
Abstract
The objective of this study was to evaluate the applicability of paravertebral blockade (PVB) for endovascular abdominal aortic aneurysm repair compared with general anesthesia (GA).
Data from patients who underwent elective infrarenal endovascular abdominal aortic aneurysm repair between August 2001 and July 2002 using PVB or GA were retrospectively reviewed and compared with respect to risk factors, intraoperative hemodynamic characteristics, operative outcome, and complications.
Ten patients underwent elective infrarenal endovascular abdominal aortic aneurysm repair under PVB, whereas 15 patients were operated on under GA. One conversion from PVB to GA was necessary for block failure. The perioperative (< 30 days) cardiovascular morbidity and overall mortality were zero in both groups. The PVB group benefited significantly with respect to the incidence of intraoperative hypotension (p < .05) and blood pressure lability (p < .01), as well as postoperative nausea (p < .01). Our preliminary results indicate that PVB is feasible and can be performed safely in a patient population with significant comorbidities.
Keywords
Endovascular aneurysm repair (EVAR) provides a less invasive treatment for abdominal aortic aneurysms (AAAs) compared with the traditional open, transabdominal approach. The lesser surgical trauma of this technique resulted in a significantly reduced operation time, intraoperative blood loss, and length of intensive care and hospital stay. 1–3 Two recent studies demonstrated a significant reduction in the perioperative risk for EVAR compared with open AAA repair in patients who would qualify for either intervention. 2,3 Although earlier reports suggested that EVAR may be suitable for patients that are unfit for elective transabdominal surgery, 1 the EVAR-2 trial showed no advantage concerning short- and intermediate-term survival after endovascular treatment for AAA compared with no intervention in patients unfit for open repair owing to a considerable operative mortality. 4
The issue has been raised as to whether the type of anesthesia may play a significant role concerning perioperative morbidity and mortality. 5,6 General anesthesia and other techniques including epidural anesthesia have been demonstrated to affect hemodynamics. 7 These methods do not differ significantly in terms of perioperative cardiovascular risk. 8–10 Although benefits were expected from local anesthesia in this respect, controversial outcomes have been published. 5,7,11
Paravertebral blockade (PVB) is a regional anesthesia technique. Local anesthetic is injected lateral to the vertebral column, where the spinal roots emerge from the intervertebral foramina and bifurcate into the dorsal and ventral rami. PVB provides unilateral motor, sympathetic, and sensory block, 12 resulting in complete deafferentiation of the corresponding dermatomes. PVB has been reported as the primary method of anesthesia in inguinal hernia repair and breast surgery 12–14 and for postoperative analgesia after GA in patients undergoing transperitoneal aortic surgery. 15
We report our initial experience with this innovative technique combined with intravenous sedation for elective endovascular treatment of AAA compared with GA.
Methods
Data were collected and analyzed retrospectively. Between August 1, 2001, and July 31, 2002, PVB was offered to eligible patients undergoing endovascular procedures. Within this time frame, 31 patients underwent endovascular repair of an AAA at our institution. For this analysis, patients with PVB were compared with those operated on under GA.
Patient inclusion criteria for EVAR included significant medical comorbidities, a hostile abdomen, or high surgical risk as defined by the American Society of Anesthesiologists' (ASA) physical status classification. 16 In addition, endovascular treatment was also offered based on patient preference, in the presence of acceptable aortoiliac anatomy. During their preanesthesia visit, patients scheduled for EVAR were given the choice between GA, neuroaxial block, or PVB with intravenous sedation where appropriate. All patients gave written informed consent to the procedure and type of anesthesia. Board-certified anesthesiologists performed all PVBs. EVAR was performed in the operating room by two vascular surgeons in collaboration with an interventional radiologist. Postoperatively, patients were observed in a postanesthesia care unit for several hours, followed by admission to the ward.
Anesthetic Techniques
Patients were fasted for a minimum of 8 hours except for certain medications. Midazolam 2 mg was administered as premedication. All patients received prophylactic perioperative antibiotics (cephazolin, vancomycin, or erythromycin) intravenously.
A radial arterial line, a 14- or 16-gauge peripheral venous catheter, and a urinary Foley catheter were placed. All attempts were made to keep the patient euthermic, including warming of the intravenous fluids and the use of an upper body forced-air warming blanket.
Paravertebral Blockade
PVB was achieved as described previously. 17 The patient was placed in a sitting position, with the back rounded and the shoulders relaxed forward, similar to a spinal approach. During block placement, standard preoperative monitoring was applied and resuscitation equipment was available. To achieve sufficient analgesia to allow for inguinal vascular access, bilateral blockade of segments T12 through L2 is needed. These spinal segments were identified and marked. The back was then prepared in a sterile fashion, and a skin wheal was made at each injection site with 1% lidocaine. A 22-gauge, 8.9 cm Tuhoy epidural needle was introduced in a parasagittal plane 2.5 cm lateral to the median, bilaterally, and advanced for 2 to 5 cm until the transverse process was contacted. After initial bone contact, the needle was walked carefully in a caudad direction. The paravertebral space was entered through needle advancement about 0.5 cm beyond the transverse process. After aspiration to avoid inadvertent positioning of the needle tip, 4 mL of ropivacaine (0.5–1.0%) with 1:200 to 1:400 K epinephrine was administered at each dermatome, bilaterally, keeping the total ropivacaine dose under 3 mg/kg. Epinephrine was added to extend the duration of the block and to reduce the risk of hypotension that may arise from more rapid absorption. Intraoperatively, sedation was maintained with a propofol infusion and fentanyl boluses as needed. In one case, midazolam was administered instead of propofol. Respiration was spontaneous with 50% oxygen in air delivered via a face mask throughout the procedure. During the EVAR procedure under PVB with sedation, patient cooperation is required to facilitate graft deployment. All patients were awake enough to control their own airway and stop respirations voluntarily when requested. Conversion to GA was considered if the patient experienced significant pain at the beginning of the procedure.
General Anesthesia
GA was initiated with propofol and fentanyl and maintained with either isoflurane or sevoflurane, vecuronium, and fentanyl as required. Patients were intubated or a laryngeal mask was placed and the patients were extubated before leaving the operating room.
Perioperative Management
Continuous electrocardiogram (leads V5 and II), invasive arterial pressure, and urine output were monitored. The blood pressure level acquired in the preoperative holding area was taken as the basal level. Variations in systolic blood pressure by more than 30% were treated as customary. For patients with preexisting hyper- or hypotension, more narrow limits were applied. Accordingly, heart rates outside optimal limits of 40 to 85 bpm were treated. For patients in baseline atrial fibrillation, an upper limit of 100 bpm was accepted.
Postoperative Management
Postoperative pain management consisted of acetaminophen 500 mg given twice daily if required. If needed, combination medications containing an opiate (Vicodin 5/500: 500 mg acetaminophen + 7.5 mg hydrocodone or Darvocet 650 mg acetaminophen + 100 mg propoxyphene napsylate) or an oral opiate (Dilaudid: 2 mg hydromorphone) were given. Alternatively, parenteral morphine sulfate was administered. For statistical analysis, the total dose of opiate analgesics was calculated to an equianalgesic dose of parenteral morphine, according to published tables. 18 In case of nausea or vomiting, an antiemetic drug (dolasetron) was administered.
Data Analysis and Statistics
Analysis of hemodynamic parameters was performed as described by Christopherson and colleagues. 10 Blood pressure lability was defined as a variation in systolic blood pressure of more than 25 mm Hg within 5 minutes. Heart rate lability was defined as a variation of more than 20 bpm within 5 minutes. Values were reported as a percentage of patients in each anesthesia group who fell beyond their calculated limit from insertion of the arterial line to transport to the recovery room.
Statistical analysis was performed using SPSS, version 10.0, software (SPSS Inc, Chicago, IL). Data are expressed as mean ± standard deviation or as total number (percentage). Numeric data were tested for normal distribution using the one-sample Kolmogorov-Smirnov test, and Mann-Whitney U or Student's t-test was performed as appropriate for data comparison. Binomial variables were calculated using the chi-square or Fisher exact test. A p value of .05 or less was considered significant.
Results
Between August 1, 2001, and July 31, 2002, 31 patients underwent endovascular repair of an AAA at our institution. Eighteen patients were operated on under GA, 3 under spinal anesthesia, and for 10 patients, PVB was used as the primary method. In three of the GA patients, PVB was performed prior to induction of GA as an additional, planned analgesic measure. For this analysis, 10 patients with primarily planned PVB as the sole anesthetic method were compared with the 15 patients operated on under GA without receiving an additional PVB.
Patient demographics and risk factors are depicted in Table 1. The median age was 77 years (range 54–89 years). Twenty-two patients were male (88%) and three were female (12%). There were no significant differences between the groups concerning age; gender; ASA class; incidence of preexisting cardiac, pulmonary, or renal disease; and basic hemodynamic characteristics. None of the patients were on chronic pain medication.
Baseline Characteristics
ACE = angiotensin-converting enzyme; ASA = American Society of Anesthesiologists' physical status classification; AT II = angiotensin II; CABG = coronary artery bypass graft; CHD = coronary heart disease; COPD = chronic obstructive pulmonary disease; GA = general anesthesia; MI = myocardial infarction; NS = not significant; PTCA = percutaneous transluminal angioplasty; PVB = paravertebral blockade.
*Mean with standard deviation.
Consistent with the 10% failure rate of the PVB, one patient was converted to GA after he experienced sharp pain on skin incision. After conversion, the procedure was performed successfully and there were no further complications. The patient was excluded from further statistical analysis. Anesthetic lead time was slightly but significantly prolonged in patients undergoing PVB (PVB vs GA = 68 vs 54 minutes; p = .03). However, mean surgery time, length of operating room time, and total anesthesia time were similar. No puncture-site complication occurred during or after administration of PVB.
There was no significant difference in estimated blood loss, requirement of packed red blood cells and intravenous fluid administration, and urine output (Table 2).
Procedural Characteristics
EBL = estimated blood loss; GA = general anesthesia; IV = intravenous; NS = not significant; PACU = postanesthesiacare unit; PRBCs = packed red blood cells; PVB = paravertebral blockade.
The hemodynamic characteristics of the two groups are shown in Figure 1. Patients in the GA group were more likely to have hemodynamic instability. Blood pressure lability occurred in 53% of cases versus none in the PVB group (p < .01). Systolic blood pressure fell below the lower limit in eight (53%) of the GA patients compared with only one patient (11%) who had received PVB (p < .05). Fluctuations in heart rate occurred more frequently in the GA group (30% vs 25%); however, the difference was not significant. GA patients required more medical interventions to stabilize hemodynamics: 0.5 interventions per PVB patient versus 1.5 interventions per GA patient (p < .05).
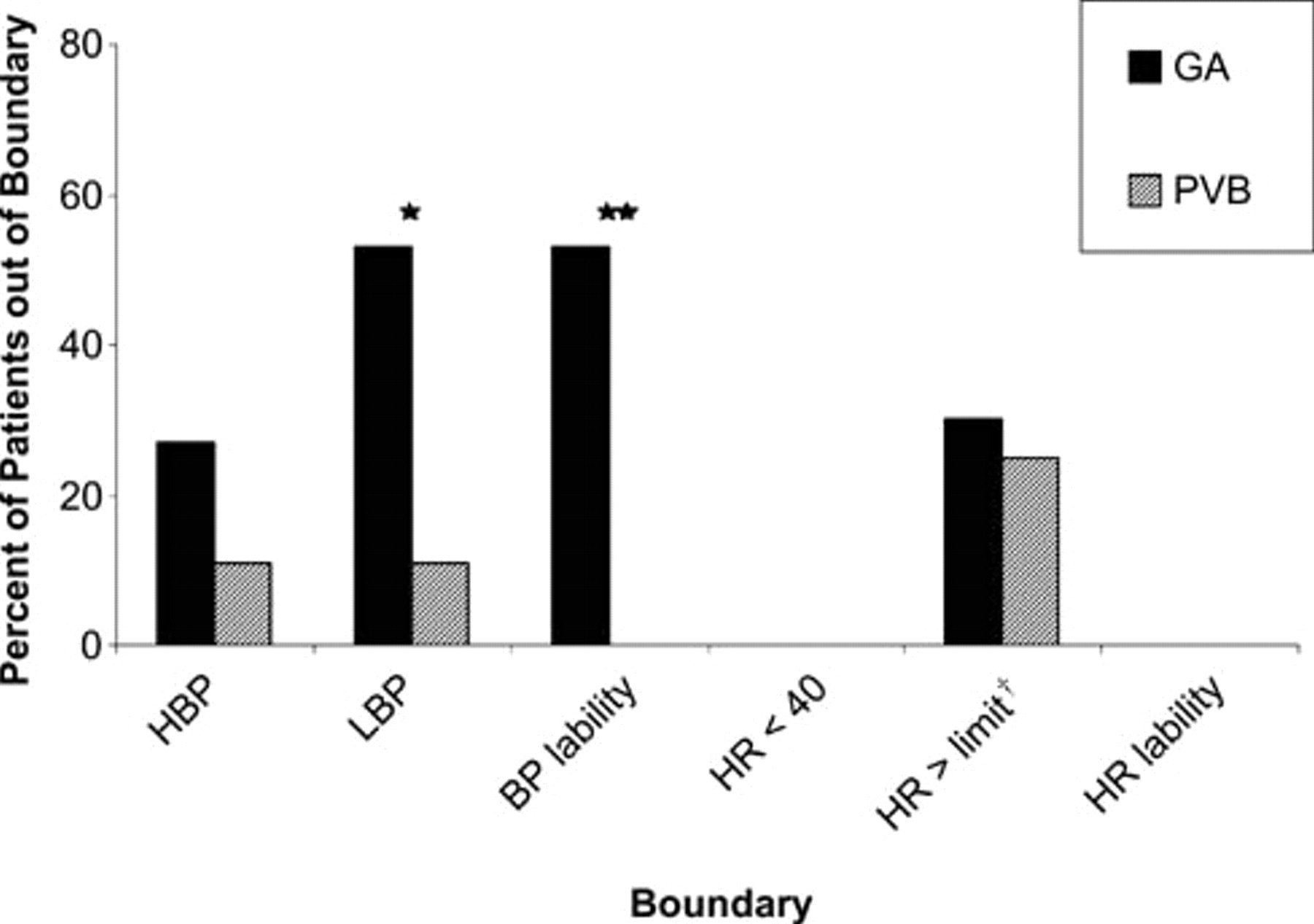
Hemodynamic characteristics. BP = blood pressure; GA = general anesthesia; HBP = upper limit of the individual allowable systolic blood pressure; HR = heart rate; LBP = lower limit of the individual allowable systolic blood pressure; PVB = paravertebral blockade. *p < .05; **p < .01; †upper HR limit of 85 bpm for patients with sinus rhythm and 100 bpm for patients with atrial fibrillation.
There were no conversions to open surgery. Two patients, both from the GA group, had a type 1 endoleak at the end of the procedure. One leak had thrombosed spontaneously on the 30-day follow-up computed tomographic examination, whereas the second leak required reintervention. Another GA patient suffered an immediate left iliac limb occlusion of his bifurcated graft owing to angulation that was treated by thrombectomy, adjunctive balloon dilation, and stent placement (Table 3).
Perioperative Complications
GA = general anesthesia; NS = not significant; PVB = paravertebral blockade.
*Equivalent of parenteral morphine (mg).
Postoperatively, GA patients received additional parenteral morphine over a longer period than PVB patients (GA vs PVB = 1.5 days vs 0.3 days; p = .03). However, the mean total parenteral morphine dose (GA vs PVB = 5.3 mg vs 1.6 mg) and the mean total opiate dose as calculated to equianalgesic morphine doses (GA vs PVB = 17 mg vs 16 mg) did not differ significantly.
Whereas postoperative nausea was frequent in the GA group (n = 12; 80%), only one patient from the PVB group was affected (11%; p = .001). Other complications in the GA group included pneumonia (n = 1), bleeding from multiple gastroduodenal ulcers (n = 1), and minor wound healing problems (n = 2).
All patients could be transferred from the recovery room to the ward on the day of surgery. Mean length of stay in the recovery room (GA vs PVB = 136 vs 120 minutes) and hospitalization time (4.6 vs 4.4 days) did not differ significantly.
Discussion
EVAR enables a minimally invasive approach to the aortoiliac vasculature using the femoral arteries as access vessels. The reduced surgical trauma allows for a broadened spectrum of applicable anesthesia regimens in aortic aneurysm repair.
Anesthetic techniques for EVAR described in the literature include GA, epidural anesthesia, combined single-shot spinal and epidural anesthesia, and direct local anesthesia. 5–7 Owing to concerns about the need for conversion to open surgery in cases of access vessel laceration or aneurysm rupture, GA was preferred in most early series. However, GA is associated with a risk of hemodynamic instability, 8 which may increase the risk of cardiovascular complications.
Neuroaxial anesthesia has been widely used and proven reliable during EVAR. 6,7 However, it is not always possible in older patients with significant comorbidities. Degenerative alterations of the spine, use of anticoagulants, or the presence of coagulopathies and an aortic stenosis may preclude the use of neuroaxial block in vascular patients. Potential complications of neuroaxial block include hypotension, compromised respiratory function, and urinary retention. 8,19 Although serious complications are rare, postdural puncture headache has been described in 0.2 to 24% of cases. 20
Verhoeven and colleagues reported a reduced incidence of respiratory complications for local and regional anesthesia compared with GA. 11 Although it is believed that local anesthesia minimizes cardiopulmonary morbidity rates in patients at high risk, de Virgilio and colleagues found similar cardiopulmonary complication rates comparing 229 EVAR procedures under general versus local anesthesia. 5 When local anesthesia was compared with other anesthesia regimens, a reduction in anesthesia and recovery room time, length of stay, and cost has been reported. 6,11 However, local anesthesia may not be feasible after previous surgery in the inguinal region or in patients with gross obesity. 11
In this study, we report a new approach to anesthesia/analgesia in EVAR patients by using bilateral PVB at the lower thoracic and upper lumbar levels. PVB is well established for anesthesia or analgesia for surgical procedures such as breast surgery and inguinal and ventral hernia repair. 12–14,21 Using bilateral injection at three levels, T12, L1, and L2, we achieved satisfactory analgesia for bilateral femoral artery exposure in 9 of our 10 patients undergoing EVAR under PVB.
Inadvertent vessel puncture, hematoma, pain at the puncture site, pleural puncture, and hypotension have been described as potential complications of bilateral PVB. 22 Whereas the risk of hemodynamic instability is certainly lower for PVB of lower thoracic and lumbar segments, the risk of pleural puncture is virtually absent. We did not encounter any of these complications. Hemodynamic stability was excellent in our PVB patients and distinctly superior to the patients under GA.
After single-injection PVB, a prolonged analgesic effect has been described for open inguinal hernia repair. 12 The need for supplemental opiate administration was significantly lower for surgical management of breast cancer after PVB compared with GA. 13 However, in our series, there was no relevant difference regarding postoperative opioid requirement. Continuous PVB might be more advantageous in this respect 19 .
Although postoperative nausea was a major issue after GA, it was observed in only one patient following PVB. This compares favorably with previously published data. 13,14
Although our frequency of 10% of initial PVB failure might appear to be high, it is within the published range of a 5 to 10% failure rate in larger series. 13,22 Naja and Lonnqvist achieved a higher success rate with the aid of a nerve stimulator. 22 Our results are also comparable with anesthetic conversion rates for EVAR in local anesthesia (0–15% 5,6 ) and epidural anesthesia (14% 6 ).
The major drawback of this study certainly is its retrospective character, which causes a lack of standardization, especially in the general surgery group. However, we could demonstrate that PVB offers a sound alternative to GA for patients undergoing EVAR. Based on these preliminary results, a prospective evaluation of the use of PVB compared with established anesthesia techniques for endovascular aneurysm exclusion is warranted. Adjunctive techniques, including the use of a nerve stimulator for more accurate block placement and insertion of a catheter for continuous anesthetic application, might improve efficacy.
Footnotes
A Vascular Surgery Research Grant from the William J. von Liebig Foundation supported the work of Matthias Biebl, Josef Klocker, Louis L. Lau, and Beate Neuhauser at Mayo Clinic Jacksonville.
Parts of the data were presented at the 26th World Congress of the International Society for Cardiovascular Surgery 2004 in Maui, Hawaii.