
Abstract
The objective of this study was to evaluate the existence of hemodynamic arterial flow correlation between preoperative duplex scanning (DS) and intraoperative direct outflow resistance (IDOR) measurements in ischemic lower limb revascularization.
Sixty-eight ischemic lower limbs were submitted to preoperative DS. Anatomic and hemodynamic arterial characteristics of the outflow system were recorded, and the results were considered in the distal anastomosis placement site decision making. IDOR measurements were obtained at the same arterial segment, and Pearson's correlation coefficient test was performed to study the preoperative DS power in predicting the intraoperative outflow resistance.
DS was technically satisfactory and helped define the distal anastomosis site in 93.2% of the cases (supragenicular popliteal artery, 19 [27.9%]; infragenicular popliteal artery, 10 [14.7%]; crural artery, 31 [57.4%]). A positive correlation could be found between preoperative DS and IDOR (0.450; p < .001). This correlation was particularly powerful in the crural artery (0.715; p < .001) when compared with the popliteal arterial segment (0.237; p = .192).
Preoperative DS may help define the best distal arterial and outflow segment to be revascularized based on anatomic and hemodynamic parameters. There is a positive flow correlation between preoperative DS and IDOR that seems to be stronger in crural revascularization surgery.
Ischemic lower limb revascularization has been extensively studied, and the surgical indications and techniques are well established. 1–3 Early graft failure has been reported in 5 to 25% of the cases. 4,5 The relatively high incidence of this complication mandates a more effective management regimen. It appears that optimization of the clinical decision to surgically intervene would be the right path to follow. 6,7 The quality of the distal vascular outflow is one of the most influential factors with respect to graft outcome. 8–10 Careful study of its characteristics can help define the best therapeutic option, 11,12 and preoperative contrast arteriography has been advocated as the mainstay outflow assessment test. Moreover, it has inherent limitations 13,14 and a low but significant complication rate and is costly. 15–17 Numerous tentative attempts to ameliorate its outflow prognostic capacity have been made, but the results have been inconsistent. 18,19 Various direct intraoperative methods have demonstrated the correlation between poor limb outflow and graft failure. 20–23 Ideally, this hemodynamic information would have to be obtained in the preoperative period if one would like to consider the outflow status in the surgical planning. Currently, duplex scanning (DS) has been proposed as the sole preoperative method in lower limb revascularization, 24–29 but its hemodynamic power in predicting the outflow status has never been reported. In this study, we evaluated the existence of hemodynamic correlation between preoperative DS and intraoperative direct outflow resistance (IDOR) measurements in ischemic lower limb revascularization.
Method
Between July 1999 and July 2004, 73 consecutive patients with critical limb ischemia (ischemic ulcer, rest pain, severe claudication) were included. Anatomic and hemodynamic arterial characteristics were studied by DS and were considered in the surgical strategy decision making.
DS was all carried out by an experienced and accredited vascular technologist team using an HDI 5000 color scanner (Advanced Technology Laboratories, Bothel, WA) and a combination of linear array transducers (4–7 MHz) to enable visualization of arteries at variable depths. Information obtained from B-mode, color-flow imaging and Doppler spectral analysis was used to compose a schematic lower limb arterial map. Possible ideal sites for distal surgical anastomosis placement were defined based on the anatomic and hemodynamic arterial characteristics, arterial internal diameter (ID), flow velocity (VEL-DS), and volume (VOL_DS) obtained at this site. For the VOL_DS calculation, the arterial ID was obtained in transverse section (media of three measurements) and longitudinal Doppler spectral analysis was obtained at the same site. We tried to ensure an angle of 60° between the Doppler beam and blood vessel axis. At this point, the scanner automatically calculated the blood flow by the following formula:

After ensuring a good inflow donor site and arterial substitute, the arterial segment chosen for distal anastomosis placement was surgically exposed. Intraoperative outflow resistance measurement was done by a simple and low-cost method previously demonstrated to be of positive graft patency prognostic value. 33,34 Before completion of the distal anastomosis, an indwelling catheter was placed distally after systemic heparinization and arteriotomy. A saline solution 500 mL bag was hung 120 cm above the arteriotomy site, and the system was connected to the previously described catheter. After 1 minute of infusion, the system was disconnected and the outflow volume (OV) infused annotated. The saline solution column remaining inside the infusion system was observed until it equalized that of the outflow arterial system pressure (OP), and its values were also annotated (Figure 1).
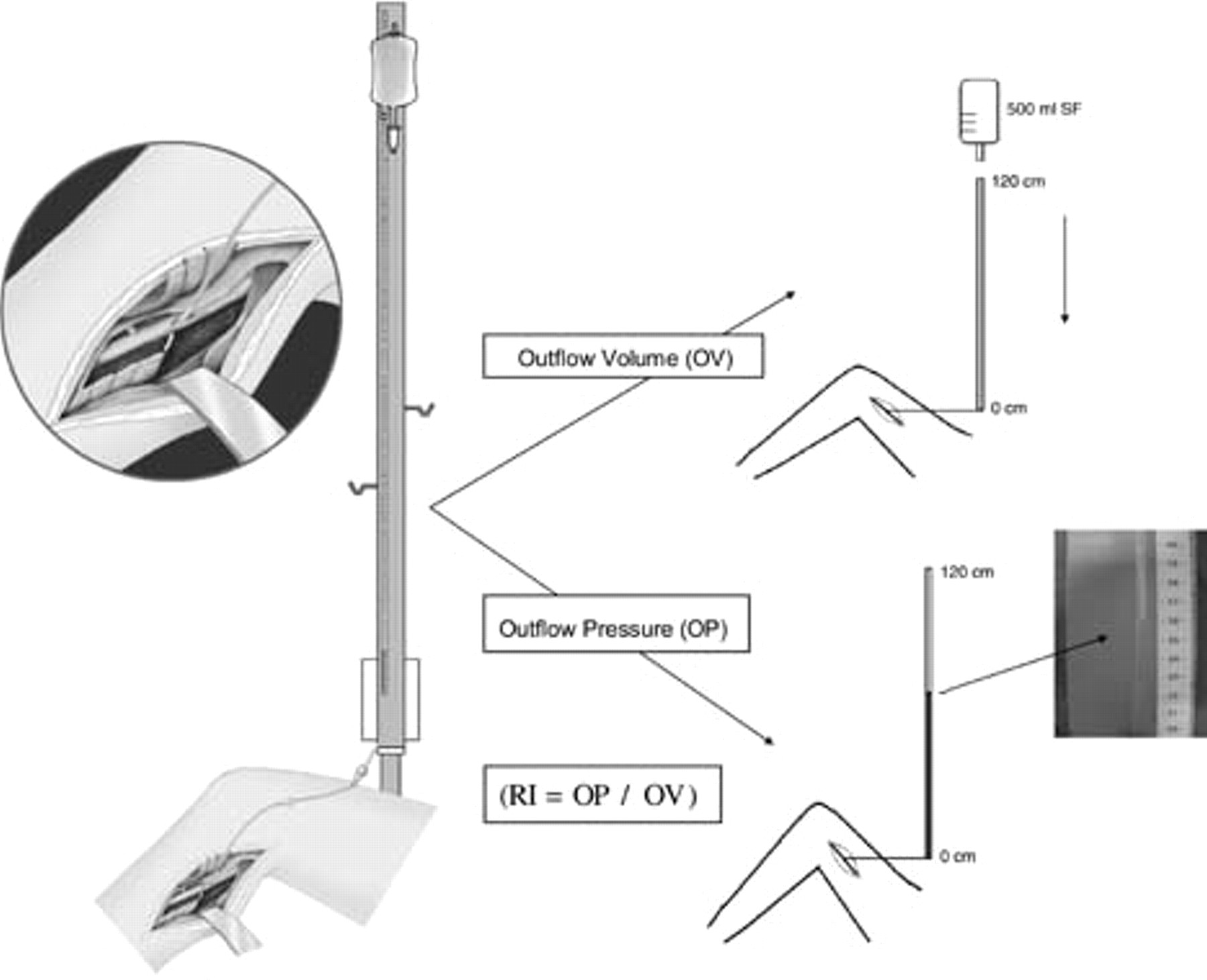
Intraoperative direct outflow resistance measurement method. OP = operative pressure; OV = operative flow volume; RI = operative resistance index.
Considering that the variables OP and OV have an inverse relationship, an outflow resistance index (RI) could be studied (RI = OP/OV). Distal anastomosis and completion arteriography were undertaken, and potential technical problems were corrected immediately.
For analysis of the preoperative hemodynamic DS power in predicting the intraoperative outflow resistance characteristics, the hemodynamic correlation between preoperative VEL-DS and VOL_DS and intraoperative OV, OP, and RI was assessed by Pearson's correlation coefficient test.
Results
Seventy-three consecutive patients with atherosclerotic chronic critical limb ischemia were included in this study. Five patients (6.8%) were excluded from the study because of failure to identify outflow arteries by DS (two cases, peroneal arteries were not visualized; two cases, severe limb infection and edema; one case, severe arterial wall calcification). Sixty-eight patients remained in the study; their demographic characteristics are listed in Table 1.
Patient Characteristics
Preoperative DS results and arterial anatomy were used to plan surgical strategy. Preferentially, autogenous grafts were used whenever possible and the bypass was made as short as possible. Forty-two (61.8%) patients received reverse and 7 (10.3%) patients in situ saphenous vein grafts. Polytetrafluoroethylene grafts were used in 19 (27.9%) patients.
Preoperative DS hemodynamic characteristics at the distal anastomosis arterial site are depicted in Figure 2.
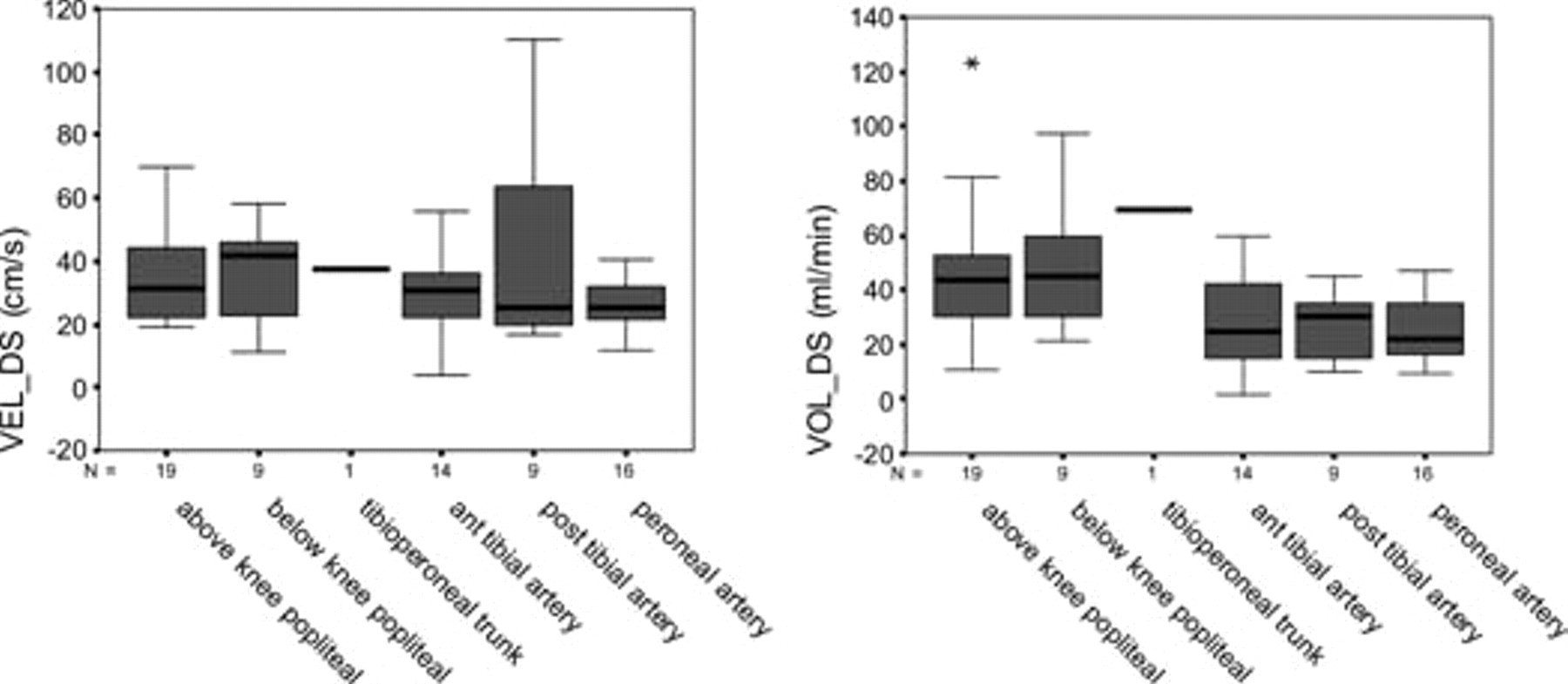
Duplex scanning outflow velocity (VEL-DS), and volume of flow (VOL_DS).
After surgical exposure and catheterization of the arteries as described above, intraoperative OV, OP, and RI characteristics are as demonstrated in Figure 3.

Intraoperative direct outflow resistance measurements. OP = operative pressure; OP = operative pressure; RI = operative resistance index.
Distal anastomosis and completion angiography were undertaken, and potential technical defects were corrected immediately.
Pearson's correlation coefficient index was not as strong when all cases were considered together. However, the correlation power varied with the distal anastomosis placement site. In above- or below-knee popliteal artery segments, this correlation was weak. Crural arteries demonstrated the strongest correlation index, particularly for preoperative VOL_DS and intraoperative OP (Table 2).
Pearson's Correlation Coefficient (p Value) between Preoperative Duplex Scanning and Intraoperative Outflow Resistance Measurement
OP = operative pressure; OV = operative flow volume; RI = operative resistance index; VEL-DS = duplex scanning velocity; VOL_DS = duplex scanning flow volume.
The correlation differences between popliteal and crural VOL_DS and OV can be better seen in Figure 4.
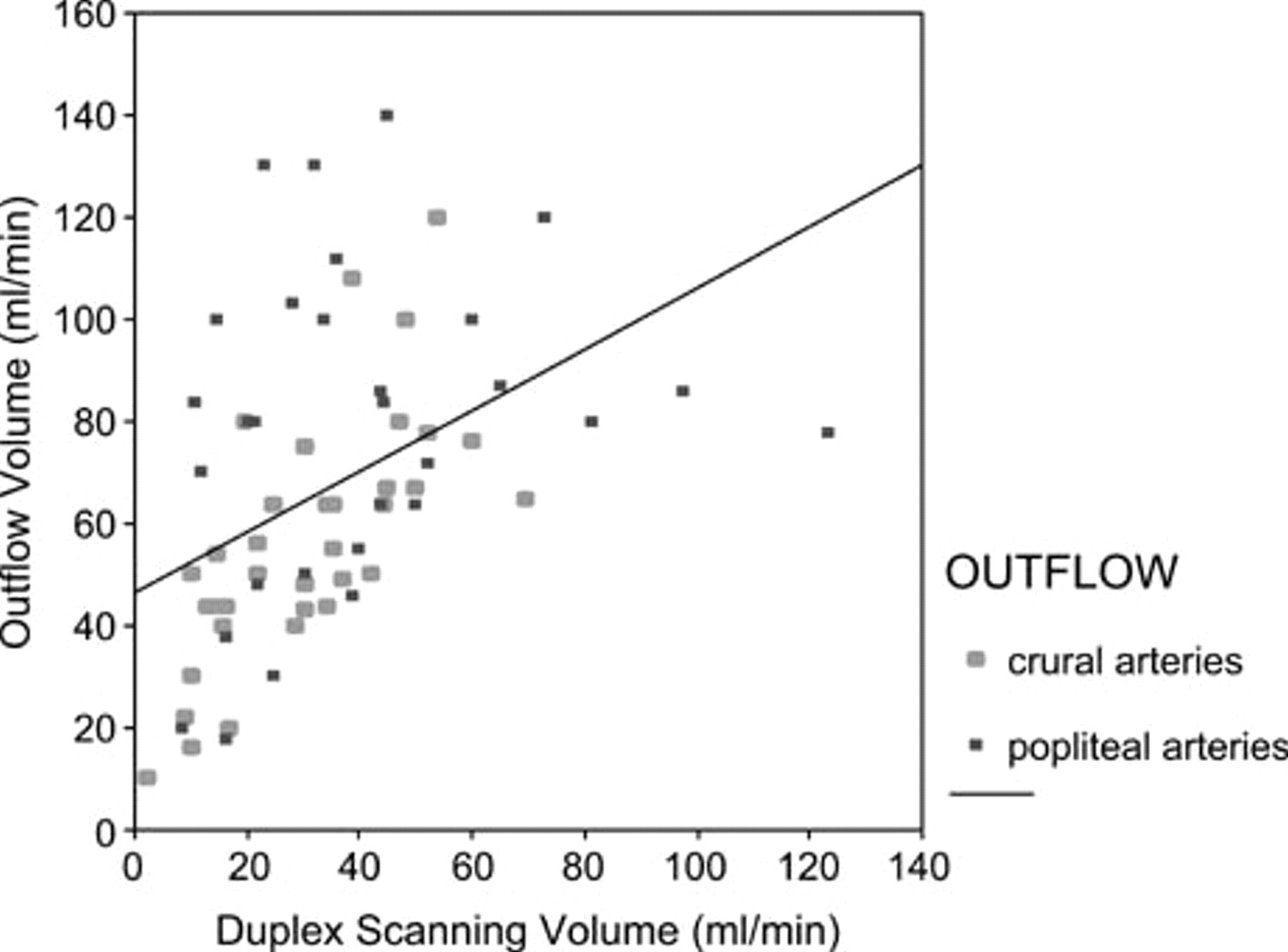
Preoperative duplex scanning flow volume and intraoperative outflow volume correlation in ischemic lower limb revascularization.
Plots of paired observations for crural arteries are shown in Figure 5. The 95% confidence interval for the regression line and the 95% prediction interval for an individual observation are also shown. Figure 6 is a difference plot of the data according to the Bland and Altman method (differences between the two techniques plotted against the averages of the two techniques).

Plot of the volume blood flow as measured by preoperative duplex scanning flow volume (VOL_DS) and intraoperative outflow volume (OV).
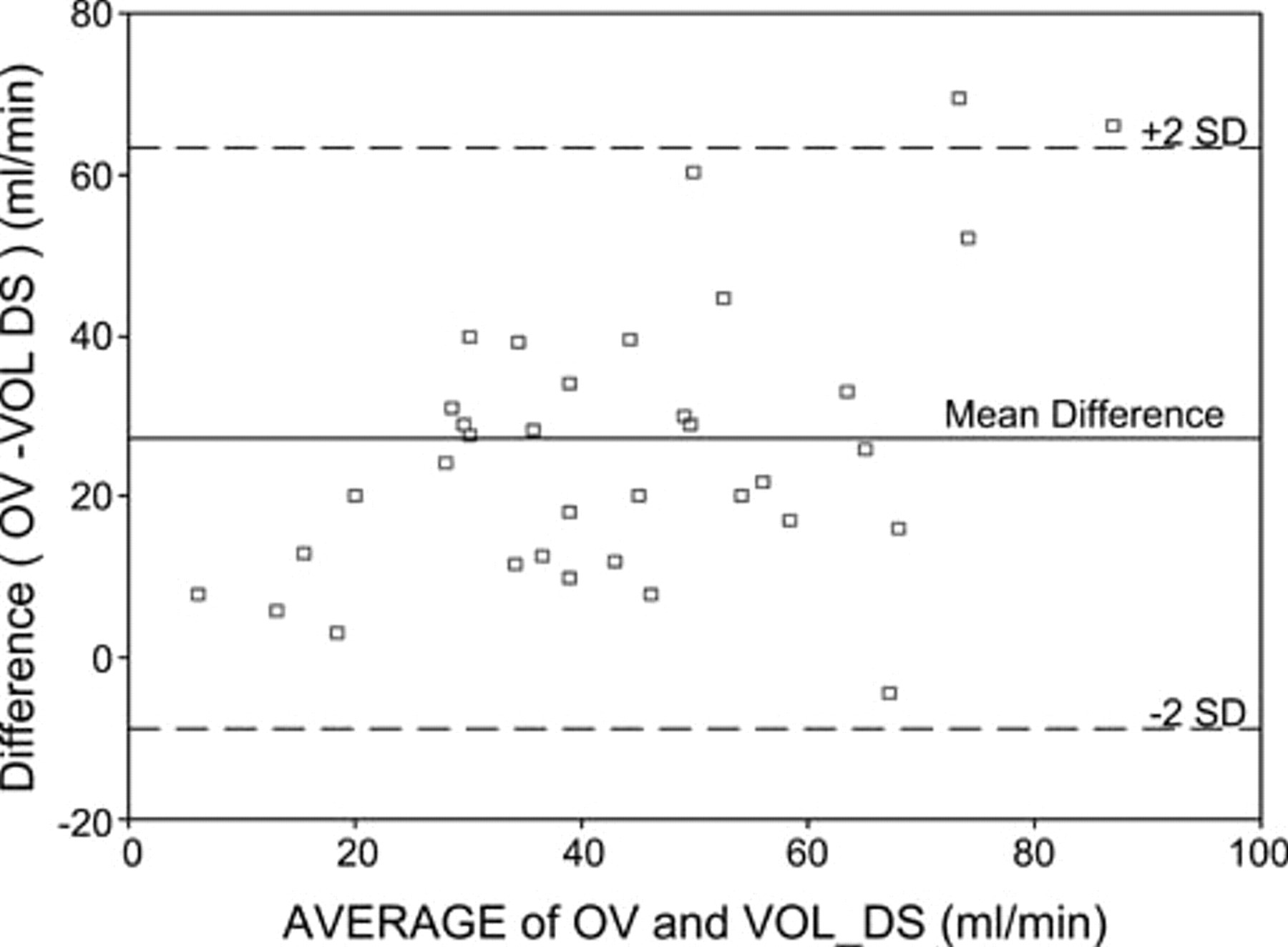
Differences in measurement of volume blood flow between preoperative duplex scanning flow volume (VOL_DS) and intraoperative outflow volume (OV) (y-axis) are plotted against the mean of the two methods (x-axis).
Discussion
Since the pioneer work of Strandness and colleagues, 35 Doppler ultrasonography has expanded the role of noninvasive tests in vascular diagnosis. 36 With the development of ultrasonic DS, a method that combines anatomic data with physiologic information became available and the functional significance of observed lesions could be characterized. At first, this technique was used in the extracranial carotid artery, 37,38 and the excellent results stimulated the study of its application in the preoperative planning of lower limb revascularization. 39–51 Currently, it has been used as the sole preoperative imaging method, and its results suggest that the accuracy of DS approaches that of angiography. 52–55 Clearly, DS has numerous advantages in the preoperative ischemic limb outflow study because it is noninvasive and can depict anatomic and hemodynamic information. Paradoxically, DS power in predicting outflow resistance has never been studied before.
Probably, intraoperative direct measurements are the most realistic way to depict runoff resistance and, theoretically, the right method to test preoperative DS power in studying outflow resistance. In this study, we compared DS preoperative VEL-DS and VOL_DS with intraoperative OV, OP, and RI trying to find a positive correlation between them.
Preoperative DS has proven to be not only suitable for clinical use but also to be as good as digital angiogram (DA) at defining both the location and extent of arterial involvement. Only five patients (6.8%) were excluded from the study because of DS technical failure. Deeply situated peroneal arteries and severe arterial calcification were revealed to be challenging for DS insonation. The presence of severe limb infection and edema can also limit its use. The analysis of the vessel wall and plaque characterization helped the surgical planning for distal anastomosis positioning. Visualization of residual lumen in both longitudinal and cross sections enabled better estimation of stenosis of eccentric plaques and hemodynamic information even at extremely low flow conditions. It is well known that patients with severe leg ischemia usually present with long and/or sequential stenosis occlusions and quantification of each particular stenosis is minimally relevant for anastomosis placement. 56 Arterial ID, VEL-DS, and VOL_DS were analyzed. Theoretically, we can argue that the better the flow, the lower the outflow resistance and possibly the better site for distal anastomosis placement. VOL_DS results were especially considered when planning for the ideal distal anastomosis site. Whenever there was more than one possible site, we decided on the greatest VOL_DS.
Measurement of volume blood flow using DS has limitations, and sources of error have been described. 57,58 Moreover, several experimental and clinical studies are based on this technique. 59,60 Currently, new generations of powerful digitized color-flow DS systems have become commercially available with built-in options for measurement of volume flow. Hopefully, this new technology and better pitfall understanding will ameliorate the clinical results.
Experimental studies have shown that measurement error can be too high for single measurement in an individual patient for the method to be used in clinical decision making. 61,62 As seen in Figures 5 and 6, the lack of agreement between the individual paired observations may preclude its clinical application for individual preoperative surgical strategy decision making.
In our study in all cases, the arterial site selected by DS analysis for distal anastomosis placement could be surgically exposed and submitted for intraoperative outflow resistance analysis by the method described above. As the correlation between preoperative DS and intraoperative direct flow measurements was analyzed by Pearson's correlation coefficient test, we noticed that there was a statistically significant but not impressive correlation power for these parameters. Interestingly, when this analysis was done considering the distal anastomosis placement site, we observed a poor correlation for supragenicular and infragenicular popliteal arteries but a stronger correlation for crural arteries. Possibly, this can be related to the convergent pattern of the limb arterial circulation and the different arterial collateralization status of the ischemic limb studied. 63–65 At proximal arterial segments, the influence of these variables can be much more powerful than at distal sites. It is well known that the number of arteries in confluence with the popliteal arteries can influence the outflow resistance at these segments. 33,66 This could be seen in our study when we considered the higher VOL_DS and OV and lower RI values for proximal arterial anastomosis sites.
We conclude that preoperative DS can frequently define the best distal arterial and outflow segment to be revascularized based on anatomic and hemodynamic parameters. There is a positive hemodynamic arterial flow correlation between preoperative DS and IDOR measurements in ischemic lower limb revascularization, particularly in crural revascularization surgery.Besides technological limitations, the positive DS hemodynamic capabilities shown in this small-series study may extend its application for perioperative hemodynamic follow-up, examination of groups, and comparison of groups. It may also assist in the evaluation of new drug, surgical, and angioplasty therapeutic strategies.