
Abstract
The purpose of this study was to assess the safety of continuous subcutaneous therapy with treprostinil sodium (Remodulin), a prostacyclin analog, and its effect on ischemic rest pain and ischemic wound healing in subjects with critical limb ischemia (CLI) and no planned revascularization procedure.
This was a 12-week, open-label, single-center pilot study enrolling 10 subjects (mean age 82.4 years) with Fontaine stage III to IV (Rutherford class 4–6) peripheral arterial disease and ankle brachial indices less than 0.55. The primary end point was safety, and the secondary end points were the effects of treatment on ischemic rest pain, limb salvage, and wound healing.
There was a 62% reduction in mean worst rest pain and a 57% reduction in mean average rest pain at week 12, with most subjects using less pain medication. Three subjects experienced complete healing of their wounds. No subject developed a new wound during the trial. Treprostinil was generally well tolerated. Subcutaneous infusion-site pain was the most frequently reported side effect, with one subject withdrawing from the study as a result. Jaw pain was reported by two subjects. One subject experienced two serious adverse events considered unrelated to treprostinil (cholecystitis and congestive heart failure).
This study demonstrates that chronic, continuous subcutaneous treprostinil is safe and can be useful in the treatment of ischemic pain and wounds in subjects with CLI. Future controlled studies are needed to evaluate these effects and determine appropriate patient selection.
Treatment options are limited for patients with chronic critical limb ischemia (CLI), a life-and-limb threatening condition that may be present in 1% of the general population over 50 years of age. 1,2 The diagnosis of CLI requires the presence of pain at rest in the foot and toes that occurs when the leg is elevated, requires daily analgesia, and can be relieved when the leg is placed in a dependent position (Fontaine stage III or Rutherford class 4). Advanced CLI can also lead to nonhealing ischemic ulcer(s) and/or gangrene (Fontaine stage IV or Rutherford class 5 and 6). 1,3 Arterial bypass surgery or an endovascular procedure such as percutaneous transluminal angioplasty is the treatment of choice for these patients. However, many patients are not candidates for these procedures owing to their advanced age, comorbidities, and other factors. 4
There are no approved pharmacotherapeutic interventions for CLI. Two oral drugs currently approved in the United States for the relief of intermittent claudication have been used outside labeling in CLI: pentoxifylline (Trental), a hemorrheologic agent, and cilostazol (Pletal), a phosphodiesterase III inhibitor. 2,5 However, there are no large randomized studies supporting their use or efficacy in the CLI population.
Prostanoids have long been proposed as pharmacotherapeutic agents in the early stages of peripheral arterial disease (PAD), as well as in CLI. Controlled and uncontrolled trials of prostanoids, particularly prostaglandin (PG)E1 and PGI2 (prostacyclin) and their analogs, have produced evidence of rest pain relief and wound healing since the 1980s. 4,6,7 In particular, intravenously administered prostacyclin and prostacyclin analogs such as iloprost have been under study for more than 10 years in Europe, where intravenous iloprost is a commonly used therapy in CLI patients in some countries. 8,9
Based on the European experience, the TransAtlantic InterSociety Consensus (a group of US and European cardiovascular societies) concluded that “Patients who have a viable limb in whom revascularization procedures are impossible, carry a poor chance of success or have previously failed, and particularly when the alternative is amputation, may be treated with prostanoids.” 4 However, a major limitation of prostanoid therapy has been the relatively short half-life of these agents, which requires the intravenous route of administration.
Treprostinil sodium (Remodulin) is a chemically stable analog of prostacyclin with an elimination half-life of approximately 4.5 hours. 10 Treprostinil was approved in the United States in May 2002 for chronic, continuous subcutaneous infusion in patients with pulmonary arterial hypertension and, more recently, for chronic intravenous infusion via a central venous catheter. 10,11 In a small acute study, intravenous treprostinil was well tolerated in subjects with severe claudication. Treprostinil was administered intravenously in escalating doses until dose-limiting side effects were observed in eight subjects (age range 56–78 years), followed by a 2-hour maintenance infusion. All of the subjects were hypertensive, five were diabetic, and half had established coronary artery disease. Treprostinil at the maximum well-tolerated doses of 10 to 20 ng/kg/min produced potentially clinically significant increases in lower limb blood flow in serial ultrasonography (blood velocity and flow), segmental arterial pressure, and pulse volume recording assessments in these subjects. 12
Treprostinil has not previously been tested chronically in patients with CLI. Given the results of the acute trial and the extensive literature describing the use of prostacyclin and its analogs in CLI, a pilot safety and dose range-finding trial evaluating chronic subcutaneous treprostinil in subjects with CLI and no planned vascular interventional procedure was conducted.
Methods
This was a 12-week, open-label, single-center pilot study to evaluate the safety and efficacy of continuous subcutaneous administration of treprostinil in subjects with CLI and no planned vascular interventional procedures. Another objective of the study was to determine a safe dose of chronic treprostinil in these subjects. The planned enrolment was 10 subjects. The study was conducted at the Southern Arizona Vascular Institute in Tucson, Arizona, between October 2003 and October 2004.
Approval for the study was obtained through Western Institutional Review Board, Olympia, Washington. All subjects were to have Fontaine stage III to IV or Rutherford class 4 to 6 disease and ankle brachial indices (ABIs) from 0 to 0.55 in the most affected limb or the limb containing the reference ischemic wound for wound healing assessments.
Subjects were excluded from the study if they had had vascular surgery or vascular procedure within 30 days of study entry, were hemodynamically unstable, and had acute renal failure; acute pulmonary failure; a history of recent intracranial bleeding, gastric bleeding, urinary tract bleeding, or significant trauma within 6 weeks; a life-threatening malignancy requiring aggressive chemotherapy; end-stage renal disease; or chronic renal dialysis. Any condition or abnormal laboratory value that, based on information in the treprostinil package insert, would constitute an unacceptable risk to the subject's safety, was also an exclusion criterion. Subjects could not have been in an investigational trial within the past 30 days or been a nonresponder to chronic prostanoid treatment in the past 30 days.
Medications for comorbid disorders, such as coronary artery disease, diabetes, hypertension, and/or chronic lung disease; normal wound care, including débridement and antibiotics; and analgesics for rest pain were permitted during the study but were not to be changed from the baseline regimens unless clinically necessary.
After the completion of baseline assessments, treprostinil therapy was initiated in the clinic. Subjects were observed for at least 2 hours following the start of the infusion. Subjects and/or a caregiver were trained to administer treprostinil on an outpatient basis using an ambulatory subcutaneous infusion pump (Model 407C, Minimed, Sylmar, CA). Each subject was to be initiated at a dose of 2.5 ng/kg/min or lower, with the dose titrated based on tolerability. Dose increases were to be 1.25 to 2.5 ng/kg/min per week. The maximum allowed dose was 15 ng/kg/min, and the minimum allowed dose was 0.625 ng/kg/min. The subjects were instructed to change the subcutaneous infusion site every 3 days.
Subjects returned to the clinic for assessments at weeks 2, 6, and 12. Treprostinil treatment was terminated by gradually decreasing the infusion rate (over a period of 1 to 4 hours) after the week 12 visit assessments were completed.
Safety Assessments
Safety was assessed in all subjects using adverse event and physical examination findings. Signs and symptoms of CLI were not considered to be adverse events unless found to be different in causality, intensity, or frequency.
Rest Pain Assessments
Rest pain was assessed in all subjects using a visual analog scale for rest pain. The subjects were asked to rate their foot pain on a scale of 0 to 10, with 0 reflecting no pain and 10 reflecting the worst pain. The scale was printed, and the subjects were asked to place a mark on the number that reflected their pain experience. Subjects were asked to rate the worst pain they had experienced since the previous assessment and their average pain during that time frame. Analgesic medication use was assessed by the investigator as unchanged, increased, decreased, or discontinued.
Wound Assessments
All 10 subjects had at least one ischemic wound at baseline. If the subject had multiple ischemic wounds, then one or two (usually the largest or most severe wounds) were to be selected as reference wounds. Selected wounds were photographed for documentation. When possible, the outside edge of the wounds was traced for area measurements (cm2). The tracings were used to calculate wound area by measuring the length and width of the wound. The wounds were described and photographed for documentation and were assessed for overall status compared with baseline (ie, worse, slightly worse, unchanged, slightly improved, improved, or healed) at study visits.
In subjects who had wounds other than those chosen as reference wounds, the overall status (ie, worse, the same, improved, or healed) of each additional wound was documented at each study visit. New wounds that occurred during the study were also documented.
Results
Safety
Ten subjects (four males) were enrolled in the study after written consent. The mean age was 82.4 years and ranged from 65 to 90 years. Eight subjects had established coronary artery disease, four were diabetic, and three had chronic renal insufficiency. All subjects had diffuse PAD, with a mean ABI of 0.37 ± 0.06 (standard error of measurement [SEM]) of the worst limb. Six subjects had bilateral limb involvement. One subject had a previous below the knee amputation owing to PAD. This subject's remaining limb had an ABI of 0.62, slightly above the allowed maximum of 0.55, but was allowed to participate in the study. Three subjects had a history of failed bypass grafts, and one subject had a failed angioplasty. All subjects met the criteria for Fontaine stage IV (Rutherford class 5 or 6) disease with ischemic rest pain and at least one ischemic limb wound. Table 1 summarizes the relevant characteristics.
Patients' Characteristics and Comorbidities
ABI = ankle brachial index.
All subjects received subcutaneous treprostinil at an initial dose of 2.5 ng/kg/min of the study drug. Nine subjects were titrated to the maximum dose of 15 ng/kg/min between weeks 1 and 6, whereas one subject elected to stay at 7.5 ng/kg/min.
Nine of the 10 subjects in the study experienced an adverse event. There were two serious adverse events, both in the same subject. The subject developed cholecystitis, resulting in a laparoscopic cholecystectomy at week 10. Treprostinil infusion was not discontinued during the procedure. At week 12, the same subject experienced worsening congestive heart failure, requiring diuretics and the addition of an angiotensin-converting enzyme inhibitor to her medication regimen. Both serious adverse events were judged unlikely to be related to treprostinil.
All of the other adverse events were well-characterized side effects of treprostinil: infusion-site pain (eight subjects), jaw pain (two subjects), headache (one subject), and diarrhea (one subject). One subject who had severe infusion-site pain, jaw pain, headache, and diarrhea withdrew from the study at week 6. Infusion-site pain and jaw pain limited the treprostinil dose to 7.5 ng/kg/min in one subject, who completed the study at that dose.
There was one other discontinuation from the study that was unrelated to any adverse event. This subject discontinued at week 6 because she felt overwhelmed by the pump and the infusion-site change requirement.
Rest Pain
The baseline mean worst and mean average ischemic rest pain scores were 8.1 ± 0.4 (SEM) and 6.9 ± 0.3, respectively. At week 12, the mean worst and mean average ischemic rest pain scores were 3.1 ± 0.8 and 3.0 ± 0.7, respectively. The reduction in the mean worst rest pain from baseline to week 12 was 62%. The reduction in the mean average rest pain from baseline to week 12 was 57% (Figure 1). Baseline data are for all 10 study subjects, whereas week 12 data are for the eight subjects who remained in the study through week 12.
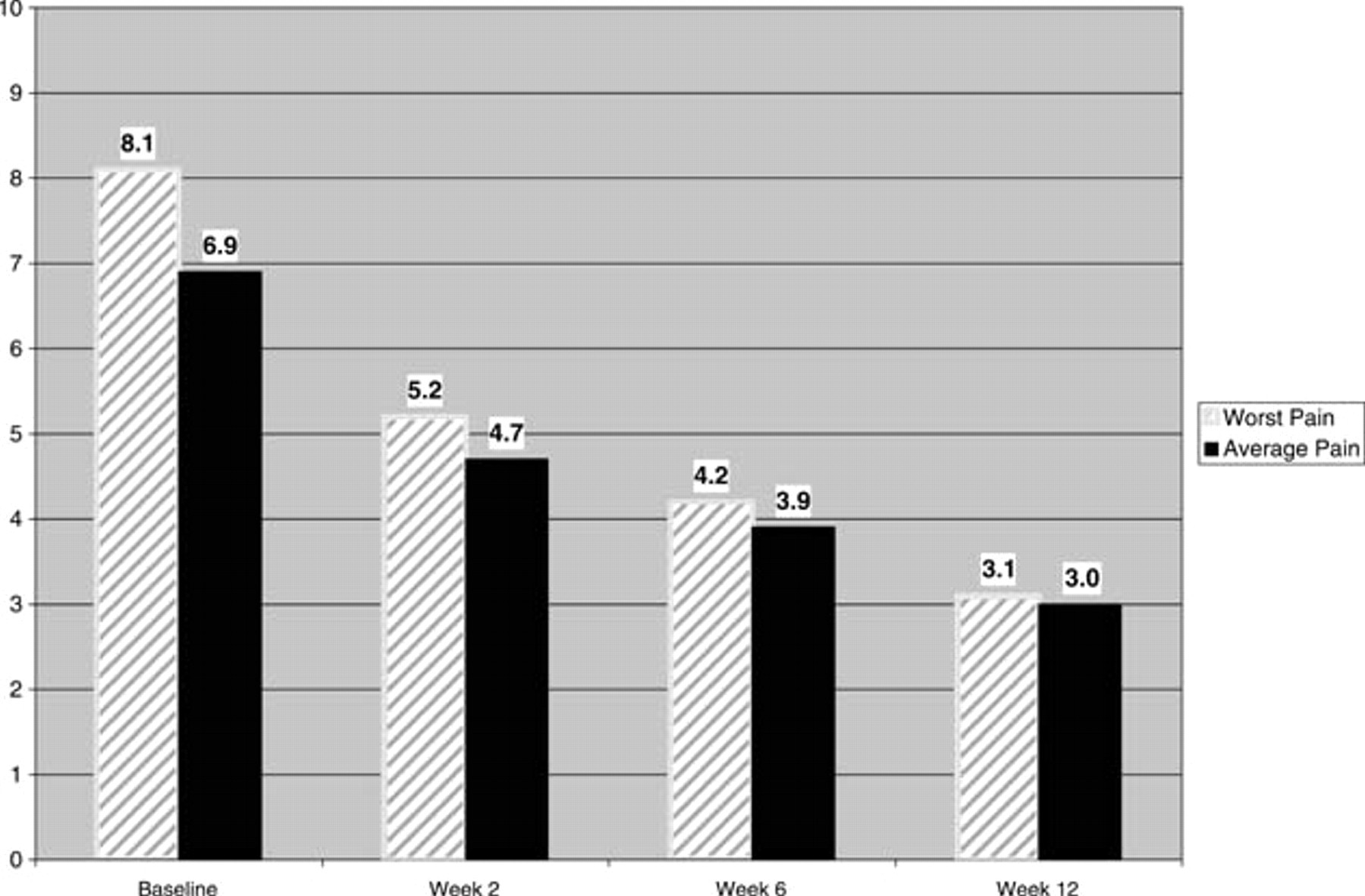
Mean pain scores. Scale: 0 = no pain, 10 = worst pain. n = 10 for baseline, week 2, and week 6. n = 8 for week 12; two patients withdrew from the study prior to the week 12 visit.
Follow-up rest pain data after study drug termination were obtained for only three subjects. In two of these subjects, average and worst pain had returned to baseline levels 8 weeks after termination of the study drug. In the third patient, average and worst rest pain scores 8 weeks after termination of the study drug remained improved compared with baseline and were similar to the week 12 scores.
At week 12, seven of the eight subjects who completed the study had decreased their pain medication use compared with baseline. Two of these subjects experienced complete ischemic pain relief and discontinued pain medication. Five of the 10 subjects were using less pain medication at week 6. The subject who withdrew from the study because of infusion-site pain had experienced complete ischemic pain relief and had discontinued pain medication at week 6 but resumed taking pain medication 1 week after discontinuing treprostinil.
Wounds
Baseline wounds varied in location, extent of tissue loss, and degree of gangrene or necrosis (Table 2). The condition of the reference wounds was evaluated by the investigator as worse, unchanged, improved, or completely healed compared with baseline.
Ischemic Wound Descriptions
The duration of wounds at baseline varied from 1 to 9 months. Wound size at baseline ranged from 0.2 to 63.8 cm2. Three subjects (cases 1, 2, and 3) with small wounds (0.2–2.0 cm2) that had been open for 1 to 12 months experienced complete healing of their wounds. No new wounds developed during the trial. Brief case reports for three subjects who experienced complete healing are presented below. A fourth case report is presented that represents novel use of a prostacyclin analog. In this subject, treprostinil was used to delay amputation to allow the subject to complete rehabilitation for a fractured hip on the endangered limb.
Three subjects went on to have below the knee amputations as a result of progressing wounds within 2 months following completion of the study. These subjects had been offered amputation as an option prior to starting the trial and chose to participate in the hope of salvaging the limb.
Case Reports
Case 1
Subject 5 is an 88-year-old female with peripheral vascular disease. An angiogram showed a completely occluded left superficial femoral artery (SFA) with collaterals reconstituting the left popliteal artery. Her ABI at baseline was 0.30. She had a small ischemic ulcer on the left second toe for 2 months that measured 0.16 cm2 and could be probed to the bone. A magnetic resonance angiogram (MRA) noted osteomyelitis of the left second toe. She had complete wound closure at week 6. Although her rest pain did not resolve completely, she changed from hydrocodone bitartrate and acetaminophen to propoxyphene and acetaminophen. Her final treprostinil dose was 15 ng/kg/min.
Case 2
Subject 7 is an 88-year-old female who presented with nonhealing ischemic wounds on the right and left third toe following toenail removal 4 weeks prior to baseline. She had bilateral renal angioplasty in 2003. An arteriogram was deferred owing to her renal status and creatinine level of 2.7 mg/dL. An MRA showed diffuse infrainguinal disease with two-vessel runoff to the foot. She was unable to walk any distance without leg pain and experienced severe ischemic rest pain at baseline. Her ABIs at baseline were 0.40 on the right and 0.36 on the left. At week 6, she had complete resolution of her rest pain, was able to walk without restrictions, and discontinued narcotic pain medication. At week 12, she had complete wound closure. Her treprostinil dose was 7.5 ng/kg/min.
Case 3
Subject 10 is a 65-year-old male with a 13-year history of PAD, as well as insulin-dependent diabetes, chronic renal insufficiency, and congestive heart failure. He had a right femoropopliteal bypass in 1991 and documented occlusion 5 months later. He has had repeated neuropathic ulcerations of the right great toe that have never fully resolved since 2001 in the presence of PAD. He participated in a previous trial of another prostanoid in late 2001 and demonstrated improvement in the ulcer at the completion of the trial, but it is unknown if he was on placebo or the active drug. He began experiencing ischemic rest pain in his right leg in 2003. At baseline, he had a nonhealing ulcer on his right great toe for 9 months measuring 1.96 cm2. He completed 12 weeks of treprostinil and showed early wound healing, with complete wound closure at week 12. He also experienced complete resolution of his ischemic rest pain and severe claudication at week 2 and discontinued his narcotic pain medications. His treprostinil dose was 15 ng/kg/min.
Case 4
Subject 3 is an 82-year-old male with a history of oxygen-dependent chronic obstructive pulmonary disease, atrial fibrillation, hyperglycemia, anemia of unknown origin, and multilevel vascular disease. His vascular disease history includes transient ischemic attacks, carotid endarterectomy in 1995 and 2003, coronary artery disease, coronary artery bypass in 1995, and documented PAD since 2002. He broke his left hip in August 2003 and developed left heel and leg ischemic ulcers while in a rehabilitation facility. A sonogram in November 2003 demonstrated distal right SFA stenosis, proximal left SFA occlusion, and mid-SFA occlusion with large collaterals. Minimal arterial flow was seen at the ankle level with toe pressure less than 40 mm Hg. The right ABI was 0.58 and the left ABI was 0.25. The subject had two large ischemic wounds with extensive tissue loss located on the left heel (63.8 cm2) and left lateral leg (40.2 cm2). There was concern that the subject would be unable to use a prosthetic limb following an amputation in the presence of the recent hip fracture and incomplete healing of the prosthetic hip. He was enrolled in the study to attempt to stabilize the wounds, provide rest and pain relief, delay amputation, and continue the rehabilitation of the left hip. His wounds remained stable during the 12 weeks of drug treatment, with no significant improvement but no worsening. Average rest pain scores were 7 at baseline and reduced to 4 at week 12. Worst rest pain scores reduced from 8 at baseline to 4 at week 12. He reduced his consumption of pain medicine from hydrocodone bitartrate–acetaminophen and oxycodone to oxycodone hydrochloride–acetaminophen alone. He completed the 12 weeks of the study and was able to complete rehabilitation of his left hip. It is anticipated that he will be able to use a prosthetic limb as a result of the delayed amputation and increased rehabilitation time.
Discussion
This is the first study evaluating chronic, continuous subcutaneous infusion of treprostinil sodium, a long-acting prostacyclin analog, in subjects with severe CLI. We found that treprostinil at a dose of 15 ng/kg/min is generally safe and well tolerated in this population, reduces ischemic rest pain, and may help heal ischemic wounds.
All 10 subjects reported improvement in rest pain as early as week 2 (when the treprostinil dose was approximately 5 ng/kg/min in most subjects). Mean pain scores continued to decline by week 6 as the treprostinil dose increased to the maximum dose of 15 ng/kg/min in most subjects. Overall, there was a decline in pain of approximately 60% at week 12 compared with baseline. This finding needs to be confirmed with more accurate methods such as patient diaries or validated pain scales, such as the Short Form McGill Pain Questionnaire, in future controlled trials.
The pain relief was accompanied by a clinically meaningful reduction in pain medication use in most subjects, with complete discontinuation of pain medications in two patients. Since CLI patients often have diminished renal function in addition to their cardiovascular disease that may limit the use of nonsedating medications such as nonsteroidal anti-inflammatory drugs, narcotics are frequently prescribed. Narcotics are effective in relieving ischemic rest pain, but the side effects of dizziness, drowsiness, and impaired mental and physical performance may increase the risk of falls or exacerbate cognitive problems in these patients. Any intervention that allows a potential reduction in narcotic use may be clinically useful in terms of improved safety for the patient. Further, two subjects spontaneously reported improved ambulation, and another subject spontaneously reported improved sleep during the study. Taken together, these findings may suggest meaningful improvements in quality of life with the use of treprostinil, which should be confirmed using a validated assessment, such as the Short Form 36 Health Survey (SF-36) instrument, in a controlled trial.
The wound healing results observed in this trial also suggest that there is a rationale for future controlled studies with careful patient and baseline wound selection and standardized wound care. This pilot trial did not limit the size or location of wounds to be assessed, and baseline wounds were quite variable in size (from 0.2 cm2 to 63.8 cm2) and the degree of necrosis and/or gangrene. Given the findings in this report—complete healing of small wounds in three subjects—and positive data with intravenous prostanoids in previous work, 4,8,9,12 there may be a role for treprostinil in ischemic wound healing in CLI patients. Continuous subcutaneous administration of treprostinil was clearly manageable for these subjects in an outpatient setting. If larger wounds are to be treated, more aggressive dosing and a longer duration of treatment should be considered. Future trials could also include skin perfusion and ultrasound measurements to extend previous work in patients with lower limb ischemia 12 and provide information about the mechanism of action.
Limitations
This was an open-label, nonrandomized study of relatively short duration with a small number of subjects with a disease that has few pharmacologic options. No statistical inference can be made regarding the efficacy of treprostinil in the treatment of CLI.
Conclusion
This open-label study supports the safety of chronic subcutaneous treprostinil infusion in patients with CLI. Ischemic pain and wounds are the primary management problems in patients with CLI. Treprostinil appeared to provide pain relief in all subjects and may have contributed to complete wound healing in three subjects. Treprostinil may be useful in the treatment of ischemic pain and ischemic wounds in patients with CLI. Future controlled studies are needed to evaluate these effects and determine appropriate patient selection.
Footnotes
Acknowledgments
We thank Courtnay Buonomo for her assistance with the preparation of the manuscript.
Medication, infusion pumps, infusion supplies, and administrative support were provided by United Therapeutics Corporation.