
Abstract
Blockchain is gaining traction for improving the security of healthcare applications, however, it does not become a silver bullet as various security threats are observed in blockchain-based applications. Moreover, when performing the security risk management (SRM) of blockchain-based applications, there are conceptual ambiguities and semantic gaps that hinder from treating the security threats effectively. To address these issues, we present a blockchain-based healthcare security ontology (HealthOnt) that offers coherent and formal information models to treat security threats of traditional and blockchain-based applications. We evaluate the ontology by performing the SRM of a back-pain patient’s healthcare application case. The results show that HealthOnt can support the iterative process of SRM and can be continually updated when new security threats, vulnerabilities, or countermeasures emerge. In addition, the HealthOnt may assist in the modelling and analysis of real-world situations while addressing important security concerns from the perspective of stakeholders. This work can help blockchain developers, practitioners, and other associated stakeholders to develop secure blockchain-based healthcare applications in the early stages.
Introduction
Digitization in healthcare means generating massive electronic health records (EHRs), empowering patients as well as the whole healthcare sector (Narikimilli et al., 2020). Furthermore, healthcare organizations connect the internet of things (IoT) and smart devices with healthcare applications to allow real-time monitoring of patients’ health and decrease hospital visits for routine checks (Yaqoob et al., 2021). Using IoT and smart devices in healthcare also results in large amounts of data generation. Such advancements bring opportunities for making immediate and informed decisions by dint of having access to the extensive patient data (Yaqoob et al., 2021; Narikimilli et al., 2020).
EHR combines the health-related information of patients (e.g. medical conditions, diseases, health monitoring data), prescription, medication, medical analysis, personal information (e.g. name, age, gender, address), and financial information (e.g. insurance, billing details). Such medical data is confidential and indispensable, as well as plays an essential role in patients’ health diagnoses and treatments to reduce medical mistakes (Chen et al., 2019). The growing medical data heightens the concerns of securing it against various security threats, for example, data tampering, data theft, and counterfeit drugs (Radhakrishnan et al., 2019; Dagher et al., 2018). Blockchain technology is emerging in healthcare to address such security challenges, improve data integrity, and restructure the transaction process to be decentralized, transparent, and irreversible. For example, Saha et al. (2019) present the blockchain-based healthcare application (BBHA) along with cloud computing to protect medical data from tampering, theft, and unauthorized use.
Blockchain is a decentralized computing architecture that operates over a peer-to-peer (P2P) network and maintains transactions in the immutable ledger (Chen et al., 2018). The ledger contains a certain and verifiable record of every single transaction ever made (Saha et al., 2019). While blockchain technology is making inroads to such domains as finance, supply chain, and digital identities, the healthcare sector is leading the way (Narikimilli et al., 2020). The success of blockchain-based applications is contingent on accurate, verifiable, and untampered medical data.
Motivation
EHRs are one of the most valuable assets in healthcare applications. The current healthcare applications follow the traditional technology infrastructure where a centralized individual is responsible for maintaining the EHRs (Dagher et al., 2018). Therefore, the traditional healthcare applications (THAs) suffer from diverse security threats (Xu et al., 2019) that could negate the confidentiality, integrity, and availability of EHRs. Consequently, the tampered medical data can cause major issues during the patient’s treatment. Besides that, there are risks of unauthorized access, information disclosure, and various internal and external threats. Mansfield-Devine (2016), Dagher et al. (2018) investigated the security of THAs, and findings show that organizations do not adhere to best practices when designing and developing healthcare applications. Moreover, the technology infrastructure is incompatible and does not provide security measures by design.
Security is critical in the acceptability of healthcare applications. The first motivation of our research is to identify the security threats of THAs and present blockchain as a countermeasure solution to mitigate them. The second motivation is to uncover potential security threats in BBHAs. Moreover, we aim to reveal what countermeasures are available to mitigate these threats to secure BBHAs. The advent of blockchain technology has opened several research areas to preserve medical data, ensure data integrity, patient ownership of their data, easy exchange of medical data, and seamless medical insurance claims. However, there is conceptual ambiguity and semantic gaps because of varied interchangeable security concepts. Such a gap brings confusion about how to treat security threats effectively (Saha et al., 2019; Linn and Koo, 2016) in healthcare applications. This constraint inspired us to build an ontological representation of healthcare information security. The ontological representation can be a helpful tool for assessing and communicating the security aspects of healthcare applications, allowing for timely decisions to fix them.
Contributions
This work builds on the work presented in Iqbal and Matulevičius (2021b), in which we present blockchain-based healthcare security ontology (HealthOnt). HealthOnt demonstrates blockchain as a countermeasure solution to alleviate security threats of THAs. However, BBHAs do not become a silver bullet, and various security threats can appear (Iqbal and Matulevičius, 2019). Thus, we extended the HealthOnt with knowledge of BBHAs security threats. This work makes the following contributions:
A framework that explains the security threats that can appear in BBHAs;
Extension of HealthOnt by encoding the knowledge of BBHAs security threats.
Similar to our previous work, the above contributions rely on the security risk management (SRM) domain model (Dubois et al., 2010; Matulevičius, 2017). The domain model assists us in developing a framework for the security threats of BBHAs that contributed to the extension of HealthOnt. The HealthOnt can support the selection of blockchain when designing healthcare applications. There exist some comparable security models that address securing blockchain-based solutions (Arunkumar and Muppidi, 2019). However, such security models are either platform-specific or can not be updated upon appearing of new security threats. In contrast, HealthOnt encodes THAs’ and BBHAs’ information security into a dynamic ontology-based knowledge that can be extended, reused, and integrated with other security ontology representations.
The remainder of the paper is structured as follows: Section 2 overviews the blockchain, discusses the research method, related work, and back-pain patients’ healthcare application case. Section 3 presents the security threats that are mitigated in THAs through blockchain, and Section 4 discusses the security threats that can appear in BBHAs. Section 5 gives an overview of ontology development. Section 6 validates ontology, and Section 7 describes the emerging challenges in BBHAs. Section 8 concludes the paper.
Background
Blockchain
Blockchain is a decentralized, distributed, and immutable ledger technology (Ali et al., 2020). Blockchain creates a chain of blocks where a unique cryptographic hash links each block to the previous block. Blockchain eliminates trusted intermediaries from the transaction process, allowing for the development of transparent, yet secure applications (Rahmadika and Rhee, 2018) where network participants are managing the ledger blocks by themselves collaboratively. Blockchain networks can be classified as permissionless (e.g. Ethereum) or permissioned (e.g. Hyperledger Fabric (HLF)). A permissionless blockchain is fully decentralized and accessible to anyone who can join the network and participate in the consensus process (Junejo et al., 2020). Contrarily, a permissioned blockchain is partially decentralized with restrictions on who can join and access the operations. The designated authority establishes the structure of the blockchain network, as well as keeps control of various operations and processes (Jin et al., 2019).
Blockchain relies on the consensus mechanisms (e.g. Proof of Work (PoW), Proof of Stake (PoS), Practical Byzantine Fault Tolerance (PBFT)) to maintain the ledger state (Zhang and Lin, 2018). For example, Ethereum employs PoW, and HLF uses PBFT consensus. A smart contract in the blockchain is a piece of code that executes autonomously when certain conditions are met (Griggs et al., 2018). Smart contract eliminates trusted intermediaries, requires less human intervention, and reduces enforcement costs. Additionally, a smart contract prevents malicious or unintentional security threats (Jin et al., 2019) and enables decentralized distributed access control for resource authorization. Blockchain also provides provenance (Singh et al., 2021) to verify the record’s authenticity, while the ledger’s characteristic of tamper-evidence (Chukwu and Garg, 2020) allows to detect any interference or tampering with the content. Finally, blockchain provides pseudonymous characteristics (Iqbal and Matulevičius, 2021b). Such blockchain characteristics make blockchain an enticing technology in various application domains. These features support transparency, trust, and tamper resistance, which are key components in making business and transactional operations more secure, efficient, and effective.
Research Method
We utilize the systematic literature review (SLR) since it allows the systematic analysis to identify relevant literature and synthesize the results. We follow the SLR guidelines of Kitchenham and Charters (2007) and define five research questions, each covering a different aspect of the SRM domain model.
In this SLR, we use the primary search, backward and forward tracing techniques (Okoli, 2015; Fink, 2019) to collect the relevant studies. First, we performed a primary search based on search strings to identify an initial set of papers. Second, a secondary search was performed employing backward and forward tracing. We defined the search strings to gather literature studies that discuss the BBHAs and their security aspects.
Inclusion and exclusion criteria.
Inclusion and exclusion criteria.
We run these search strings on ACM Digital Library, IEEE Xplore, SpringerLink, ScienceDirect, Scopus, and Web of Science. We also included other non-academic research (e.g. gray literature). We applied exclusion (EC) and inclusion (IC) criteria to identify only the relevant papers (Table 1). For example, the papers that were duplicates, not in English, shorter than five pages, inaccessible (via university subscriptions or internet search), or published before 2008, were excluded (EC1 & EC2). We included the papers within the domain of blockchain and covering the security aspects of healthcare applications with blockchain (IC1), and providing blockchain-based countermeasures (IC2). To identify the security threats of BBHAs, we search for papers that discuss security threats of BBHAs (IC3) and countermeasures to mitigate them (IC4). The search resulted in approximately 1900 research papers from all the sources. First, we removed the duplicates and then performed several filtering iterations by considering the exclusion and inclusion criteria. A total of 90 papers remained that were subjected to full-text examination. After the full-text examination, a total of 39 studies remained that we used to conduct our research.
We utilize the SRM domain model (Dubois et al., 2010; Matulevičius, 2017) that helps to structure the security risk analysis of healthcare applications (Tables 3 and 4) that contributed in HealthOnt. Among other SRM approaches (Ganji et al., 2019), the SRM domain model fulfills the criteria of ISO/IEC 27001 standard and explores three aspects (e.g. assets-, risk-, and risk treatment-related) during the early phases of information system development. Based on the SRM domain model, the asset can be categorized as a system or business asset. The business asset has value, and the system asset supports it. Security criteria (confidentiality – C, integrity – I, and availability – A) distinguish business assets’ security needs and constraints. The risk constitutes the threat and one or more vulnerabilities. The threat targets the system asset and exploits the vulnerability. The vulnerability is connected to the system assets and depicts their weaknesses. Impact harms the business asset and negates the security criteria. The risk treatment implements the security requirements as countermeasures to improve the system security. Furthermore, we evaluate the ontology by performing the SRM of a back-pain patient’s healthcare application case.
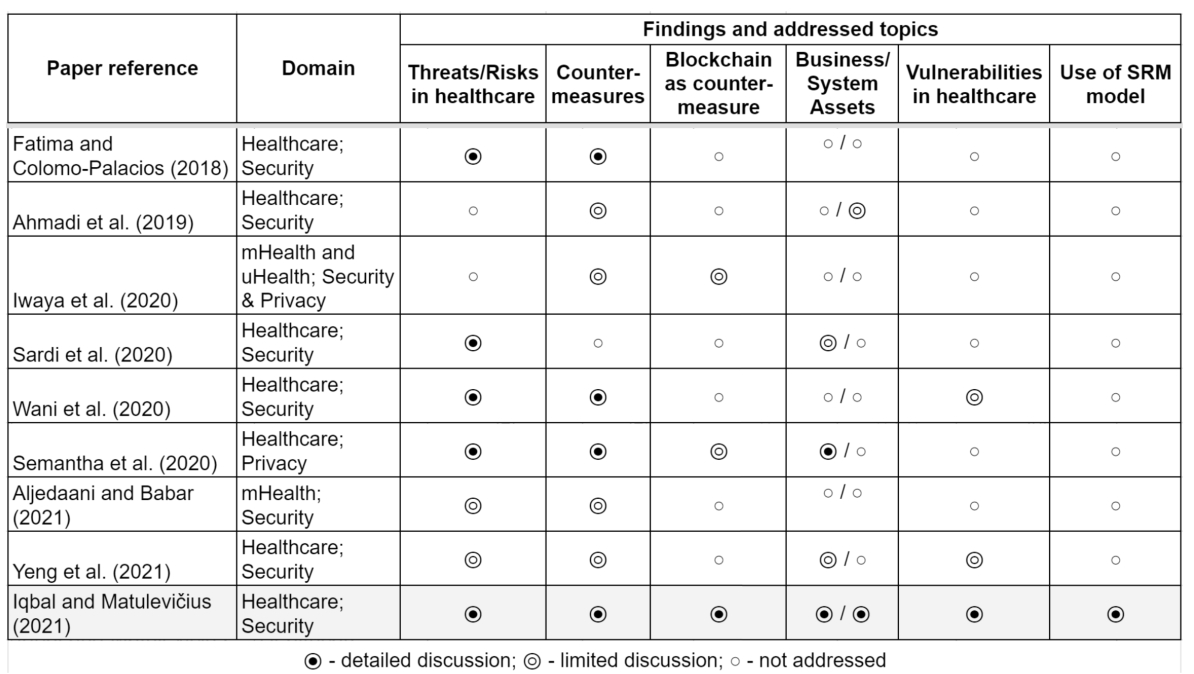
While healthcare applications are getting ubiquitous, researchers are working to improve the security and privacy of these applications to an acceptable level. However, a number of surveys and literature studies have only focused on the technical perspective of security threats in healthcare applications (Table 2). The studies neglected the business context and the impact of security threats on business assets, also not following the SRM domain model to describe the relationships of security threats with the system. Moreover, the THAs are not fully leveraging the benefits of emerging technology (e.g. blockchain).
Comparison of traditional healthcare applications.
Comparison of traditional healthcare applications.
For instance, Fatima and Colomo-Palacios (2018), Aljedaani and Babar (2021) review the common security threats and corresponding countermeasures considering only the technical side of the healthcare systems components. Similarly, Wani et al. (2020) investigated a few notable vulnerabilities in the hospitals connected to bring-your-own-device usage, the study reviewed the countermeasures to mitigate them. Still, they do not explicitly pinpoint the assets in the healthcare system targeted by the security threat and what business assets to protect. Sardi et al. (2020) explore the variety of existing security threats in healthcare facilities solely and briefly mention key assets. Still, they highlight the lack of risk assessment based on the specific needs of healthcare facilities and processes.
Some studies focus on controls to secure complex mobile, ubiquitous, and connected IoT healthcare systems. For example, Ahmadi et al. (2019), Iwaya et al. (2020) classified various countermeasures. However, they do not consider the context of such measures and do not describe how they can contribute to EHRs protection. At the same time, Yeng et al. (2021) present relatively complex security and privacy analysis of healthcare systems by investigating what assets to protect in healthcare, their vulnerabilities, and countermeasures. Table 2 illustrates that most of the literature reviews similar to our previous work (Iqbal and Matulevičius, 2021b) present a rather limited scope of analysis. Also, it is noteworthy that only a few studies mention blockchain technology as a countermeasure to THAs’ security threats. However, various organizations started working on BBHAs, for example, IBM-Blockchain (2022) is integrating blockchain in healthcare for better data sharing between healthcare providers without compromising data security, to overcome the drug counterfeiting (Martino et al., 2019), and so on.
In recent years,
Linn and Koo (2016) describe the fundamental principles of blockchain to address the security and privacy issues of THAs. The study also discusses the technical advantages of blockchain in healthcare (e.g. faster and easier interoperability). Randall et al. (2017) present the different use cases to address the security and interoperability challenges of THAs. Chukwu and Garg (2020) perform the SLR to explore the trust, security, and privacy constraints of traditional EHRs and how blockchain plays a role in overcoming them. The SLR of Agbo et al. (2019) investigates the security challenges, including how blockchain can protect medical data from potential data loss, corruption, or intentional security attacks. Jin et al. (2019) present blockchain in healthcare for secure and privacy-preserving medical data sharing. The study argues that blockchain’s tamper-evidence and decentralization features could help build a secure medical data-sharing network.
The related works explore various security aspects without addressing vulnerabilities, what assets to protect, blockchain characteristics, and not adhering to any SRM domain model. Furthermore, the related works do not address the security threats and vulnerabilities that may arise in BBHAs. In contrast, we use the SRM domain model to analyse and compile the security threats of THAs and BBHAs. We also investigated the countermeasures to minimize them. To ease the SRM of healthcare applications, we provide an SRM domain model-based ontological framework (HealthOnt) that offers a dynamic knowledge base of security threats of THAs and BBHAs, vulnerabilities, assets to protect, and countermeasures to mitigate the security threats of both THAs and BBHAs.
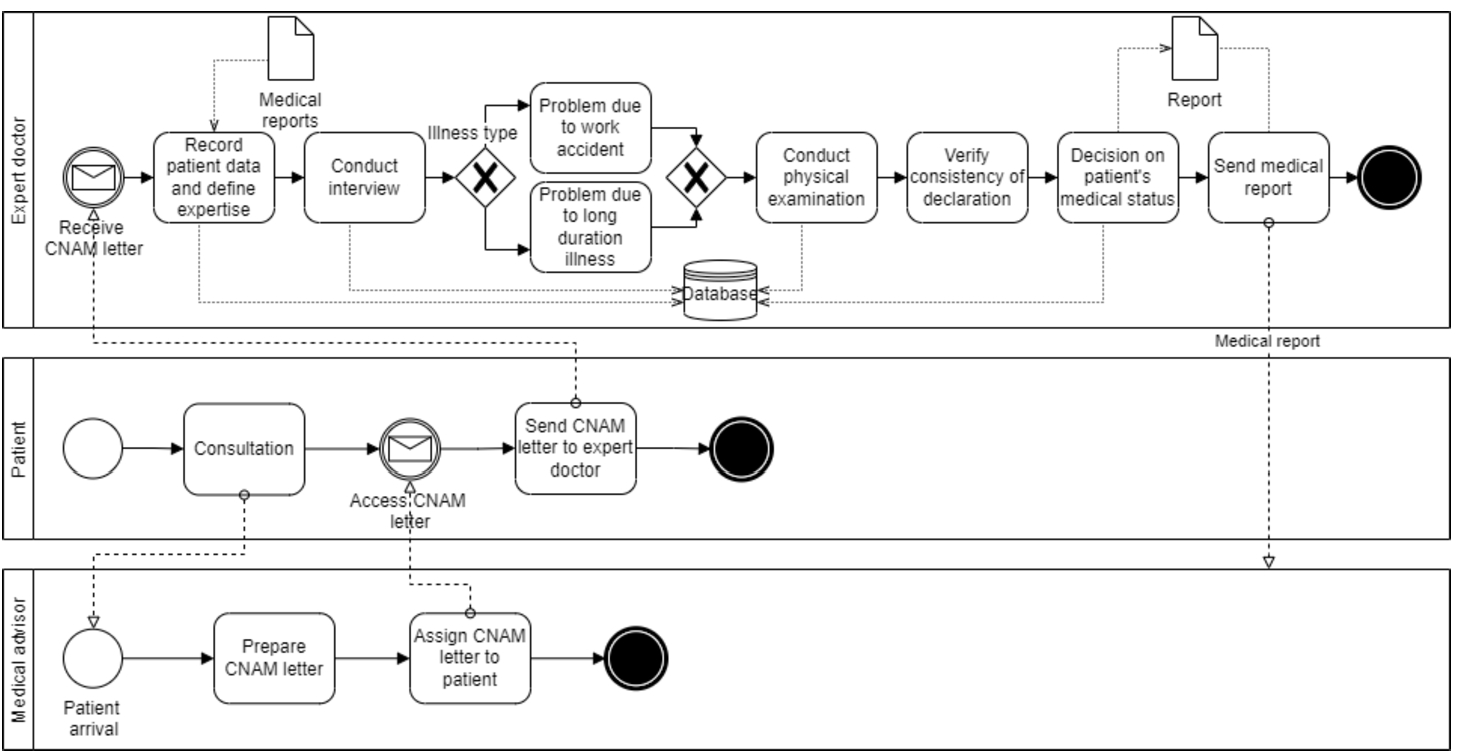
In this section, we discuss a case of the back-pain patients’ healthcare application that we used to evaluate the ontology. This application is operating at Farhat Hached University Hospital in Sousse, Tunisia to illustrate our proposal. The case scenario is shown in Fig. 1, where the main stakeholders are the medical advisor, patient, and expert doctor. The scenario starts when the patient contacts the medical advisor for consultation. After the appointment, the medical advisor prepares the CNAM letter1 (including questions to the expert doctor) and attaches the necessary medical reports. The patient is then in charge of delivering the CNAM letter and the medical reports to the expert doctor. The expert doctor registers the patient’s data and collects additional information during the interview in order to define illness type (e.g. work accident or long-duration illness). For example, during the interview, the expert doctor collects whether the patient suffers from low back-pain, the type of sciatica, whether the patient is diabetic, and also asks for the personal information (e.g. marital status, number of children, and the last job type). Thereafter, the expert doctor identifies the illness and studies the necessary documents related to either the work accident or the long-term illness.
Case of back-pain patients’ healthcare application.
Next, the expert doctor performs the patient’s physical examination and records results (e.g. weight, height, build, limp, and gait). During the physical examination, the expert doctor can check and verify the consistency of the claim. Then, the expert doctor writes a conclusion based on the gathered data (e.g. on the patient’s details, interview, and the physical examination outcomes). The expert doctor writes a medical report and sends it to the medical advisor. This report includes the conclusion about the patient’s medical status and guides the medical advisor regarding the decision (e.g. whether the medical leave is needed, what is the duration of the medical leave, and when the patient could return to work). We will consider this back-pain patients’ healthcare application case to illustrate the security threats and how they can be mitigated using blockchain technology.
In our previous work (Iqbal and Matulevičius, 2021b), we examine the literature studies that describe how blockchain can alleviate the security threats of THAs. We developed a framework (Table 3) using the SRM domain model and discussed the five security threats (e.g. data tampering, data theft, medical records mishandling, counterfeit drugs, and man in the middle) of THAs in detail. In this work, we provide the summary of those threats and other threats (e.g. single-point failure, repudiation, insurance fraud, clinical trial fraud, tampering device settings, social engineering) we discuss in detail. The framework describes THAs’ security threats, vulnerabilities, assets to protect, blockchain-based countermeasures, and blockchain features that correspond to each countermeasure.
Data Tampering
THAs lack control over patients’ data security (Xu et al., 2019), which is a major concern for healthcare organizations. Blockchain provides various controls by design that can mitigate this threat. For example, smart contract-based distributed access control (Maesa et al., 2017) regulates the users’ access to stored medical data. Strong cryptographic primitives (Esposito et al., 2018) help to build fine-grained access control. In a blockchain, the records are difficult to modify and delete due to the ledger redundancy and append-only structure (Dagher et al., 2018). PoW consensus verifies transaction and data validation without a third party (Hussein et al., 2018). Also, using the SHA-256 hashing, blockchain computes a unique hash id of original data to verify the authenticity of data (Han et al., 2018). HLF uses trusted authorized nodes to verify and validate the authenticity of data (Chen et al., 2018). Blockchain is tamper-evident (Han et al., 2018) and thus detects any unauthorized modifications. Blockchain builds robust audit trails in an immutable ledger by keeping a record of each performed action (Bhuiyan et al., 2018).
Data Theft
EHRs include confidential information that is attractive to cybercriminals that exploit various vulnerabilities in THAs to steal EHRs. In contrast, BBHAs are resistant to data theft. Blockchain works over a P2P network where nodes behave both as a server and client to send and receive data directly. This mechanism helps to protect the data leakage to unauthorized users (Chen et al., 2018). Dagher et al. (2018) used the voting process (e.g. QuorumChain algorithm) to determine which nodes are allowed to access certain types of data. The permissioned blockchains define permission settings to restrict unauthorized data access (Han et al., 2018). The strong cryptographic primitives (Esposito et al., 2018) and smart contract-based distributed access control (Hussein et al., 2018) allow only authorized users to access medical data. The ancile framework (Dagher et al., 2018) uses the proxy re-encryption to store hashes of data on-chain and off-chain. In addition, Esposito et al. (2018) suggests data obfuscation to protect data on-chain and off-chain.
Framework that presents security risk analysis of traditional healthcare applications.
Framework that presents security risk analysis of traditional healthcare applications.
Healthcare institutions must guarantee that medical records are kept confidential and secure. In THAs, the medical institutions control and manage the patient’s medical data where the non-relevant individuals can access it. BBHAs enable permission settings and distributed access control to handle patients’ medical data (Yaqoob et al., 2021). Also, blockchain performs data validation before saving on the ledger during the consensus process. For example, blockchain defines data validation rules which are agreed upon by other network nodes (Dexter, 2018). Thus, all the nodes follow those rules to validate the data and discard all the unauthorized changes (Shi et al., 2020).
Counterfeit Drugs (Fake Medicine)
The creation and distribution of counterfeit pharmaceuticals is a global problem with significant health and economic consequences, primarily for consumers (Martino et al., 2019). According to Yaqoob et al. (2021), 10–30% (worth $200 billion) of drugs sold worldwide each year are counterfeit, posing significant health risks. Blockchain offers a solution to enable pharmaceutical traceability, real-time access to data, and supply chain validation by creating a log to track each step (Narikimilli et al., 2020; Yaqoob et al., 2021; Martino et al., 2019). For example, IBM Research uses blockchain to reduce or eliminate the drug counterfeiting problems in Kenya (Martino et al., 2019) by using immutable and traceable logs at each stage of the pharmaceutical supply chain.
Man in the Middle (MitM) Attack
According to SpecOpsSoft (2020), MitM attacks are rising in healthcare applications to gain or manipulate sensitive information. Xu et al. (2019) introduce the blockchain-based distributed interplanetary file system (IPFS) for storage to establish a secure communication channel. Blockchain works on a P2P network that makes it hard for an attacker to intercept the communication, data analysis, or sniffing (Chen et al., 2018). Blockchain maintains pseudo-anonymity, for example, the patients and their medical data are linked with a cryptographic hash. Also, the data processing in a blockchain is anonymous (Yaqoob et al., 2021) that hides the actual identity from patients’ medical data (Ali et al., 2020).
Single Point Failure
Like any other system, the attacker can find faults in the system’s design, implementation, or centralized dependency components to disrupt the healthcare services.
Repudiation
The patient’s medical data is sensitive and life-critical. The healthcare system should trace all actions performed (intentionally or unintentionally) by the authorized users on a patient’s medical data and easily identify how it was performed.
Insurance Fraud
Healthcare insurance frauds are increasing, which involves the filing of dishonest healthcare claims. For example, the value of challenged healthcare claims surged from $11 billion to $54 billion annually (Narikimilli et al., 2020).
Clinical Trial Fraud
Reproducible data is the lifeblood of advanced research across the globe. Currently, the healthcare institutions and research groups suffering from clinical trial frauds (George and Buyse, 2015) and medical decisions made by researchers on the premise of fraudulent data could leave patients at risk.
Tampering Device Settings
Medical devices connected to the internet and the internet of things (IoT) enable healthcare professionals to be more watchful and connected with the patients. Progressively, IoTs are becoming the heart of digital healthcare, but new security challenges are appearing.
Social Engineering
According to HelpNetSecurity (2019), only 1% of cyber-attacks in the year 2019 were exploited due to hardware or software vulnerabilities, and 99% of cyber-attacks utilized some form of human intervention (e.g. phishing, fake identity, honey trap, etc).
The security risk analysis of traditional healthcare applications shows that blockchain can help the healthcare sector to overcome the security threats of traditional technology infrastructure for preserving the medical data, data integrity, and patient ownership of their data. We use the constructs of the SRM domain model that fulfills the criteria of ISO/IEC 27001 standard (Ganji et al., 2019) for defining the scope of our work and to assist in building a framework for structuring the security risk analysis of traditional and blockchain-based healthcare applications. This framework (Table 3) presents blockchain as a countermeasure solution for mitigating the security threats of THAs. Blockchain provides technology infrastructure with unique characteristics for building healthcare applications. For example, blockchain operates over a P2P network, uses consensus mechanism and cryptography, is immutable, decentralized, tamper-evident, and provides permission settings, provenance, and pseudo-anonymity. However, we cannot deny the security aspects of BBHAs because in recent years various security threats have appeared in blockchain-based solutions. Hence, we discuss such security threats in the next section.
Security Threats Appeared
We analyse the literature studies that describe security threats to BBHAs. We identify those security threats and categorize them using the SRM domain model and develop a framework (Table 4). The framework illustrates the BBHAs’ security threats, vulnerabilities, assets to protect, countermeasures, and corresponding countermeasure strategies. In this section, we discuss the security threats in detail.
Sybil Attack
Sybil attack is a P2P network attack (Douceur, 2002) where the attacker creates numerous fake identities and connects with victim nodes to isolate them from other honest nodes.
Framework that presents security risk analysis of blockchain-based healthcare applications.
Framework that presents security risk analysis of blockchain-based healthcare applications.
The double-spending is categorized under data consistency attack (Nicolas et al., 2021) to spend the same transaction twice (Pérez-Solà et al., 2019). Similarly, in BBHAs, the attacker can change the transaction state and spend the same transaction twice.
Eclipse Attack
In an eclipse attack, the attacker takes control of all the neighbuoring peers of the victim node and hides the correct ledger from the victim node (Rahmadika and Rhee, 2018).
Smart Contracts Attacks
The security of smart contracts has become a major concern in recent years (Singh et al., 2021) as a result of different security issues originating in blockchain-based applications from the execution of smart contracts.
Block Withholding Delay
In PoW-based blockchains, a block withholding delay is common. The attacker miner joins a victim mining pool and refuses to submit blocks on time (Liu et al., 2019).
Sybil-Based DoS
Blockchain-based applications operate over a P2P network. Despite being operated on a P2P network, they are still vulnerable to DoS attacks (Guru et al., 2021).
Deanonymization Attack
Anonymization is a characteristic of blockchains that refers to hiding an identity, but still possible to link a user or company behind each transaction (Quintyne-Collins, 2019).
Quantum Computing Threats
Quantum computing research is advancing, and many cryptographic protocols in use currently are vulnerable to quantum computing (Shankland, 2021). Blockchain platforms rely on cryptographic protocols that are also vulnerable to quantum computing.
Endpoint Vulnerability
The easy way of attacking technology solutions is through endpoint vulnerabilities, which occur where humans and technology interact (Velissarios et al., 2019). Hence, the protection of endpoints is paramount in BBHAs (Velissarios et al., 2019).
Other Security Threats
In this section, we outline numerous possible security threats of blockchain systems (Table 5) that have yet to be studied in BBHAs but may appear. Therefore, blockchain developers and practitioners should be aware of these security threats.
Security threats not yet investigated in blockchain-based healthcare applications but may appear.
Security threats not yet investigated in blockchain-based healthcare applications but may appear.
We build this framework (Table 4) aiming to provide the details about the security threats that may appear in BBHAs, and the controls to mitigate them. Both frameworks (Tables 3 and 4) complement one another in the context of the SRM constructs we used. However, the aforementioned frameworks represent the knowledge base in a static manner and are difficult to update when new security threats, vulnerabilities, or countermeasures appear. To overcome these issues, we build a blockchain-based healthcare security ontology, HealthOnt, where these frameworks serve as a foundation.
Ontology is a collection of concepts and their relationships (Herzog et al., 2007). To avoid the repercussions of a misunderstanding, ontology elaborates the meaning of concepts within a domain (Kang and Liang, 2013). In the security domain, ontology is frequently used to systematically classify security risks, preventative measures, and associated security implementation technologies (Kang and Liang, 2013). Furthermore, the Noy and McGuinness (2001) illustrate the reasons that motivate the development of an ontology. For instance, ontology makes it possible to i) share a common understanding, ii) reuse of domain knowledge, iii) make domain assumptions explicit, iv) separate domain and operational knowledge, and v) analyse domain knowledge. As a result, we present HealthOnt2 which is available online3 and encapsulates security threats of THAs and BBHAs.
HealthOnt is based on web ontology language (OWL) and WWW Consortium (W3C). OWL is a semantic web language based on description logic (DL) to illustrate rich and complex knowledge about things (e.g. concepts), groups of things, and their relations. OWL supports a resource descriptive framework (RDF) to define a metadata model to build a readable semantic infrastructure (Hector and Boris, 2020). RDF supports triplet format (e.g. subject-predicate-object) for describing the ontology concepts. For example, in this triplet (DataTampering
We utilize the ontology construction method (Uschold and Gruninger, 1996) and this approach has also been applied in Iqbal and Matulevičius (2020) to build an ontology for security threats of Corda-based financial applications. We start the ontology building process by identifying its purpose and scope. Second, we collect the domain information (e.g. concepts and relations) and categorize it in the frameworks (Tables 3 and 4). This process refines the concepts and improves the technical domain language related to assets, security criteria, threats, vulnerabilities, and countermeasures. Thereby, the frameworks provide a coherent structure and required level of understanding for a successful implementation of HealthOnt. Third, we used Protege4 to formalize the domain knowledge in our ontology by coding the concepts and relations. Our previous work (Iqbal and Matulevičius, 2021b) presents the details related to the ontology construction.
Ontology Validation
Ontology validation is important to ensure the correctness of ontology, the meaning of ontological reasoning, and the effective use of an ontology (Steiner and Albert, 2017). In (Iqbal and Matulevičius, 2021b), we use the qualitative assessment criteria (Raad and Cruz, 2015) to validate the HealthOnt. This approach helps in the early phases to check whether the coded concepts model the real-world domain for which the ontology is built. The qualitative assessment criteria contribute to the quality of ontology, but it does not address how good the developed ontology is? To answer this question, we use a back-pain patient’s healthcare journey to map the coded knowledge of healthcare security.
Analysis of the Back-Pain Patients’ Healthcare Application Case
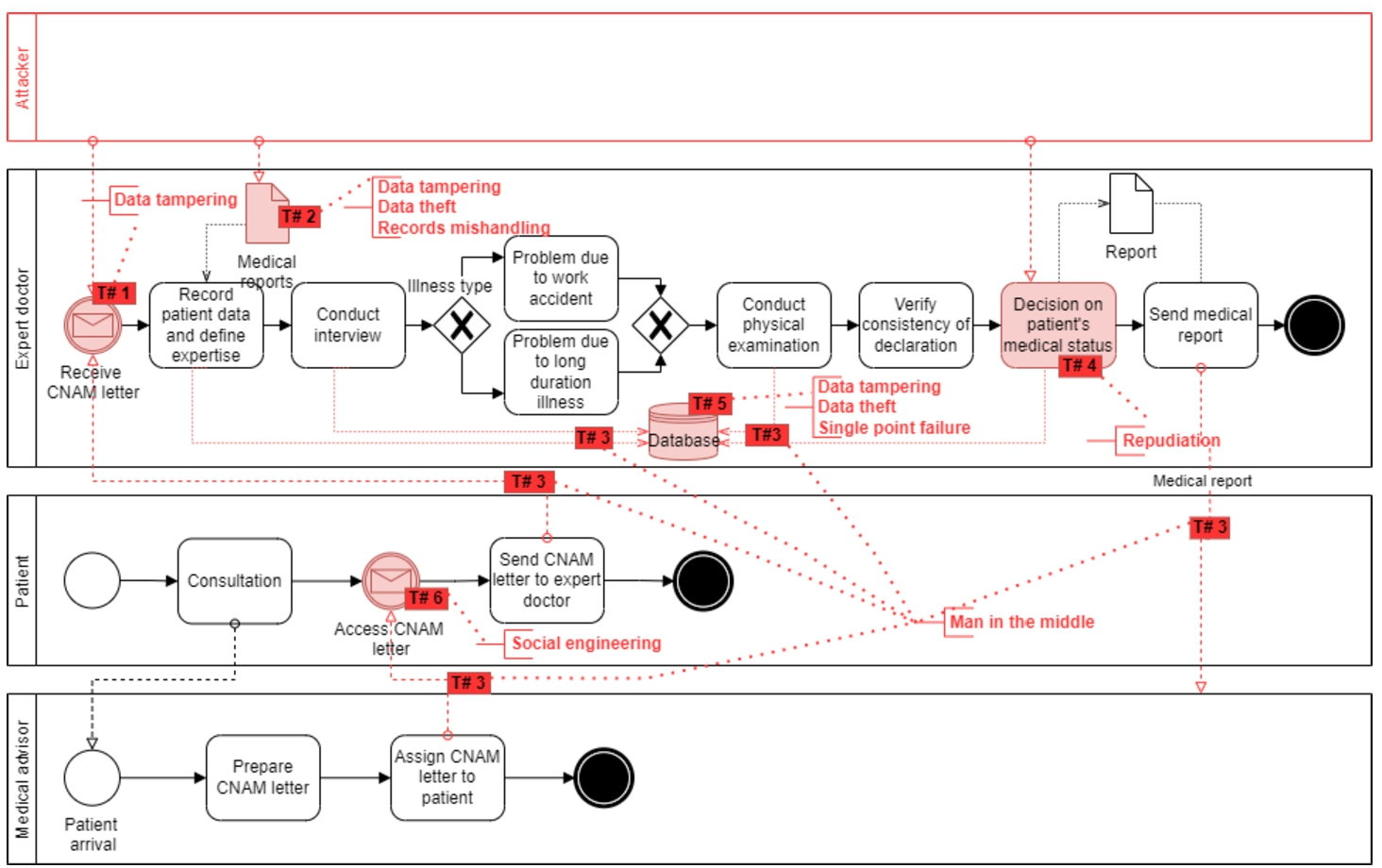
We use HealthOnt to map the healthcare applications’ security knowledge on a back-pain patients’ healthcare application (BPPHA), described in Section 2.4. HealthOnt helps to identify the security threats of it that are highlighted as threat points in Fig. 2.
Mapping of security threats that can appear in traditional BPPHA using HealthOnt.
We present blockchain as a countermeasure solution (Fig. 3) to illustrate the blockchain-based BPPHA that implements various security controls by design and mitigates security threats of traditional BPPHA. For example, the blockchain-based role-based access control (RBAC) can restrict access to the CNAM letter. Blockchain provides a consensus mechanism to verify and validate the CNAM letter transaction without requiring a third party, a unique hash id of the original CNAM letter stored in the blockchain to verify its authenticity, and an immutable ledger to keep track of each performed action. Similarly, medical reports can be protected against data tampering using RBAC and blockchain-based controls to verify and validate the authenticity of medical reports. The use of RBAC and cryptography (e.g. to store only encrypted medical reports on-chain and off-chain) overcome data theft. Also, the permission settings and access control enable patients to control their medical reports, and the tamper-resistant environment of blockchain guarantees the authenticity of medical reports.

Blockchain as a countermeasure solution to mitigate security threats of traditional BPPHA.
Blockchain-based BPPHA works on a P2P-based distributed network to exchange data (e.g. CNAM letter, medical reports, medical records). It makes it hard for an attacker to intercept the communication, data analysis, or sniffing. Blockchain enables pseudo-anonymity because the patients and their medical data are linked with an anonymous public address. Blockchain-based BPPHA has an immutable ledger that keeps immutable logs to track who and when the particular operation (intentional or unintentional) was performed. Thus, overcoming the repudiation threat. Medical records and healthcare database can be protected against data tampering by using decentralized access control and blockchain controls to verify and validate the authenticity of medical records and healthcare databases. Decentralized access control and cryptography overcome the threat of data theft. Moreover, blockchain is decentralized, operates over a P2P network, and does not rely on a single or central point server and service. Thus, it is resilient to a single-point failure. Blockchain-based BPPHA employs RBAC to guarantee that only relevant people have access to specific information, and unauthorized users cannot access it.
Blockchain technology is advancing in the healthcare domain, and along with the security issues, it is also facing scalability, privacy, and regulatory challenges.
Various solutions are explored to overcome scalability issues (e.g. permissioned blockchains, lighting protocol, sharding, delegated proof of stake, directed acyclic graph) (Singh et al., 2021). These techniques can help to increase the volume of transactions, although more work is needed in this direction.
To overcome privacy challenges, different privacy-preserving proposals (e.g. secure multi-party computation, zero-knowledge proof, homomorphic encryption, ring signatures, transaction mixers) (Bernal Bernabe et al., 2019) and blockchain platforms (such as Enigma, Zcash, Monero) (Khan and Nassar, 2019) are advancing to preserve the privacy of confidential information. These solutions primarily address overall transaction privacy in cryptocurrency-based blockchain platforms. Therefore, more research is required in the area of privacy-preserving blockchains for healthcare applications.
Many organizations are collaborating on regulatory guidance (such as a legal framework for data storage and sharing over blockchains) (Yaqoob et al., 2021). However, more research is needed to standardize blockchains for healthcare applications.
Concluding Remarks
Footnotes
Caisse Nationale d’Assurance Maladie (French) – National Health Insurance Fund.