
Abstract
Surgical bypass represents one of the chief treatment modalities for peripheral arterial occlusive disease. Despite improving techniques, graft occlusion accounts for the majority of these bypass failures. Once occluded, however, these grafts are thought to rarely pose a threat for future ischemic events. This report describes two patients with previously thrombosed grafts who subsequently presented with limb-threatening ischemia owing to peripheral embolization from the graft.
Two patients with occluded grafts presented with ipsilateral limb-threatening acute ischemia. Both of these patients developed severe acute limb-threatening ischemia weeks to months after known graft thrombosis. Arteriography revealed peripheral embolization in each case. Both patients were operated on for disconnection of the thrombosed graft from the native circulation and have been free of recurrent symptoms.
The occluded graft, although generally innocuous, can be a source of peripheral emboli, resulting in peripheral embolization and acute limb ischemia. Both patients in this report developed limb-threatening ischemia owing to embolization from the cul-de-sac of occluded prosthetic grafts. Due to the rarity of the condition and its associated morbidity and mortality, awareness and recognition of this phenomenon are critical. Operative disconnection is recommended if the embolism occurs downstream of the graft and no other embolic source can be identified.
Peripheral arterial occlusive disease continues to be a major cause of morbidity and mortality affecting our aging population. In addition to controlling several common contributing cofactors, such as hypertension, diabetes mellitus, smoking, and hyperlipidemia, surgical revascularization continues to occupy the mainstay of our treatment regimen. Despite improvements in technical skills and resultant patency, a finite failure rate for arterial reconstructions remains. 1 Once occluded, however, these grafts are considered to be inert entities that are left in place owing to a higher morbidity as a result of explantation.
Acute limb ischemia is a clinical entity that results in significant limb loss and mortality. The incidence of acute limb ischemia is about 1.7 in 10,000, with an associated limb loss rate of 8 to 22% and a subsequent 1-year mortality rate of 10 to 17%. 2 Acute limb ischemia may be due to atheroembolism from the aortoiliac system or it may be due to embolism from the heart. In situ thrombosis of an existing stenosis may also result in acute limb ischemia. In cases of embolization, 80% will originate in the heart and 10% will originate in the arterial or venous system, and in 10% of cases, a source cannot be identified. 3–5 This report describes two such patients in whom the cause of acute limb ischemia appears to have been embolization from a thrombosed graft.
Case Report
The following report describes two cases in which patients who had previously undergone revascularization for chronic ischemic symptoms proceeded to graft occlusion. Weeks to months after a documented graft thrombosis, both patients experienced acute limb ischemia in the ipsilateral extremity. These patients underwent appropriate investigations to try to ascertain a possible source of the embolus. They underwent a negative hypercoagulable workup consisting of factor V Leiden mutation, proteins C and S, antithrombin III, homocysteine, anticardiolipin antibodies, lupus anticoagulant, and prothrombin gene mutation. In both patients, a full workup, including echocardiography; computed tomography of the chest, abdomen, and pelvis; arteriography; and appropriate blood tests was performed and was unrevealing as far as a potential source of the peripheral embolization.
Patient 1 is a 75-year-old woman who presented in December 2001 complaining of severe bilateral calf claudication, which she found disabling. She had a medical history significant for hypertension, diabetes mellitus type 2, coronary artery disease with a previous myocardial infarction, and hyperlipidemia. On examination, she had normal femoral pulses bilaterally and absent popliteal and pedal pulses.
After an attempt at conservative nonoperative therapy, she still continued to be significantly limited by her claudication and decided to undergo surgical therapy. An arteriogram revealed bilateral superficial femoral artery occlusion beginning at the orifice with reconstitution of her above the knee popliteal arteries. She underwent right femoral to above the knee popliteal bypass with 6 mm nonsupported polytetrafluoroethylene (PTFE) in September 2002 followed by left femoral to above the knee popliteal bypass with 6 mm nonsupported PTFE in January 2003, with resolution of all claudication symptoms. In December 2003, she returned with complaints of recurrent right calf claudication. A duplex sonogram confirmed thrombosis of her right femoropopliteal graft, and because her symptoms were only 2 days old, catheter-directed thrombolysis was successfully attempted. No underlying anatomic cause of graft failure, including anastomotic stenosis, was identified after lytic therapy was completed. She was placed on oral anticoagulation with warfarin with a goal international normalized ratio of 2.0 along with one aspirin (325 mg) per day in an attempt to maintain graft patency. She had complete resolution of her claudication at this time. In February 2004, she presented again with complaints of recurrent right calf claudication that was similar in severity to her presenting complaints. Duplex ultrasonography at that time confirmed repeat thrombosis of her right femoropopliteal graft. At that point, it was decided not to try to reopen this graft given that she had stable claudication with no evidence of advanced ischemia.
In March 2004, 1 month after known graft thrombosis, she presented to the emergency department with a cool, pulseless right leg. The foot was acutely ischemic, and an arteriogram at that time reconfirmed occlusion of her right femoropopliteal graft with evidence of embolization to her right profunda femoris artery (Figure 1). She underwent operative exploration, which revealed evidence of a fresh thrombus both embolized to her profunda femoris artery and at the orifice of the occluded graft. This proximal thrombus was intimately attached to the more organized thrombus in the mouth of the PTFE graft with an interface certainly suggestive that the profunda femoris thrombus was a fresh embolism of the thrombus in the clotted graft. A thrombectomy of the profunda femoris artery was performed with disconnection of the proximal graft anastomosis from the native circulation and patch angioplasty of the common femoral artery. It should be noted that at the time of presentation, a diligent search for alternative etiologies was undertaken and none were found. The patient had no onset of any arrhythmias or signs of a new cardiac event. An echocardiogram revealed good left ventricular function and no evidence of mural thrombus or valvular vegetations. Since her operation, she has had no recurrent events.

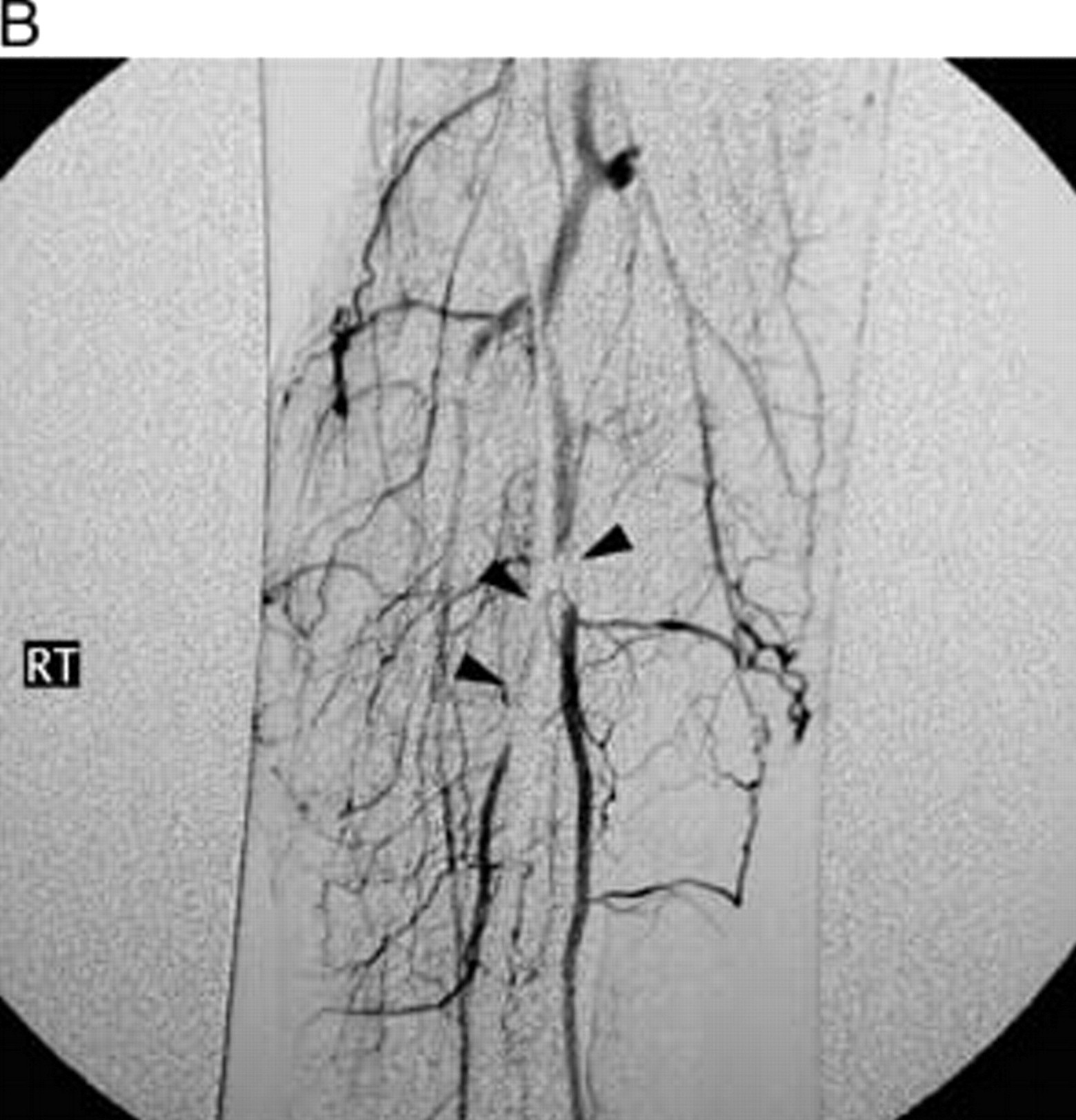
A, This right lower extremity arteriogram of a patient with an occluded right femoropopliteal graft reveals occlusion of the right common femoral artery at the level of the anastomosis (arrowhead), with thrombus from the graft extending into the native arterial lumen (arrow). B, Distal runoff showed evidence of embolism at the level of her profunda femoris artery (arrow) leading to an ischemic right lower extremity. She underwent a profunda femoris artery embolectomy with disconnection of the graft from the native circulation, which has prevented further embolic events.
Patient 2 is an active 51-year-old male who presented in 1998 with a 3- to 4-month history of worsening right calf claudication. His medical history was significant only for an 8-pack-year smoking history. On examination, this patient had a palpable mass in the right popliteal fossa with weak pedal pulses. After workup, he was diagnosed with popliteal cystic adventitial disease and underwent en bloc resection with reconstruction of the right popliteal artery with a greater saphenous vein interposition graft in 1998. The patient remained symptom free until January 2000, when he presented with recurrent right calf claudication. An angiogram at that time revealed moderate stenosis at the proximal and distal anastomoses of the vein graft, and angioplasty was attempted to increase distal perfusion. After this intervention, however, his right calf claudication continued to worsen. In August 2000, he then underwent an above to below the knee popliteal artery bypass with 8 mm PTFE based on a concern that the saphenous vein was not of adequate caliber, especially in a younger man who was very physically active. Following this procedure, he was free of calf pain and was able to return to his daily activities. In April 2002, he presented to the emergency department with acute onset of persistent right calf pain. On examination, he had a cool right calf and foot with absent pedal pulses. An angiogram at that time revealed occlusion of his PTFE popliteal bypass, patency of his vein interposition graft, and a filling defect of the anterior tibial artery consistent with embolism (Figure 2A). He was treated with catheter-directed thrombolysis, resulting in dissolution of the embolus with resolution of all symptoms. The patient was discharged on one aspirin (325 mg) per day. Unfortunately, he presented to the emergency department in December 2002, 8 months after known graft thrombosis, again complaining of the acute onset of persistent right calf pain. The angiogram at that time revealed a filling defect, this time in the tibioperoneal trunk, consistent with embolism (Figure 2B). This was treated again with catheter-directed thrombolysis, with dissolution of the embolus and resolution of all symptoms. This patient subsequently underwent disconnection of both proximal and distal anastomoses of his above to below the knee popliteal bypass graft with patch angioplasty of the popliteal artery in January 2003 and has since been free of recurrent episodes of embolic acute right calf ischemia.
A, This right lower extremity arteriogram (a) of a patient with cystic adventitial disease after resection reveals occlusion of an above to below the knee popliteal bypass graft (arrow) with in-line flow through a previous saphenous vein interposition (arrowhead). He presented on two separate occasions with an ischemic right calf and foot. An arteriogram of his right calf runoff at the first episode (b) showed evidence of embolic occlusion of his anterior tibial artery, which was treated with thrombolysis with resolution of symptoms. B, A similar arteriogram at the time of the second episode revealed embolism to the level of the tibioperoneal trunk (arrowheads). This was treated with thrombolysis with subsequent disconnection of the above to below the knee popliteal artery graft from the circulation. He has since been free of recurrent ischemic episodes.
Discussion
Acute limb ischemia may result from embolism of thrombus from an occluded vascular graft into the native circulation. Despite its infrequency, this phenomenon has been reported in association with hemodialysis access procedures. Yang and colleagues reported a distal embolus occurring in association with an occluded upper extremity arteriovenous graft. 6 Their patient experienced acute hand ischemia 10 years after known graft thrombosis, suggesting that it may be associated with extrinsic compression of the graft. They did not recommend the routine disconnection of all such grafts. Lancombe reported distal embolization from aneurysmal degeneration of the arterialized vein segment of an arteriovenous fistula. 7
The phenomenon of distal embolization of thrombus from an occluded axillofemoral bypass has been well described. 8 McLafferty and colleagues and Mawatari and colleagues described the incidence of upper extremity embolism from occluded axillofemoral bypasses to be as high as 33 to 80%. 9,10 Both of these groups recommended routine disconnection of such grafts secondary to their high likelihood of embolization to the distal arterial tree. Khalil and Hoballah recommended disconnection of such grafts if associated with radiographic evidence of embolic potential on duplex ultrasonography and/or angiography. 11 In contrast to operative disconnection of these occluded grafts, Bandyk and colleagues recommended short-term anticoagulation with shoulder motion limitations after graft thrombosis in their series of three of five patients with distal embolization. 12 Elective surgical repair was recommended if duplex ultrasonographic studies revealed repairable defects in the axillary artery. Kallakuri and colleagues reported a two-patient series of upper extremity embolism from occluded axillofemoral bypass grafts successfully treated with endovascular embolectomy and occlusion of the graft stump with a covered stent. 13
Our case series represents the first report of distal embolization of thrombus from chronically occluded infrainguinal bypass grafts. Although distinctly unusual, this possibility must be kept in mind when assessing patients with peripheral embolization from an unknown source. All patients who present with evidence of embolic acute limb ischemia must undergo a full evaluation to determine the source of the embolus. In the event that a patient with peripheral embolization and acute limb ischemia has a negative embolic and hypercoagulable workup but an occluded vascular graft in the appropriate anatomic distribution, this graft should be considered a potential source of peripheral embolization.
In the case of patient 1, the phenomenon of an ascending thrombus resulting in occlusion of the common femoral artery bifurcation following the occlusion of a femoropopliteal graft has been described. Given that the profunda femoris in this patient was patent at the time of the embolic presentation, this case represents a patient who may have progressed to an ascending common femoral artery bifurcation thrombosis but experienced an embolic event from the ascending thrombus prior to complete bifurcation occlusion. The cause of proximal, ascending thrombosis after femoropopliteal graft failure frequently is anastomotic stenosis. This patient had no evidence of proximal anastomotic stenosis as the cause of graft failure. In cases in which an anastomotic stenosis is diagnosed, the preferred treatment would entail a femoral endarterectomy with arterial repair.
In this report, it is important to consider whether these embolic or ischemic events occurred acutely at the time of graft occlusion or at a later point, as we suggest, from a chronically occluded graft. Both of these patients experienced their ischemic event weeks to months after known graft thrombosis. Patient 1 had a time lapse of at least 1 month from known documented graft thrombosis to presentation with acute limb ischemia; during that interim period, she was experiencing calf claudication only. In regard to patient 2, it is not possible to clearly define the first episode of acute limb ischemia in relation to thrombosis of the PTFE graft. It should be noted that his saphenous vein interposition graft remained patent during this entire time period. It is, however, clear that the second episode of peripheral embolization occurred 8 months after documented graft thrombosis. At both times, the arteriogram clearly revealed the characteristic findings of peripheral embolization.
In both patients, the source of peripheral embolization was thrombus from an occluded prosthetic graft. The source of these emboli may be either the proximal or distal anastomosis. Therefore, in patient 1, the embolus occurred downstream of the proximal anastomosis only, and, as such, this proximal anastomosis was disconnected with repair of the common femoral artery. In the case of patient 2, both the proximal and distal anastomoses had in-line flow to the embolic distribution, and, as such, both anastomoses were disconnected because neither one in particular could be indentified as the source. Given the small number of patients, coupled with the rarity of this condition, it is not possible to identify whether the conduit type may have predisposed these patients to this complication.
The awareness and recognition of this phenomenon are important in preventing the recurrence of embolism and limb ischemia and, by extension, promoting limb preservation and survival. In the setting of acute limb ischemia secondary to peripheral embolization, in the appropriate anatomic distribution downstream of a known thrombosed graft, it may be prudent to disconnect the graft to exclude it from the circulation to prevent recurrent arterial thromboembolism. This disconnection of the thrombosed graft from the native circulation should be performed at any connection that has in-line flow with the embolus.