
Abstract
Carotid artery surgery (CAS) performed under cervical plexus block is frequently associated with significant intra- and postoperative pain. To evaluate whether preoperative administration of ketorolac may improve analgesia in this type of surgery, 80 patients scheduled for CAS under cervical plexus block were randomly allocated to receive intravenously either 30 mg of ketorolac or placebo 30 minutes before surgery. Verbal rating scale pain scores during surgery and 3 and 6 hours after surgery, the number of patients requiring additional analgesia, and the total analgesic consumption both during and within 6 hours after surgery were significantly lower, whereas the time to first postoperative analgesia was significantly shorter in the ketorolac group than in the control group.
The results of this prospective, randomized, double-blind study show that a single 30 mg dose of ketorolac administered intravenously 30 minutes before surgery reduces intraoperative pain and preempts postoperative pain in patients undergoing CAS under carotid plexus block.
Cervical plexus block (CPB) is frequently used for carotid artery surgery (CAS). 1 As a one-time antinociceptive treatment starting before surgical incision, CPB should provide an adequate level of intraoperative analgesia, with the possible efficacy limited to the immediate postoperative period.
The largest published series of 1,000 CPBs for carotid endarterectomy, however, reported that local anesthetic supplementation was required in 53% and intravenous sedation in 66% of patients. 2 A number of sedatives and opioids, as well as their combinations, have been employed to improve the patients' comfort and cooperation during surgery. 3–6 These drugs may not only impair mental status evaluation but may also compromise respiratory and/or cardiovascular function. Furthermore, high-intensity noxious stimuli from surgery-caused injury may trigger central sensitization, which amplifies postoperative pain. 7 It is not rare, indeed, that narcotic analgesics are administered for pain relief after this type of surgery, 6,8 which may delay postoperative recovery.
Nonsteroidal anti-inflammatory drugs (NSAIDs) are suitable for mild to moderate pain, 9 their analgesic effects being attributed primarily to the peripheral anti-inflammatory actions in inhibiting synthesis of prostaglandins through cyclooxygenase inactivation. 10 It has been reported that preoperative NSAID use may preempt postoperative pain by preventing both peripheral and central sensitization. 11,12
In this prospective, randomized, double-blind, placebo-controlled clinical trial, we investigated whether preoperative administration of a single dose of ketorolac, an NSAID with strong analgesic activity, may reduce pain during and after CAS performed under CPB.
Patient Population and Methods
After obtaining approval from the Institutional Ethics Committee and written informed consent, we studied 80 patients, aged 49 to 80 years, scheduled for elective CAS under CPB. Patients with known contraindications to NSAID use and those with a history of allergy to anesthetics or NSAIDs were excluded from the study. Patients were allocated randomly to one of the two groups, using a computer-generated random numbers table, to receive either intravenous (IV) ketorolac 30 mg or saline placebo 30 minutes before surgery. Prior to surgery, each patient was instructed on the use of the verbal rating scale (VRS 0–10; 0 = no pain; 10 = the worst pain imaginable) for reporting pain. 13
All patients were premedicated with intramuscular (IM) midazolam 0.03 mg kg−1 and atropine 0.01 mg kg−1. A 16-gauge peripheral IV cannula was sited, and a 20-gauge cannula was inserted in the contralateral radial artery for invasive arterial blood pressure measuring and blood gas sampling. Other monitoring included five-lead electrocardiography (leads II and V5), noninvasive blood pressure, and pulse oximetry.
Placement of CPBs was performed by the attending anesthesiologist experienced in the technique. Deep CPB was performed by a three-injection technique at the C2, C3, and C4 levels, as described by Moore, 14 using a mixture of 15 mL bupivacaine 0.5% and 5 mL lidocaine 2%. The superficial block was performed by injecting 15 mL of the above-mentioned anesthetic mixture in the subcutaneous plane along the posterior border of the sternocleidomastoid muscle and along the inferior border of the mandible. Twenty minutes after the block was placed, loss of pinprick sensation in the C2–C4 dermatomes confirmed that the patient was ready for surgery. A single 2 mL aliquot of lidocaine 2% was administered topically onto the carotid sheath prior to carotid artery dissection. Propofol in 20 mg IV bolus doses was given to patients reporting discomfort throughout the procedure. A Javid shunt was placed if there was a change in neurologic status during carotid cross-clamping. After surgery, the patients were observed routinely in the postanesthesia care unit (PACU) for 6 hours and were given 1 g of oral acetaminophen for moderate pain or 50 mg of IM tramadol for severe pain.
Postoperatively, all patients were asked to score the level of pain they had experienced during and 3 and 6 hours after surgery by using an 11-point VRS. In addition, the number of patients receiving propofol, the total amount of the drug given intraoperatively, the number of patients requiring postoperative analgesia, the time to first analgesia after surgery, and total analgesic consumption within the investigated period were recorded. All perioperative adverse events were also noted.
The attending anesthesiologist, surgeon, PACU staff who administered postoperative analgesia, and the investigator who recorded the pain scores were blinded to the treatment group.
Data are presented as mean (SD), median (range), and number (%). Statistical analysis was performed using Student's t-test, Mann-Whitney U test, and Fisher exact test, where appropriate. A value of p < .05 was regarded as significant. Assuming that approximately 65% of patients require analgesia and sedation during CPB for CAS, 2,8 we calculated that to detect with 80% power and at the 5% two-sided significance level a 50% reduction in the aforementioned event rate, 34 patients would be required in each group. 15 Thus, 40 patients per group was considered sufficient to allow for inevitable dropouts.
Results
Seventy-five patients were enrolled in the study. Three patients with peptic ulcer disease, two patients with renal dysfunction, and one patient with a known allergy to NSAIDs were excluded from the study. The two groups were comparable with respect to demographic, clinical, and surgical characteristics (Table 1).
Patient Characteristics, Medical History, and Surgical Data for the Ketorolac and Placebo Groups
*Data expressed as mean ± SD.
†Data expressed as number (%).
‡Data expressed as median (range).
Patients in the ketorolac group were significantly less likely to receive intraoperative propofol supplementation than those in the placebo group (relative risk = 0.5). Ten patients (27%) in the ketorolac group, compared with 22 patients (58%) in the placebo group, required propofol intraoperatively (p = .01) (Table 2). Total propofol consumption was significantly less in the ketorolac group (13.5 ± 25.0 mg) than in the control group (37.4 ± 48.8 mg) (p = .01). In addition, patients in the ketorolac group had a significantly lower VRS pain score (1.9 ± 1.0) during surgery than did patients in the placebo group (2.8 ± 1.5; p < .01) (Figure 1).
Pain Assessment during and in the First 6 Hours after Surgery in the Ketorolac and Placebo Groups
*Data expressed as number (%).
†Data expressed as mean ± SD.
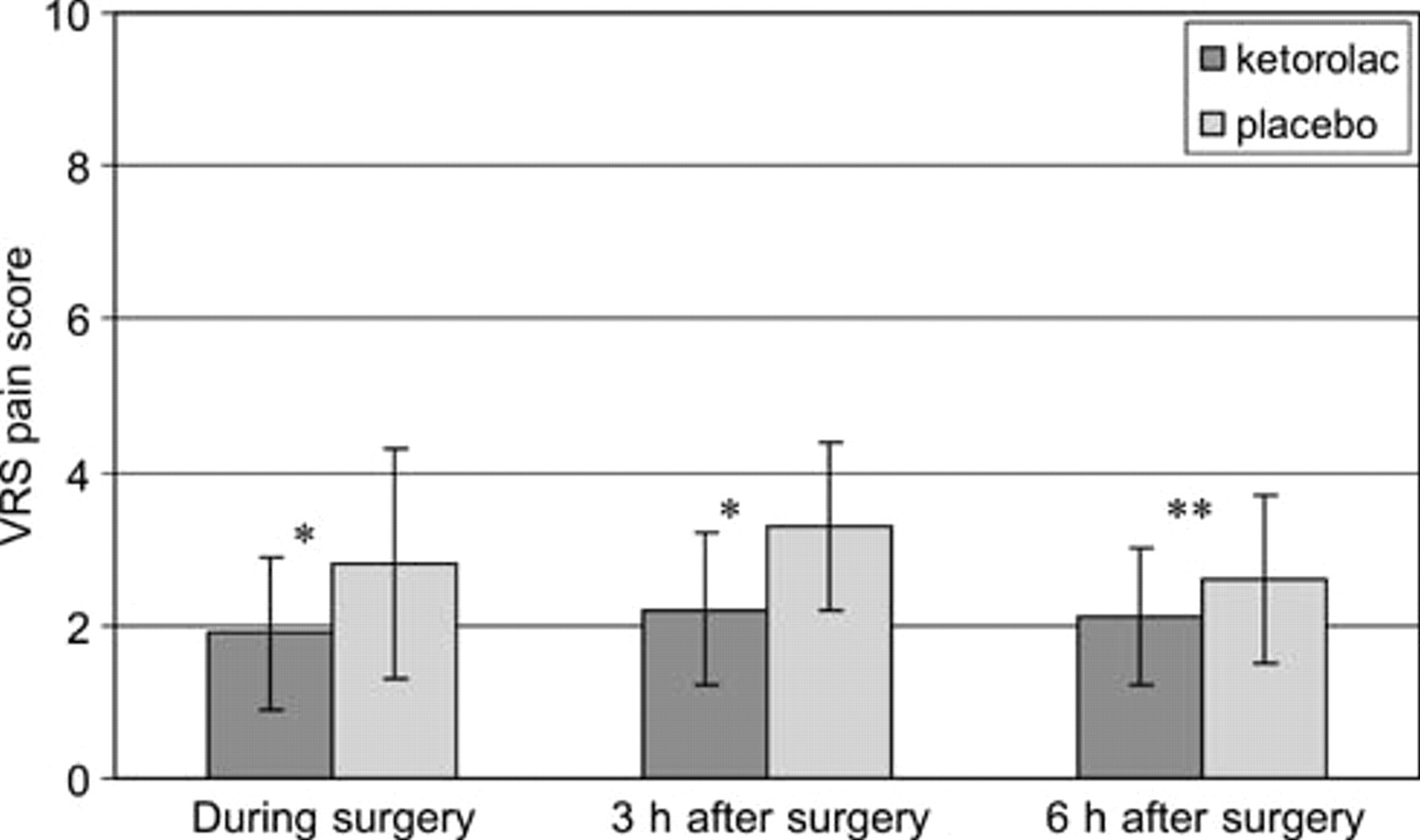
Verbal rating scale (VRS) pain scores during surgery and 3 and 6 hours after surgery in the ketorolac and placebo groups. *p < .01; **p = .03.
Patients who had received a single 30 mg dose of IV ketorolac preoperatively requested supplemental analgesia within 6 hours after surgery significantly less frequently than placebo patients did (relative risk = 0.2). Only four patients (11%) in the ketorolac group, compared with 21 patients (55%) in the placebo group, received an additional analgesic in the cited period (p < .01) (see Table 2). The total amount of acetaminophen consumed was significantly lower in the ketorolac group (0.1 ± 0.3 g) than in the placebo group (0.5 ± 0.5 g) (p < .01). None of the patients in the former group, compared with six patients (16%) in the latter one, required tramadol for postoperative pain relief (p = .03). The ketorolac group reported a longer time to first analgesic administration (3.2 ± 0.5 hours) compared with the placebo group (2.1 ± 0.7 hours) (p < .01). Moreover, the ketorolac group had a significantly lower VRS pain score than the placebo group both 3 hours (2.2 ± 1.0 vs 3.3 ± 1.1; p < .01) and 6 hours after surgery (2.1 ± 0.9 vs 2.6 ± 1.1; p = .03) (see Figure 1).
Two patients needed placement of a Javid shunt, one in each group. There were no perioperative permanent neurologic deficits. No significant bleeding problems were observed by the surgeon either during or after surgery. None of the patients needed conversion to general anesthesia. All patients were transferred to the ward 6 hours after operation and were discharged home on the second or third postoperative day.
Discussion
The results of our study show that a single 30 mg dose of ketorolac, administered intravenously 30 minutes before operation, improves both intra- and postoperative analgesia in patients undergoing CAS under CPB.
Intraoperative Pain
The combined (superficial and deep) CPB provides suitable operating conditions for CAS. 2 However, some patient discomfort is frequently encountered, the main cause probably being irregularly innervated surgical areas. 16 Anxiety and fear may be important contributing factors in pain genesis. In the study of Merle and colleagues using 20 mL of 2% lidocaine for superficial CPB and approximately the same amount of 0.5% bupivacaine for deep CPB, 7 of 11 patients (64%) required intraoperative fentanyl in addition to supplemental local anesthetic infiltration. 3 Of these, 43% received the drug during tissue retraction and almost all (86%) during carotid intima dissection. Similar results were obtained when 30 mL of ropivacaine 0.375% was used for combined CPB. 8 Furthermore, Umbrain and colleagues reported only half of patients to have been completely satisfied with analgesia provided by the above-mentioned CPB technique. 17 Increasing ropivacaine concentration to 7.5 mg/mL in the same study reduced the incidence of intraoperative pain but increased that of side effects (coughing, hoarseness), although without reaching statistical significance.
In our study, the number of patients requiring supplemental analgesia (58%) and the overall VRS pain score (2.8 ± 1.5) during CAS under combined CPB alone was in agreement with previously reported data. 3,8 Preoperative IV administration of ketorolac 30 mg, however, significantly reduced (1.9 ± 1.0) the intraoperative VRS pain score and the relative risk of propofol supplementation by 50%. This supports the previous clinical findings that ketorolac, owing to its strong analgesic potency, is suitable for treatment of moderate to severe pain, which requires analgesia at the opioid level. 18 Ketorolac inhibits both cyclooxygenase and lipoxygenase enzymes and may release endogenous opioids, 19 which makes it more potent than other NSAIDs. Thus, ketorolac 30 mg IM was demonstrated to be as efficacious as morphine 12 mg IM or meperidine 100 mg IM in reducing the pain associated with major surgery. 20
Furthermore, a single 30 mg dose of ketorolac, given preoperatively in the current study, reduced the total propofol consumption by 64%, which may be of particular importance in maintaining hemodynamic stability and in keeping the patient awake enough to allow close neurologic assessment during carotid cross-clamping.
We chose propofol as an adjunct to CPB because it was confirmed to be as effective as opioids but was associated with fewer adverse effects. 4 We administered repeated bolus doses of propofol rather than continuous infusion, not only because eventual painful stimuli have been transitory during CAS but also to avoid oversedation. 21 Only a single 2 mL aliquot of lidocaine 2% was administered topically onto the carotid sheath to simulate the usual clinical practice at our institution, based on our own experience and previous studies suggesting that the need for occasional intraoperative sedation is high, despite the repeated surgical field infiltration with a local anesthetic. 3,8
As sole analgesics, NSAIDs, including ketorolac, are not suitable for intraoperative pain control for the sake of their “ceiling” effect. Ketorolac is recommended for the short-term management of acute postoperative pain 19 and can be initiated only after the pain occurs or, better, some time before surgery-induced nociception starts, which is an approach underlying the concept of preemptive analgesia. 7 In the present study, ketorolac, administered preoperatively primarily for the latter purpose, reduced intraoperative pain, which may be an additional benefit in terms of consecutively diminished stress response, improved patient comfort, and reduced need for analgesia and sedation during surgery.
Postoperative Pain
Although CPB attenuates the transmission of noxious afferent information from the incisional injury to the spinal cord, a large number of patients requiring supplemental analgesia during surgery indicate that CPB may not block it completely. Moreover, as a one-time intervention, it may not abolish afferent barrage from the inflammatory injury in the initial postoperative period. As a consequence, processes leading to central sensitization may occur, setting the stage for increased postsurgical pain and an increased requirement for analgesics. 7,11,12 Indeed, pain following CAS may be severe, as judged by clinical studies reporting that some 35% of patients needed morphine for postoperative pain relief, 6,8 the median time to first analgesia having been as early as 45 minutes after surgery. 8
The results of the present study support the concept of preemptive analgesia in the broad sense by which the effective blockade of noxious stimuli, generated during surgery and during the initial postoperative period, reduces subsequent pain by preventing altered sensory processing of afferent input on both the peripheral and the central level. 7,11 This advantageous effect would outlast the pharmacologic duration of action of the analgesic concerned. 22 Ketorolac, given intravenously 30 minutes prior to surgery, significantly reduced not only VRS pain scores but also the number of patients requiring acetaminophen and tramadol and the total analgesic consumption within the 6-hour period after completion of surgery, which approximates 8 hours after its administration. This indicates that some postoperative pain has been preempted, given that the usual clinical duration of the analgesic effect after a single ketorolac dose is about 6 hours. 23 Preemptive analgesia induced by ketorolac may be attributed primarly to its well-documented peripheral anti-inflammatory effects, although central mechanisms of action may also be involved. 24
The results of clinical trials regarding the value of NSAIDs in achieving preemptive analgesia are controversial. 25 Broad preemptive effects were reported by some authors 26–29 but denied by others. 30,31 The limitation of NSAIDs as preemptive analgesic agents arises from the difficulty in establishing objective, effective analgesic levels prior to surgical trauma. 12 In the current study, however, the reduced VRS pain score and the need for additional analgesia during surgery in patients who received ketorolac preoperatively compared with those who had received placebo suggest that ketorolac, as an adjunct to CPB, established an effective preincisional analgesic state.
With respect to primarily peripheral mechanisms of NSAID action, we administered ketorolac 30 minutes before surgery to allow sufficient time for it to reach the surgical field and preclude the de novo synthesis of prostaglandins by cyclooxygenase inhibition. This is in agreement with other studies supporting the preemptive analgesic efficacy of NSAIDs. 32,33
As is the case with any NSAID, the potential for surgical site or gastrointestinal bleeding is of particular concern, although only a modest prolongation in bleeding time (within the normal range in almost all patients) had been reported following ketorolac administration. 34 It has been suggested that the stress of surgery may, in fact, raise platelet function and counteract the decrease in platelet aggregation owing to ketorolac. 35 In a retrospective postmarketing surveillance that included more than 20,000 patients, a slightly increased risk of gastrointestinal bleeding, but not of surgical bleeding, was reported in patients who received ketorolac compared with those receiving opioids. 36 However, the risk of serious gastrointestinal adverse effects with NSAIDs, including ketorolac, seems to be very low after short-term perioperative use. 37 A single dose of the drug is unlikely to have a significant risk, although in this study, for safety reasons, we excluded patients at risk of adverse events related to NSAID administration. In our patients, excessive wound bleeding and gastrointestinal, renal, or other complications were not observed in the ketorolac group or in the placebo group.
In conclusion, a single 30 mg dose of ketorolac, administered intravenously 30 minutes before surgery, reduces the need for additional analgesia and sedation and preempts postoperative pain in patients undergoing CAS under CPB. The technique is simple and easy to perform, has minimal side effects, and improves patient comfort. However, with respect to potential adverse events related to NSAID administration, a precaution is necessary when selecting patients for the above-mentioned analgesic treatment.