed than might be expected for this large population, because of the well-established principle of managing these in national network of bone tumour centres. The timely diagnosis and treatment of bone lesions is vital, 23 and after presentation to the network, one-third of these patients were promptly referred outside the South West region. The remaining patients with benign lesions did not need onward referral out of the region, because of the reassurance given by face-to-face discussion with senior colleagues. Thus, the network provides both confidence to the treating consultant and supports an appropriate and timely onward referral if required.
The incidence of paediatric fractures is approximately 20 per 1000 per annum 24 and complication rates can be high. 25 In 2012, we estimate that the hospitals within this network area treated 20 000 paediatric fractures annually. 26 Thus, while paediatric trauma is a significant workload, only 19 cases were discussed over the entire study period. The corrective effects of delayed healing and remodelling are well documented 27 and may account for this low rate of concern by the clinicians. The clinician's combined long-term experience of the benefit of waiting for remodelling is also reflected in the fact that realign-ment procedures were recommended to only five out of the 19 children. Our study suggests that local systems successfully manage the vast majority of post-traumatic complications.
Complications after paediatric bone and joint infection are not unusual and the difficult cases discussed reflect the literature. 28 The consensus opinion is helpful for planning surgery for late deformity secondary to growth arrest and avascular necrosis. The network was also particularly useful for clarifying atypical causes of infection-like conditions and advising on further imaging and biopsy. Subsequently, the multidisciplinary team environment facilitated referral to rheumatology colleagues. Similarly, ruling out an infection in the context of an inflammatory arthropathy can be challenging 28 and the support of a body of consultant opinion can be useful in preventing unnecessary diagnostic procedures.
Outcome of patient journey
Appropriate care delivered close to home and school is desirable for the paediatric population 29 and improvements in the delivery of local care maximises the use of clinicians’ time. 9 The network meetings enabled 14 face- to-face referrals to be made. However, after discussion in the group and advice given to the local consultant, 14.3% of those patients did not need to travel to the hub. Overall, approximately three-quarters of those children with complete follow-up available had their entire treatment locally, following reassurance or advice from the network meeting (Fig. 5). Five out of the 131 patients were advised by the group to see an out-of-region expert, thereby avoiding an unhelpful referral to the hub and expediting the referral pathway.
The outcomes of the cases have been audited to ensure good results are maintained 9 and to identify any concerns or areas for improvement. The results are discussed at subsequent meetings and thus the experience gained is shared through the network. Cases with poor outcomes did occur but were uncommon and ongoing cases, such as those who may require further procedures or network input, are re-discussed at subsequent meetings. Consequently, the network has reduced the burden of travel for patients, expedited their treatment and provided a mechanism for re-discussion of unresolved issues by a panel of experts.
Rationale for cases discussed with the network
Networks provide a means for communication between different healthcare providers and enable equitable access to services across geographical boundaries.9,20 The clinician benefits through reassurance, advice and education, 12 particularly in the context of high rates of litigation in orthopaedic surgery. 30
The consultant network can provide clinical reassurance to the treating consultant and the patient, reflected in the fact that reassurance of the management plan was the most frequent cause for discussion. The clinician's habit of lifelong learning requires insight into areas for improvement aided by discussion with colleagues 31 and we found a trend for consultants reaching a decade of experience to raise more cases for discussion. This might be explained by the progress of clinicians to a stage where they undertake more challenging cases. In addition, consultants with the most experience brought the majority of teaching cases, demonstrating the utility of the network in supporting the development of junior colleagues.
The activity of this network demonstrates the potential for a regular, scheduled mechanism to gain second opinions, re-assurance and enable direct referrals.
Limitations to the network
The network did not receive any specific funding and administrative costs were minimal. Nevertheless, consultants and healthcare professionals who attended were not able to carry out other duties and these costs should be considered. For example, each patient seen in an outpatient clinic costs £117. 32 However, lost productivity was minimised as most attendees did so in time set aside for continuing professional development.
Management of the cases which were discussed may have been delayed until the outcome of the meeting was known. However, this should be balanced against the benefit of the expert input given by the network. Additionally, the alternative would be to enter a waiting list for a referral to another consultant for a second opinion. Cases which required urgent management may therefore need discussion by another mechanism.
While various specialties were present at the meetings, few members of the wider multidisciplinary team attended. This may be as most discussions relate to potential operative intervention but wider participation could be beneficial to the debate.
There is a potential bias to cases presented, particularly for teaching, with those with successful outcomes being presented. Nevertheless, the network offered a confidential space to discuss difficulties.
Models of care continue to evolve and managed clinical networks are best suited to specialties with a wide range of rare conditions with potentially serious complications.
This paper describes an established clinical network in paediatric orthopaedics and highlights the potential benefits. The activity demonstrates the paediatric orthopaedic workload and areas contributing complex problems, with hip conditions contributing the most cases.
The patient journey has been streamlined as a consequence, with 74% of these challenging cases managed locally and a reduction in the number of onward referrals needed. It has enabled rapid referrals to national specialists or another specialty, thus reducing the time to treatment.
For the clinician, the network helped to confirm the management plan and provide reassurance. This is also beneficial in the context of potential litigation. Consultants around the tenth year of practice presented the most cases, which may reflect career progression for taking on more complex cases, while the most senior surgeons brought the most cases for teaching.
Future development will include the evolution of pathways of care through the network which will contribute towards service commissioning. We recommend the implementation of regional networks for paediatric orthopaedic services.
Footnotes
Acknowledgement
The authors would like to thank Georgia Antoniou for assistance with data entry and statistical analysis.
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
{kind=link}