
Abstract
Pseudoaneurysm (PSA) formation is an uncommon complication in carotid surgery. PSA of the carotid artery requires surgical or endovascular treatment to prevent PSA thrombosis, embolization from the thrombotic material within the PSA, hemorrhage after rupture, or compression on the adjacent structures. We present a case of a symptomatic common carotid PSA that occurred 14 months after routinely performed eversion carotid endarterectomy.
Pseudoaneurysm (PSA) formation is an uncommon but well-recognized complication after carotid endarterectomy (CEA), 1 most frequently described after patch angioplasty following longitudinal arteriotomy of the common carotid artery (CCA) and the internal carotid artery (ICA) for the treatment of atherosclerotic disease. 2–4 Infection is most frequently identified as a cause of PSA formation, either through suture-line failure or after bacterial colonization of the patch material. 2 When diagnosed, PSA of the carotid artery requires surgical or endovascular treatment to prevent PSA thrombosis, 3,4 potentially fatal embolization from the thrombotic material often present within the PSA, hemorrhage after rupture, or compression on the adjacent structures. We present a case of a symptomatic common carotid PSA that occurred 14 months after eversion CEA. In the available English literature, we could not find a similar case that complicated an otherwise routinely performed procedure.
Case Report
A 63-year-old male was admitted to our vascular surgery clinic for a 3 cm pulsating mass in his left midneck (Figure 1). Fourteen months earlier, eversion CEA and abbreviation of the ICA were performed for a symptomatic 80% diameter stenosis with transient ischemic attack (TIA).

A 3 cm pulsating mass is seen in the left midneck of our patient 14 months after eversion carotid endarterectomy.
The risk factors registered were hypertension, smoking, and a family history. The patient also complained of claudication in his right leg, but the walking distance was long, and further diagnosis was not proposed. Duplex scanning of the supra-aortic branches showed hemodynamically significant carotid atherosclerotic disease. Echocardiography showed an ejection fraction of 30%, with mitral regurgitation of 3+, and coronarography showed significant coronary artery disease.
CEA of the CCA was performed using a Vollmar ring device from the distal edge of the opening in the CCA, formed after ICA transection, downward to the clamp. The operation and postoperative course were uneventful. Three months after CEA, he had an acute inferolateral myocardial infarction, and coronary artery bypass grafting with mitral valve repair was done.
After the initial 1-month examination, the patient did not return for further follow-up for personal reasons.
The most remarkable physical sign on admission was an outstanding vagal reaction after the slightest pressure on the mass; extreme dysphagia with vomiting sensations resolved immediately after releasing the mass. There were no signs of infection such as fever, leukocytosis, or erythema.
Duplex scanning of the mass revealed a PSA of 18.7 mm in transverse diameter, with thrombotic masses (Figure 2). Angiography was not performed for suspected embolic complications.

A duplex scan of the mass showing a pseudoaneurysm (PSA) of 18.7 mm in transverse diameter with thrombotic masses. Top, sagittal plane; bottom, transverse plane. Dotted lines enhance the outer limit of the PSA.
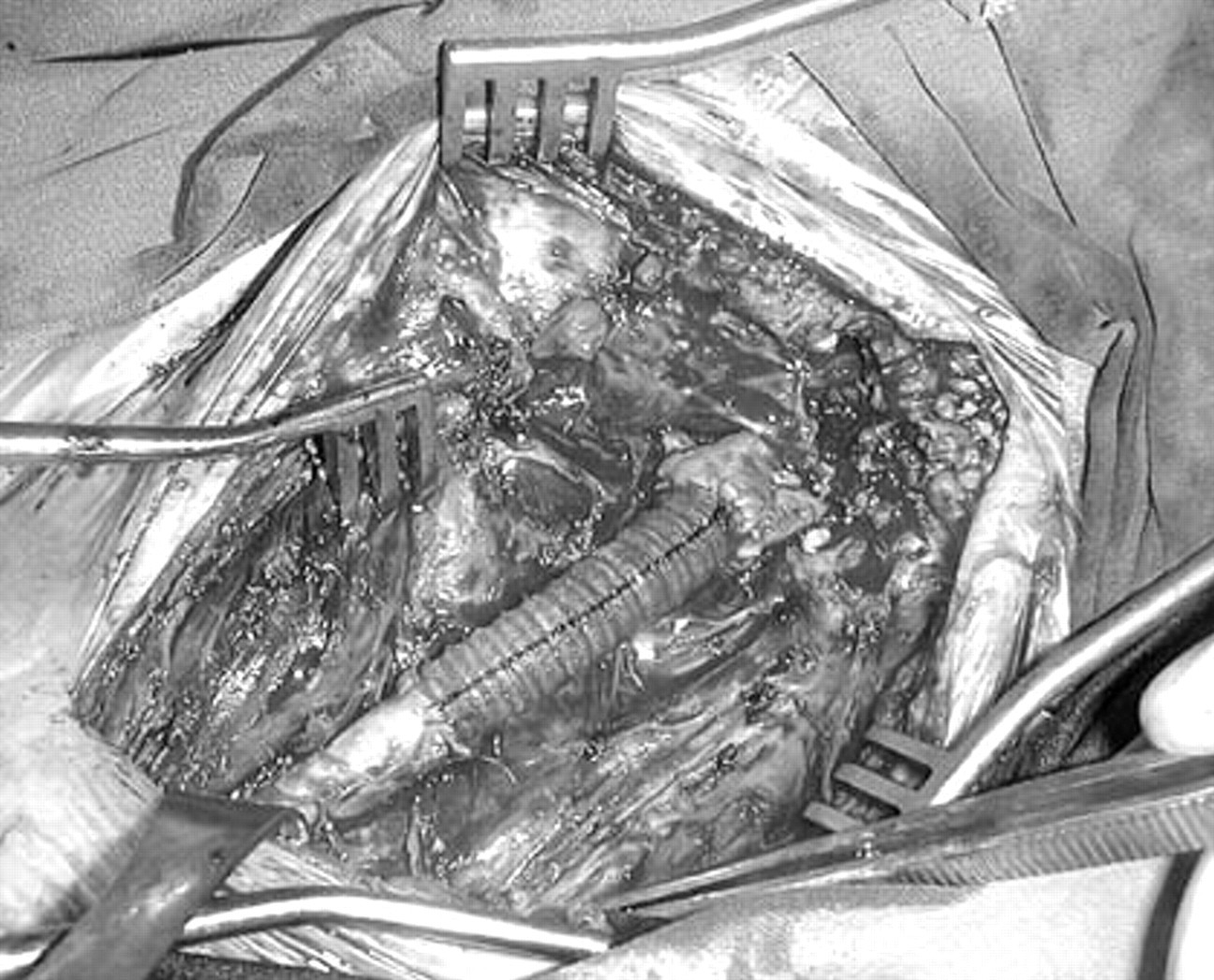
Surgical treatment included dissection of the PSA, identification and preservation of the vagal nerve, and dissection of the ICA. The most remarkable intraoperative finding was a massive thrombus within the PSA (Figure 3). Reconstruction included PSA resection and tubular Dacron graft interposition with the intraluminal Prewitt-Inahara shunt throughout the operation (Figure 4). An 8 mm graft was used to fit both the ICA and the patent external carotid artery in the anastomosis, and because the CCA was wide, the reconstruction was agreeable.

Top, Operative view; pseudoaneurysm (PSA) dissected with identification and preservation of the vagal nerve and dissection of the internal carotid artery. Bottom, Thrombus within the PSA.
The reconstruction included pseudoaneurysm resection and 8 mm tubular Dacron graft interposition.
The aneurysm wall was submitted for histologic examination, which revealed a thin neointimal layer with zones of smooth muscle cell proliferation and scattered extracellular matrix. Cultures were taken from the thrombus, aneurysmal wall, and the surrounding tissue but remained sterile.
The operation and the postoperative course were uneventful; all of the symptoms of the vagal stimulation resolved instantly, and the patient was discharged from the hospital on the sixth postoperative day. He was discharged on aspirin 100 mg/daily, β-blockers, and angiotensin-converting enzyme inhibitors. Routine controls were done after 1 month, after 6 months, and after 1 year. Clinical and duplex scanning findings during the 5-year follow-up were satisfactory.
Discussion
The potential for PSA formation is an uncommon but well-recognized complication associated with patch closure following longitudinal CEA. 1,5,6
In the series of El-Sabrout and Cooley, PSAs related to Dacron patches occurred in 38 (58%) of 65 patients with extracranial carotid aneurysms registered at the Texas Heart Institute from 1960 to 1995. 7 Other authors reported on much smaller postendarterectomy PSA series, 4 or single-patient case reports were described. 2,3,8 Infection was the most frequent cause of PSA formation, 7 but bioprosthetic patch technical failure was reported as well. 3,4 Some case reports did not report on the etiology of the PSA. 2
Opposite to longitudinal endarterectomy, series that reported on eversion endarterectomy did not recognize PSA as a serious postoperative complication. 1,9,10 Our experience in 2,124 eversion CEA procedures performed from 1992 to 1997 is similar to these reports because we did not encounter a PSA that required surgical treatment in that period. 11 These facts were frequently used in favor of the eversion technique when compared with longitudinal endarterectomy because the eversion technique needs no patch material, thus minimizing the infective complications ascribed to patch material.
Given that our patient had no signs or symptoms of infecton, the probable cause of PSA formation was thinness and weakness of the residual carotid artery wall left after endarterectomy, with hypertension contributing to PSA enlargement in time. Our technique at that time included a large oblique opening in the distal CCA and the bulb resulting from the initial incision about half an inch from the bifurcation; instead, a short ICA transection is usually performed. This resulted in a “patch” formation after eversion from the proximal ICA, which was enlarged even after cephalad incision from the heel of the transected ICA to correct the redundancy that is often present. Also, Vollmar ring endarterectomy was a routine part of the procedure for the CCA endarterectomy. Therefore, the PSA presented was formed after proximal ICA eversion, classic bulb and distal CCA endarterectomy technique, and proximal CCA Vollmar ring endarterectomy. This experience caused a change in our technique, so that we now complete the endarterectomy procedure at the distal end of the opening in the CCA, which is formed after transection of the ICA. Our further experience is satisfactory because only one PSA occurred from 2000 to 2005 that needed surgical correction, but it was seen in a patient with correction of the ICA kinking in whom no endarterectomy was performed.
Noninvasive color Doppler ultrasonography, which is easily repeatable, can provide useful data for the morphologic evaluation of a carotid PSA. Although it was frequently used in other reports, 2–4,7,8 it was always followed by angiography, even in the cases when endovascular repair was not performed. Given that the authors did not comment on that, we could presume that angiography was considered a “gold standard” for indicating surgical treatment.
We did not perform angiography in our patient, fearing embolic complications from the mural thrombus that was seen on the duplex scan. The confinement of the PSA to the midneck and to the CCA, its relatively small size, and no need to visualize the aortic arch influenced our procedure to be the opposite of the experience of other authors who routinely perform angiography.
Because of the unpredictability of ischemic complications and possible fatal stroke following eventual thrombotic embolization to the brain from the PSA, early and appropriate repair is recommended. 2,5 As stated by Hertzer, surgical treatment appears to be quite appropriate for most aneurysms that are located near the carotid bifurcation, which was the case in our patient. 5 We decided to perform Dacron graft interposition because no appropriate vein was available after coronary artery bypass grafting and no local or systemic signs of infection were present. Furthermore, we obtained optimal diameter matching of the CCA and the graft and avoided the kinking and thrombotic occlusion that occasionally occur after imperfectly tailored venous grafting. However, surgical correction of a carotid PSA should be performed by experienced teams in high-volume carotid surgery institutions.
The inherent risks of reoperative carotid surgery and growing practice of endovascular therapy resulted in endoluminal exclusion of a postoperative carotid PSA using Dacron, polytetrafluoroethylene, or autologous vein covered stents. This technique seems to be particularly useful in high-risk patients who may not be candidates for open reconstruction, 3 but so far, only small series or single case reports were presented, with short-term follow-up. 2–4,8 In these reports, early thrombosis was reported, 4,8 whereas embolization from the thrombus within the PSA might occur during the procedure. 2,4 In our case, endovascular treatment was not a reasonable option because it was necessary to completely remove the PSA and its content and eliminate any compression to the vagal nerve, with its frustrating symptoms for the patient. Nevertheless, whichever technique is chosen to repair postendarterectomy carotid PSA, open-surgical or endovascular, the decision should be made after an individual patient risk/benefit evaluation.