
Abstract
Concomitant management of synchronous abdominal aortic aneurysm (AAA) and colorectal cancer (CRC) is mandatory in cases in which both entities are life threatening for the patient. The endovascular aneurysm repair (EVAR) method can contribute toward concomitant management by offering the avoidance of an otherwise threatening vascular graft infection. We present a case of a complicating CRC and a synchronous AAA, which were successfully treated at the same hospitalization. The AAA was treated first by EVAR, and the colon resection followed 3 days later. The patient's postoperative course was uneventful. EVAR, if the standard criteria are met, could comprise an alternative and reliable solution for treating concomitant AAA and CRC even in the acute setting.
The occurrence of concomitant abdominal aortic aneurysm (AAA) and colorectal cancer (CRC) is a rare medical entity, which is followed by controversy about the optimal treatment. 1–4 Morris and Da Silva, reviewing the literature, proposed that the treatment priority lies with the life-threatening lesion. 5 But what happens when both lesions can have an immediate negative impact on the patient's health? Such cases include the presence of an AAA > 5.5 cm and a synchronous obstructing or perforating CRC. Velanovich and Andersen indicated that in this case, one-stage treatment may be necessary to avoid the risk of postoperative AAA rupture and to manage the urgent situation of a complicated tumor. 6 Unfortunately, the concomitant treatment, although tempting, has the theoretic risk of vascular graft infection. An alternative solution could be provided by the evolving method of the endovascular aneurysm repair (EVAR). The latter, except for the good functioning results achieved so far, 7,8 also holds the advantage of not interfering with the bowel resection. Thereafter, EVAR might overcome the treatment obstacles in this challenging group of patients.
We report a case of concomitant infrarenal AAA of 6.5 cm in diameter and obstructing CRC located at the splenic flexure of the colon, which has been successfully treated by EVAR and subsequent laparotomy for colon resection.
Case Report
A 79-year-old female was referred to the University Hospital of Ioannina from a district hospital for vascular assessment and treatment. The first assessment of the patient was carried out at the district hospital, where she was diagnosed with a synchronous AAA and obstructing CRC (Figure 1). The patient's complaints were of progressing abdominal distention, diffuse abdominal pain, and constipation lasting approximately 20 days. Her medical history consisted of arterial hypertension, coronary artery disease, asthma, deep venous thrombosis of the right lower limb, and cholecystectomy. The abdominal computed tomographic (CT) scan revealed the presence of a tumor located at the splenic flexure of the colon, which was nearly obstructing the bowel lumen and also had signs of inflammation around it (Figure 2A). No liver metastases were noted. In addition, an infrarenal aortic aneurysm was found, sized 6.5 cm in diameter and not involving the iliac arteries (Figure 2B). After admission, the patient underwent colonoscopy, which confirmed the CT scan findings. The endoscopic biopsies showed the colon infiltration by a poorly differentiated adenocarcinoma.

Plain abdominal radiograph: the transverse colon is gaseous and distended, with a cutoff sign at the left upper quadrant (thick arrow). There is also visible calcification of the abdominal aortic aneurysm wall (thin arrows).
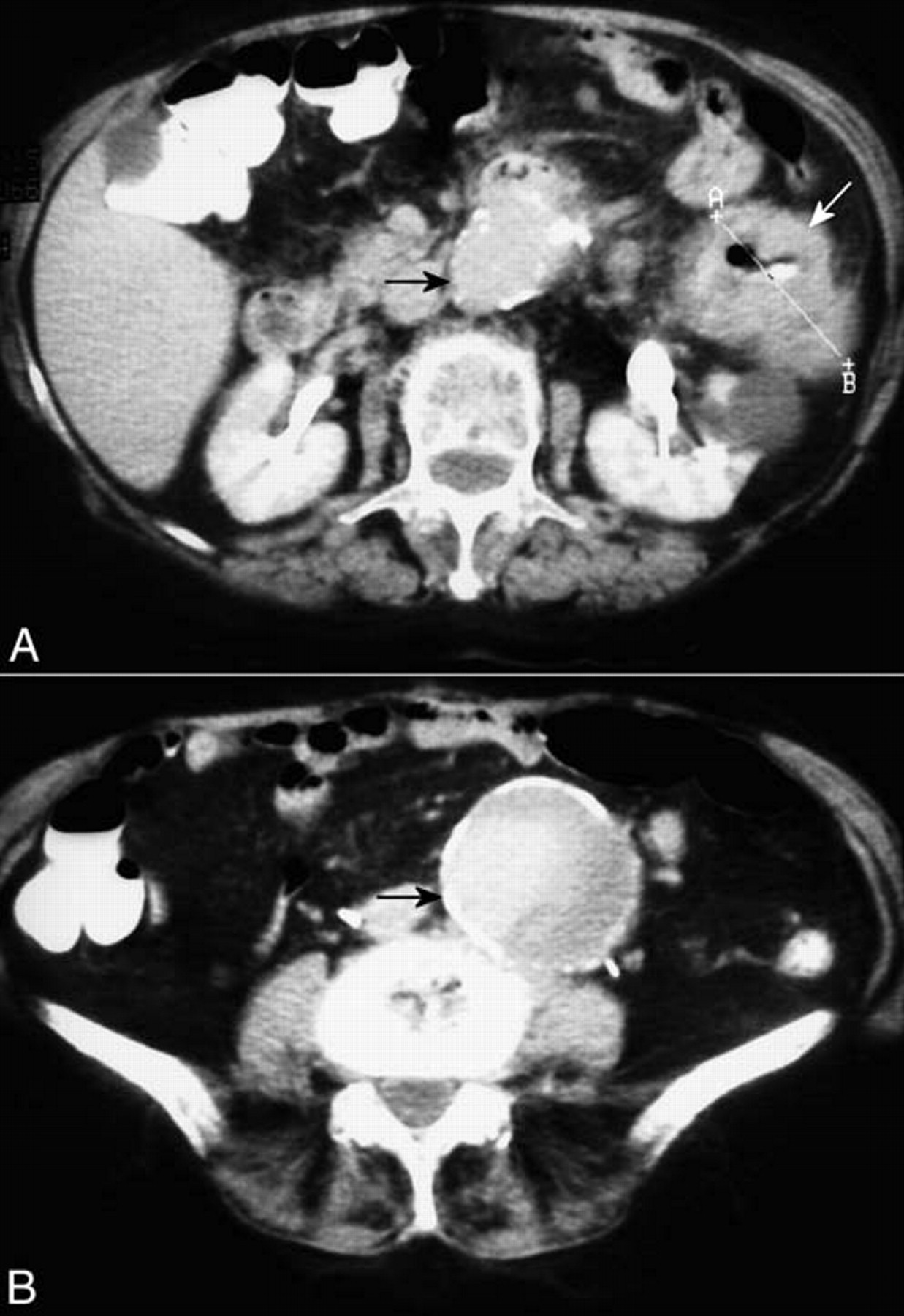
Preoperative abdominal computed tomographic scan. A, Thickening of the bowel wall with narrowing of the lumen near the splenic flexure of the colon (white arrow) and the origin of the aneurysm in the infrarenal aorta (black arrow). B, The abdominal aortic aneurysm in its largest transversal diameter (black arrow).
The advanced complicated malignant disease and the medical history of the patient led to the decision to treat both entities during the same hospitalization and with the most minimally invasive treatment. The AAA characteristics were in favor of using an endovascular graft in terms of an existing proximal neck of about 15 mm, without severe angulation, and a good distal landing zone on both common iliac arteries. The AAA repair was performed first. Under spinal anesthesia and prophylactic antibiotic therapy for both aerobic and anaerobic microbes, an aortoiliac bifurcated endovascular stent graft (Talent, Medtronic AVE, Medtronic Europe S.A., Route du Molliau, Switzerland), with a 28 mm proximal and a 16 mm distal diameter, was deployed through bilateral femoral arteriotomies. The completion aortogram confirmed a well-positioned and functioning endograft without evidence of endoleak. The total procedure was completed in 2 hours. After an uneventful 3-day recovery period and good bowel preparation, the patient underwent an extended left hemicolectomy under general anesthesia. The pathologic examination of the surgical specimen showed a poorly differentiated T3N2 tumor.
The patient had an uneventful recovery, and the functional outcome of both procedures was excellent. She was discharged from hospital on the eighth postoperative day from colon resection, with reference to the outpatient clinics of the Oncology Department. Unfortunately, the survival of the patient was affected by early cancer recurrence. At 3 months, she underwent CT of the abdomen according to our post-EVAR follow-up protocol, in which an excellent functional vascular result without any evidence of endoleak was revealed (Figure 3). On the other hand, diffuse lymphatic dissemination was seen in the abdomen and especially around the aorta (see Figure 3). After that, she had a rapid deterioration and died of disseminated disease 1 month later.
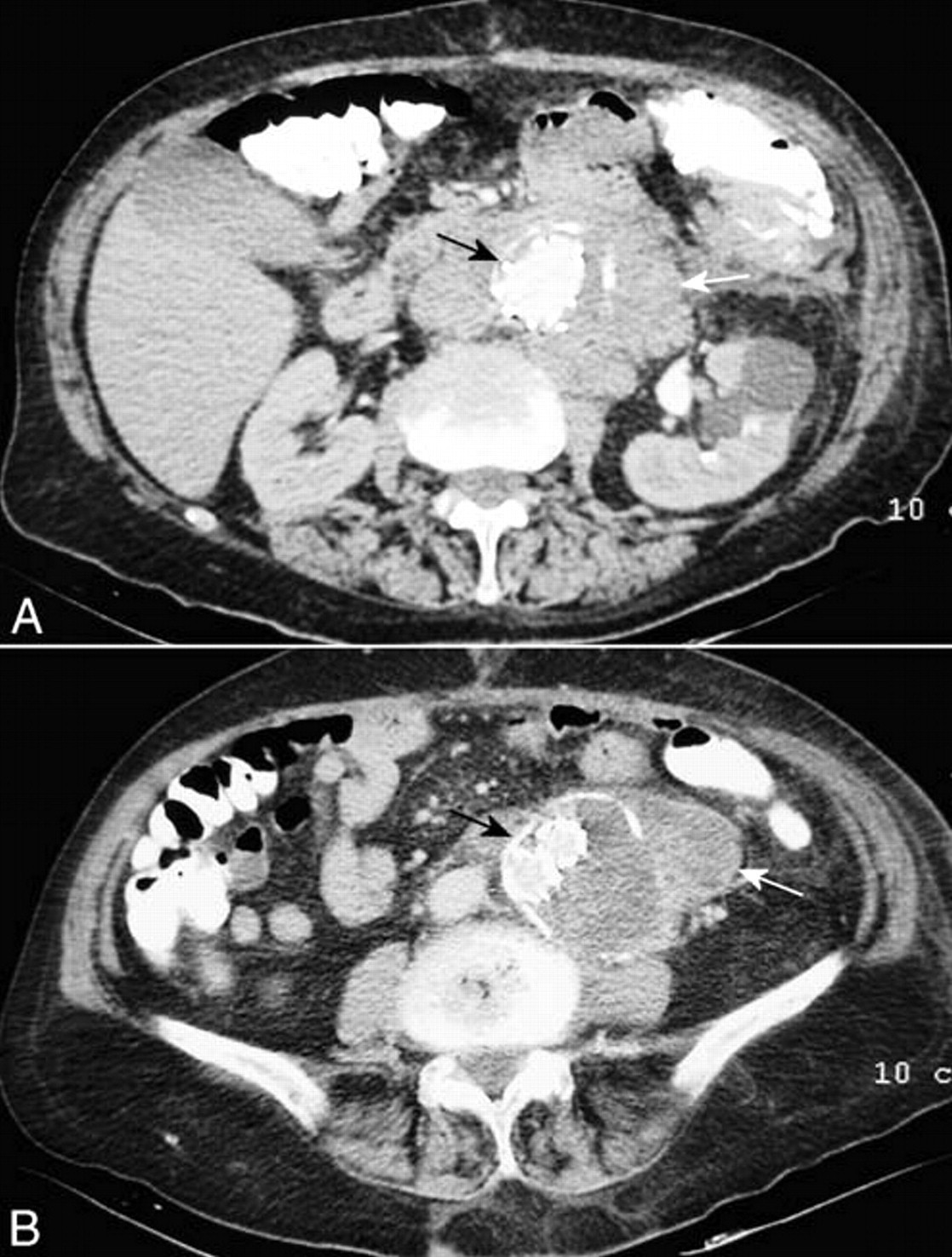
A and B, Follow-up abdominal computed tomographic scan 3 months postoperatively. Good position and function of the aortic stent graft (black arrow), with no evidence of endoleak inside the aneurysm sack. The presence of bulky para-aortic lymph nodes is also noted (white arrow).
Discussion
The incidence of coexisting AAA and malignant disease is reported to range from 4 to12.6%. 3 The best way to treat this patient group remains under consideration, mainly because of a lack of prospective randomized studies. The dilemma is even greater when the concomitant malignancy originates from the gastrointestinal tract. The most challenging cases, which are fortunately uncommon (< 3.5%), are those of CRC coexisting with AAA. 5
During the past 40 years, a controversy has existed in the treatment strategy between one- and two-stage procedures. The main arguments against the two-stage procedure are the risk of either AAA rupture in the postoperative period (10–47%), when the malignancy is treated first, or considerable delay in the management of the malignant disease in the opposite case. 4,9–12 Conversely, in the one-stage procedure, the operation becomes more severe, and there is always the possibility of aortic graft infection, with its deleterious effects on the patient's health or even life. 13 Indeed, the highly contaminated bowel content makes the one-stage procedure more prone to aortic graft infection, even though there is no evidence to support this so far. 5,14 In reviewing this problem, in 1965, Szilagyi and colleagues recommended that the symptomatic lesion should be treated first. In the asymptomatic population, the AAA takes priority when it is large and the CRC when the AAA is small. 1 Two decades later, Lobbato and colleagues questioned 43 professors of general and vascular surgery on their treatment preference concerning concomitant AAA and CRC. 15 The majority answered that they would treat the symptomatic lesion first. Only two stated that they would perform simultaneous procedures but under the condition that both lesions were asymptomatic. In 1985, Velanovich and Andersen concluded that when an AAA exceeds 5 cm in diameter and coexists with a complicated CRC, the one-stage procedure should be considered, provided that the operative mortality rate is estimated to be < 10%. 6 In summary, the current proposed treatment is the two-stage procedure, with priority given to the most life-threatening lesion (AAA > 5 cm or complicated CRC), and the one-stage procedure when both lesions are symptomatic and/or equally dangerous to the patient. 5,11
The evolving method of EVAR in the treatment of AAA has shown good results in carefully selected patients. EVAR demonstrates the following potential advantages: placement under regional anesthesia, avoidance of arterial cross-clamping, minor operative trauma, reduced blood loss, and reduced length of intensive care unit and hospital stay. 16,17 The avoidance of laparotomy and interference with bowel contents makes EVAR an excellent solution for patients with concomitant AAA and CRC. Of course, not all AAAs are suitable for EVAR, and it has been estimated that about 60% of them could be treated with this particular technique, whereas the larger ones usually have a more adverse morphology. 17 Reviewing the literature, we found four reports of EVAR in nine patients with malignancies. 18–21 Only in three reports (five patients), the concomitant malignancy had a colorectal origin. 19–21 In the first study, the patient was diagnosed with a 5.7 cm AAA and a rectal T2N0 tumor. He was treated by EVAR and local excision of the tumor owing to the patient's refusal of laparotomy. 19 The second study includes two patients with AAAs of 3.4 and 6.5 cm in diameter and a sigmoid and rectal cancer (T3N0), respectively, which were treated by EVAR and following bowel resection. 20 The third study (two patients) refers to a complication of aortic endograft (limb occlusion) followed by lithotomy position for rectal anterior resection. 21 None of the above patients had an indication for urgent intervention regarding the CRC.
In this case report, we confronted two diseases, a 6.5 cm AAA and a complicated CRC causing obstruction. Both lesions had the same priority index: a high risk of rupture of the AAA and a symptomatic tumor, which could not be referred for the staging approach. The preexisting comorbidities, along with the status of the patient and the favorable characteristics of the AAA, made her a possible candidate for a two-stage procedure with EVAR followed soon by laparotomy. Both diseases were managed successfully, although the aggressive nature of the tumor did not allow the long-term survival of the patient. To our knowledge, this is the first successful treatment of concomitant symptomatic CRC and large AAA by EVAR. The dilemma of appropriate therapy with special consideration to the risk of prosthetic aortic graft infection seems to have an alternative solution. If the standard criteria are met, EVAR provides the safest and most reliable approach for the demanding surgical situation of the coexistence of an AAA and a CRC.