
Abstract
Poor rehabilitation rates and the high-cost of managing postamputation patients justify an aggressive revascularization policy in critical lower limb ischemia. Endovascular therapy is our first choice for limb salvage in these patients. However there are patients for whom endovascular therapy is not feasible. When bypass is necessary, autologous vein is a superior conduit to synthetic material. However, varicosities usually contraindicate autologous vein bypass because of the risk of aneurysm formation, rupture and increased intimal hyperplasia compared with nonvaricose venous grafts. We report the use of varicosed long saphenous vein (LSV) with external Dacron support in infrainguinal bypass procedures for limb salvage, where endovascular therapy was not feasible. The external Dacron tube was not brought close to the distal anastomotic area itself. With a mean follow-up of 18 months, duplex ultrasonography and computed tomography angiography showed no evidence of stenosis of the reinforced vein segments or aneurysmal degeneration of the residual vein. External reinforcement with Dacron prosthesis allows the use of autogenous greater saphenous veins with varicose dilatation without compromising graft patency and limb salvage.
Keywords
The autologous vein is a superior conduit for infrainguinal bypass surgery. 1,2 However, the use of autologous vein may be limited if these are postinflammatory wall changes in a small, phlebitic vein or if there is segmental varicose degeneration of the vein. 3 Although minor dilatation can be corrected by plication, tuck stitching, or resection-anastomosis, major extensive dilatation and varicosities usually contraindicate autologous vein bypass. Their large diameter and unfavorable flow dynamics predispose these veins to aneurysm formation and rupture. Furthermore, they undergo increased intimal hyperplasia compared with nonvaricose venous grafts. 4 This has led several authors to use external envelopment of varicose veins with prosthetic material. 5,6 We have an aggressive policy of endovascular management as first-line treatment for patients with lower limb occlusive disease and critical limb ischemia. 7–10 However, a proportion of patients still exists in whom subintimal angioplasty is not feasible. We report the use of a varicosed long saphenous vein (LSV) with external silver-impregnated Dacron support in infrainguinal bypass procedures for critical limb ischemia in patients for whom endovascular subintimal angioplasty was not an option.
Technique
All patients with critical limb ischemia have arterial duplex sonograms and vein mapping performed preoperatively in the vascular laboratory. If the LSV is the only possible conduit and appears to be varicosed on preoperative duplex ultrasonography, it is mapped.
The vein is harvested using a stepladder technique. Prior to excision of the vein, it is marked along its length with an indelible pen and 6-0 polypropylene subadventitial longitudinal thread from head to toe so that any twisting of the vein becomes obvious and can be easily avoided. A nontraumatic clamp is then placed through a silver-impregnated 10 mm Dacron Unigraft (UNIGRAFT-DV, Braun, Melsungen, Germany), and the distal end of the vein is clamped. The vein is straightened and allowed to rest within the Dacron tube without fixation, with ample vein allowed through at each end. This avoids a mismatch in compliance between the Dacron graft and arterial segment and prevents constriction of the vein, which could reduce graft wall elasticity and promote formation of distal anastomotic intimal hyperplasia. 11
Following formation of the proximal anastomosis with 6-0 Serapren polypropylene sutures (Serag Wiessner, Naila, Germany), blood is allowed to flow through the proximal anastomosis to distend the the vein-graft. After reclamping, the distal end of the reinforced graft is usually tunneled subsartorially or subcutaneously. The graft is then flushed with heparin, and the distal anastomosis is fashioned with 6-0 Serapren polypropylene.
In the first case, the patient had nonhealing ischemic infected ulcers; in the second case, the patient had an inflammatory ruptured superficial femoral artery (SFA) aneurysm; and in the third case, the patient had a popliteal artery aneurysm (PAA) with distal embolization and gangrene of his toe. Thus, in all cases, because of signs of infection, we elected to use a silver-impregnated Dacron Unigraft to reinforce the vein conduit.
Case Reports
Case 1
A 62-year-old lady presented with a nonhealing left leg ulcer for 6 months and rest pain for 2 weeks (Figure 1). She is an ex-smoker with unstable angina, poorly controlled hypertension, chronic obstructive airways disease, renal impairment, and CREST syndrome. Her ankle brachial indices (ABIs) were 0.6 bilaterally, with digital pressures of 86 mm Hg on the right and 50 mm Hg on the left. Lower limb duplex ultrasonography demonstrated a left external iliac artery (EIA) 5 cm stenosis. She also had an SFA occlusion, which had echolucent material and no nipple, which would allow initiation of a subintimal plane. 8 We elected to perform a left EIA angioplasty and stenting with concomitant left common femoral artery to below-the-knee popliteal artery bypass by vein graft, tunneled subsartorially. Operation involved stepladder harvest of her LSV, which was found to be varicosed and thus was reinforced externally by a 10 mm Silver Dacron Unigraft (Figure 2). The patient was seen postoperatively at 6 weeks, 3 months, 6 months, and 9 months. At each visit, she had arterial duplex ultrasonography, ABIs, and digital pressures. Her ulcer is now healed, and duplex ultrasonography confirmed the patency of the graft. 12

Ischemic ulcer (case 1).

Varicosities along a harvested long saphenous vein (case 1).
Case 2
A 73-year-old male, hypertensive smoker with atrial fibrillation and class I heart failure presented with swelling over the medial aspect of his right thigh, which had increased in size over the course of the preceding 6 weeks. He was unable to weight-bear or flex his knee owing to pain. On examination, there was a pulsatile mass over the medial aspect of the right midthigh. The mass was tender to touch, indicating impending rupture. There was also evidence of distal ischemia and embolization. His right ABI was 0.7.
Duplex sonograms revealed an SFA aneurysm with a diameter of 9.4 cm and an incidental finding of a 3.5 cm abdominal aortic aneurysm.
On a magnetic resonance angiogram (Figure 3), there was no flow below the common iliac artery on the contralateral asymptomatic left side, in spite of a normal ABI. The reason for this was the presence of an arteriovenous (AV) fistula between the right SFA and the right superficial femoral vein, causing low resistance and high flow, the presence of which was confirmed at operation.

Peripheral magnetic resonance angiogram (case 2). A, Absence of blood flow to the contralateral asymptomatic leg owing to hemodynamic steal to the symptomatic ipsilateral leg. The cause is timing of the magnetic resonance angiography. B, The superficial femoral artery aneurysm.
At operation, his SFA aneurysm was found to have ruptured, with evidence of thrombus. The LSV from the opposite left side was harvested through a stepladder skin incision; it had numerous varices along its course. The vein was reversed and laid within a 10 mm silver Dacron Unigraft (Figure 4). The graft was tunneled subsartorially and anatomically through the popliteal fossa to below the knee and anastomosed to the distal popliteal artery using 6-0 Serapren polypropylene sutures. His postoperative course was uneventful. Serology for syphilis was negative. Culture and sensitivity swabs taken intraoperatively were also negative. Histology confirmed an atherosclerotic aneurysm. The patient was seen postoperatively at 6 weeks, 3 months, 6 months, 9 months, and yearly thereafter, and at each visit, he had arterial duplex ultrasonography, ABIs, and digital pressures. Two years postoperatively, the graft remained primarily patent on duplex ultrasonography (Figure 5). 12 The patient also had computed tomographic angiography 2 years postoperatively. This was because his abdominal aortic aneurysm had expanded and he needed assessment for endovascular aortic aneurysm repair. None of the investigations showed evidence of stenosis of the reinforced vein segments or aneurysmal degeneration of the residual vein, nor were there any signs of septation or areas of turbulence.

Left long saphenous vein with varicosity at its proximal end, with a Dacron 10 mm patch overriding it (case 2).
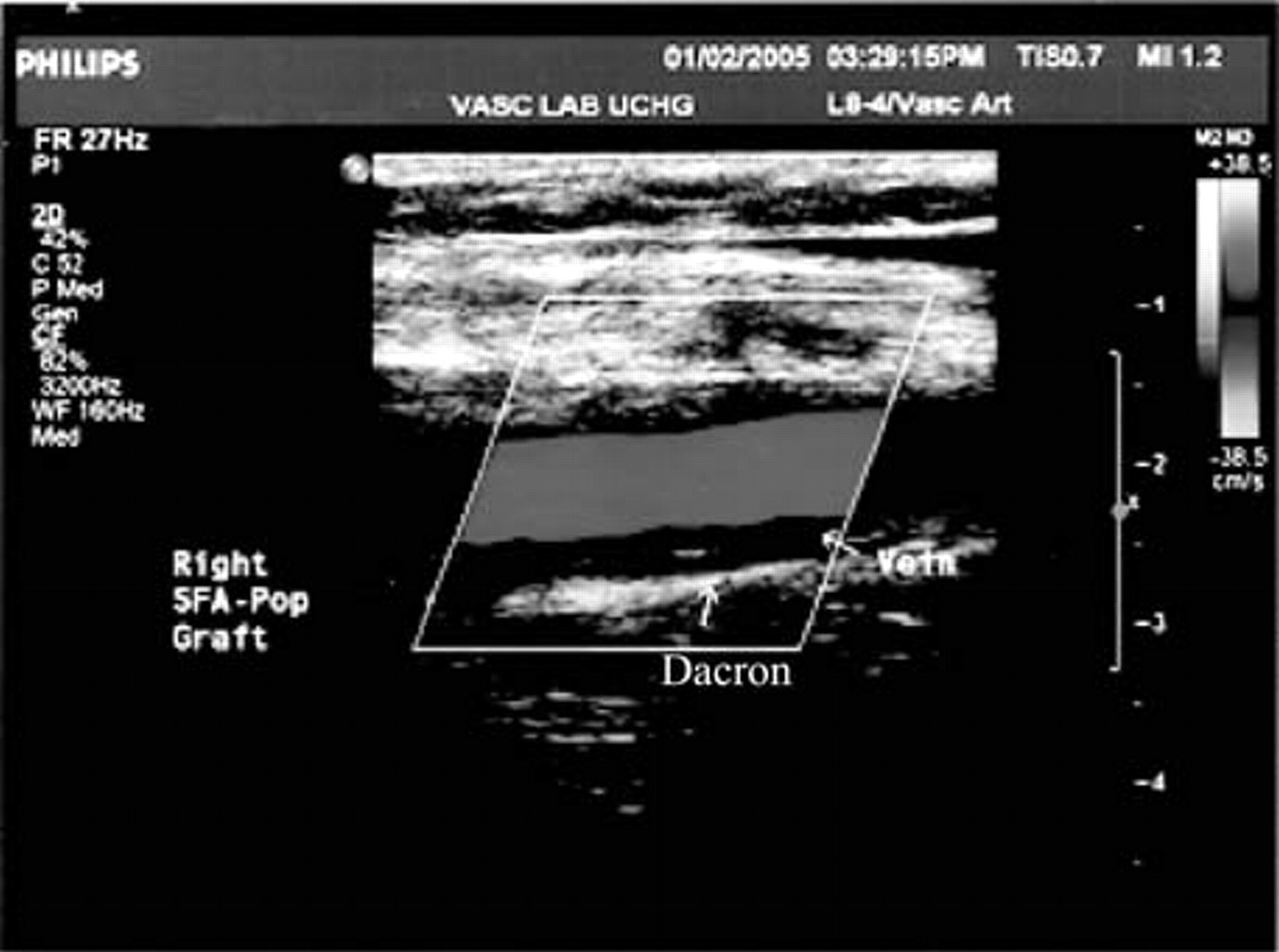
Color duplex ultrasonography 2 years following superficial femoral artery aneurysm repair (case 2).
Case 3
A 51-year-old male heavy smoker was transferred from a district hospital with a 9-day history of a painful, cold right foot with blue discoloration of his middle toe. Echocardiography showed no cardiogenic embolic source, and duplex ultrasonography demonstrated no abdominal aortic aneurysm. Lower limb arterial duplex ultrasonography revealed a 4.1 × 4.6 cm right popliteal aneurysm with thrombus and patent superficial femoral and crural arteries. His left popliteal artery was not aneurysmal, and his ABIs were normal bilaterally. His left LSV was marked for use in a right femoropopliteal artery bypass with aneurysm ligation. At operation, following a stepladder harvest, his LSV was found to be thin walled and varicosed. The vein was externally supported using a 10 mm silver Dacron Unigraft. His postoperative course was uneventful, and 9 months postoperatively, his graft remained patent on duplex ultrasonography. 12
Discussion
Our first-line management for patients with lower limb occlusive disease and critical limb ischemia is subintimal angioplasty. 7–10 Ninety percent of our patients are treated by subintimal angioplasty alone, with less than 6% requiring subsequent surgery. 7 Our limb salvage rate with this technique now approaches 97%, and we have shown the technique to be cost-effective and minimally invasive, without compromising primary patency, patient survival, and subsequent vascular intervention. 7 However, a small proportion of patients still exists in whom subintimal angioplasty is not possible.
When we perform bypass surgery, our preferred conduit is always the autologous vein. The excellent long-term results with the autologous LSV in infrainguinal bypass surgery have not been matched by those with synthetic materials. 1,2 This is especially true when crossing the knee, and many reports, including randomized, multicenter trials, can confirm that the autologous saphenous vein is the material of choice when limb revascularization is performed at the level of the distal popliteal artery or tibial vessel. 2,13–15 However, the presence of varicosities in the harvested vein can limit its use. The abnormal wall structure of varicose veins, with increased fiber propagation parallel to the enlargement of the vessel wall, decreased mechanical properties, and variations in lumen diameter, can lead to hemodynamic disturbance, turbulence, aneurysm development, and increased long-term risk of thrombosis, embolization, and rupture when exposed to arterial pressure. 16,17 Even long-term functioning normal vein grafts have been found to be at significant risk of aneurysmal degeneration. 18,19
To overcome these limitations, many authors have suggested the use of synthetic material to reinforce the vein. Parsonnet and colleagues first proposed the use of Dacron to externally reinforce a nondiseased vein. 20 Since then, similar techniques have been described in both normal and varicosed veins. Derieu and colleagues performed polytetrafluoroethylene (PTFE) wrapping of normal LSV segments in distal bypass surgery to prevent external compression and strangulation by scar tissue after reoperation and reported satisfactory graft function. 21 Melliére and colleagues used dilated segments of the LSV, which were wrapped in short segments of PTFE prosthesis or handmade Dacron mesh, in a small series of patients, with no complications and no dilatation in the unwrapped segments during follow-up. 22 In addition to this clinical series, other authors have described extensive external wrapping with prosthetic material of highly varicosed LSV, with excellent long-term results. 23,24
In our first case, duplex ultrasonography demonstrated echolucent material in the SFA, indicating the presence of thrombosis. This made it impossible to manage by subintimal angioplasty owing to the risk of distal embolization and rethrombosis. 7,8 We used a combination of techniques. Percutaneous transluminal angioplasty and stenting of her left EIA allowed us to increase her inflow while at the same time we performed a common femoral to below-the-knee popliteal artery bypass, preferring to use the autologous vein when crossing the knee. 2 However, this was limited by the presence of significant varicosities in the harvested vein, which had not been demonstrated on preoperative duplex ultrasonography. We elected to reinforce the vein externally with a 10 mm Silver Dacron graft. Nine months postoperatively, she was hemodynamically and symptomatically patent. Her ulcer is healed, and duplex ultrasonography confirmed the patency of the graft.
Our second case is an atherosclerotic SFA aneurysm. True atherosclerotic SFA aneurysms are extremely unusual entities. A report by Graham and colleagues of 172 arteriosclerotic femoral aneurysms did not mention SFA aneurysms, 25 nor did the reviews by Levi and Schroeder or Baird and colleagues. 26,27 These are attributed to weakening of the arterial wall owing to atherosclerosis and are mostly found in elderly smoking men. 25 Aortic aneurysms are approximately 10 times more common in patients with true femoral artery aneurysms, 25 and our patient had a 3.5 cm abdominal aortic aneurysm extending into the common iliac artery bilaterally. Like the majority of patients with SFA aneurysms, his aneurysm remained undetected until rupture.
There have been no reported cases of an atherosclerotic SFA aneurysm with an AV fistula in situ. Our patient developed an AV fistula between the SFA and the vein. The presence of the fistula suggests an inflammatory component to the aneurysm, but we found no evidence of an inflammatory process, with the erythrocyte sedimentation rate, C-reactive protein, syphilitic screen, immunologic screen, and culture and sensitivity all being normal. The reason for the AV fistula formation may be due to the size of the aneurysm. This aneurysm is the second largest reported (range 3–12 cm; average 5.9 cm), and the pressure effect most likely led to the AV fistula. The lack of evidence of inflammatory, immunologic, or connective tissue disorders suggests that this was a truly atherosclerotic aneurysm.
Cutler and Darling first described 63 procedures on atherosclerotic femoral aneurysms. 28 Since then, most reported cases have been repaired by vein graft (either in situ or from the contralateral leg) or prosthetic graft (PTFE or Dacron graft), above or below the knee, with surgeons using different modalities to suit the situation and circumstances of the patient and the surgeon's preference. No cases in the literature had been repaired using a combination of vein and Dacron graft.
Our third case is that of a PAA complicated by distal embolization. The optimal management of PAAs remains unclear. Although endovascular stents have been used with some success, the aneurysm needs to be anatomically suitable; open surgical techniques are still the mainstay of treatment. However, limb salvage is notoriously low in patients with symptomatic PAAs. 29 Nevertheless, although long-term graft patency may not be good, limb salvage is achieved if the graft remains patent for more than 1 year. 30 Use of the autologous vein undoubtedly allows for increased chance of extended patency and thereby improves the probability of limb salvage. Not wishing to compromise this chance, we used the LSV, despite extensive varicosities, by reinforcing it with a silver Dacron graft. We found no reports of varicosed saphenous veins reinforced by a Dacron graft in PAA repair.
This is the first report that demonstrates the versatility and variety of applications of this technique. The only other reported indication was described by Moritz and colleagues, in which they used a special Dacron mesh for wrapping varicose veins and implanted the graft in an aortocoronary position and a femorodistal position, with satisfactory clinical and functional results for both. 5,31
As an alternative to prosthetic material, the use of an ultraflexible metal mesh tube intraoperatively has been described. 32 In our cases, we used the silver Dacron graft owing to the high risk of infection in all three cases, but any type of prosthetic material would probably be compatible. The advantage of the grafts we used was their “off-the-shelf” availability. Other groups recommend mesh grafts to avoid ischemia of the vein wall by enhancing contact between the vein graft and well-vascularized surrounding tissue. 5,33 Another advantage of using mesh tubes is to avoid entrapment of perivenous effusion, which can lead to graft stenosis. These devices are now available in a variety of sizes off the shelf and are composed of open-pore biocompatible materials that adapt to the irregularities of the exterior vein wall. Application sets also allow for quick preparation of the hybrid graft.
We found no evidence of intimal hyperplasia during follow-up in any of our cases. Some authors have reported that constriction of venous grafts by a Dacron mesh tube reduces graft wall elasticity and promotes formation of distal anastomotic intimal hyperplasia. 11 To avoid such an increased mismatch in compliance while making use of the advantages of this method, the external mesh tube must not be brought close to the distal anastomotic area itself.
Endovascular therapy remains our first-line management of critical limb ischemia. However, there are patients for whom endovascular therapy is not feasible and in whom venous varicosities would previously have precluded autologous bypass. We believe that Dacron graft–vein bypass is superior to synthetic bypass for infrainguinal revascularization in these patients, allowing the superiority of the vein without compromising graft function and integrity.