
Abstract
The purpose of this article is to report the initial experience with endovascular repair of thoracic aortic disease in a single tertiary vascular unit in northwestern Greece.
Between 2003 and 2005, 16 patients were treated with endovascular techniques for various pathologies of the descending thoracic aorta. Twelve patients were treated electively and four emergently. Operative and follow-up data for a mean time of 18.4 months were retrospectively collected and analyzed.
Primary technical success was obtained in 14 (87.5%) cases. No early or late deaths occurred, and there was no major operation-related complication. No paraplegia was observed in our patients. Stent graft–related complications occurred in 18.75% (one type 2 and two type 3 endoleaks), but they all had a favorable outcome. No further problems have been reported in any of our patients.
Endovascular stent graft repair for diseases of the thoracic aorta seems to be a promising alternative to open surgery, especially for high-risk patients. Long-term results are needed to confirm the early benefit of this treatment option with regard to morbidity and mortality rates. The potential of this technique to be applicable even in relatively small, tertiary vascular centers might be of great benefit to patients.
FOR ALMOST 50 YEARS after the first successful repair of a descending thoracic aortic aneurysm (DTAA) by Lam and Aram in 1951, 1 open surgical repair has been used as the treatment of choice for diseases of the thoracic aorta, dramatically increasing the life expectancy of patients who suffer from such pathologies. 2–4 However, open surgery is associated with considerable morbidity and mortality, especially in emergency situations and in type B aortic dissections, although the frequent comorbidities of these patients quite often make them unsuitable candidates for surgical intervention. 5–12 Endovascular techniques have been lately proposed as an alternative treatment for thoracic aortic disease because they have the potential to decrease morbidity and mortality rates and thus expand the number of patients to whom a safe treatment can be offered. 13
Until now, several single series and quite recently the European and UK registries have reported their experience with endovascular stent graft treatment of thoracic aortic lesions. 14–20 Although it is too early to demonstrate the long-term results of this treatment option, the short- and midterm data from the vast majority of these centers are undoubtedly encouraging. The purpose of this report is to present the initial experience with endovascular treatment of different thoracic aortic pathologies in a single tertiary vascular unit in northwestern Greece.
Methods
We retrospectively reviewed 16 patients who were treated with endovascular stent grafts for thoracic aortic disease between March 2003 and December 2005. Eighteen patients who were admitted during this period to our vascular unit were suffering from such pathologies. The two patients who did not receive endovascular therapy were treated, one with open surgery and the other conservatively because he refused any treatment option. All of the procedures were performed in the Vascular Surgery Unit of the University Hospital of Ioannina in northwestern Greece. The endovascular approach was applied electively on 12 patients as the first-choice treatment, as well as in four emergency situations. Fourteen of these patients (87.5%) were evaluated to be at high risk of open surgery (American Society of Anesthesiologists [ASA] class 3 or 4). All patients gave informed consent to undergo endovascular stent graft repair (EVR). It must be mentioned that for a similar period of 3 years prior to EVR introduction to our unit, 12 patients had presented with thoracic aortic pathologies. Three of them were treated with open surgery for DTAAs, whereas nine were treated conservatively, two for uncomplicated type B aortic dissections and seven because they refused or were at high risk of open surgery.
The aortic diseases and history of the patients are shown in Tables 1 and 2. Perioperative imaging consisted of computed tomographic (CT) angiography of the thorax, abdomen, and pelvis for all patients with multiplanar reconstruction when judged necessary. The 12 electively treated patients additionally underwent classic angiography of the aorta. The criteria used to determine the anatomic suitability for EVR of all of the diseased aortic lesions was a proximal and distal aortic neck ≥ 2 cm. However, in two cases for which such a proximal aortic neck was not available below the orifice of the left subclavian artery, we decided to use part of the distal aortic arch as an additional landing zone, thus overstenting the left subclavian artery. After EVR and hospital discharge, patients were routinely followed up with clinical examination and CT angiography of the aorta at 1, 3, 6, and 12 months and annually thereafter.
Patients' Characteristics and Procedure-Related Results
History, Pathology, Surgery, and Follow-Up Details of Each Patient
AAA = abdominal aortic aneurysm; AV = aortic valve; EVR = endovascular repair.
*Descending thoracic aortic aneurysm and AAA EVR at the same procedure.
All of the EVR cases were performed under general anesthesia except one, which was performed under spinal anesthesia because the patient was suffering from severe obstructive pulmonary disease. Appropriate preparation for thoracotomy was done for all patients in the event that conversion to open repair was needed during the procedure. All of the endografts were deployed through a common femoral artery. Additionally, the left radial artery was catheterized and a 5F sheath was inserted in all cases. An angiography catheter was then forwarded into the aortic arch to perform intraoperative angiography. We preferred the left radial artery instead of brachial artery catheterization to avoid ischemic complications to the distal upper extremity during or after the procedure. Additionally, with this access, the existence of the angiography catheter inside the left subclavian artery and the aortic arch offered a continuous marking of the orifice of the left subclavian artery during the procedure, something that cannot be easily achieved with contralateral femoral artery access. Cerebrospinal fluid drainage or other spinal cord protective adjuncts were not used in any of the cases.
Eleven patients were treated with Talent devices (Medtronic AVE, Medtronic Europe SA, Route du Molliau, Switzerland) and five with TAG devices (W.L. Gore & Associates, Inc., Flagstaff, AZ). In eight patients, more than one endograft was used. Two of the patients with DTAA had a coexisting abdominal aortic aneurysm, which was treated during the same procedure with EVR, whereas three had undergone previous open surgery for abdominal aortic aneurysm repair. In one case, the EVR was performed as the second-stage procedure for the repair of the DTAA after previous aortic valve, ascending aorta, and aortic arch replacement with the elephant trunk technique for the treatment of an extended aortic aneurysm affecting the entire thoracic aorta. In this case, the proximal landing zone of the endograft was into the previously placed synthetic Dacron graft, just proximal to the distal arch anastomosis. 21 After the end of the procedures, all patients were taken to the intensive care unit (ICU) for monitoring in the early postoperative period.
Perioperative and follow-up data were collected for all patients. These consisted of operative and stent graft–related early (< 30 days) and late (≥ 30 days) complications, length of ICU and hospital stay, blood loss and biochemical measurements, and primary technical success of the procedure (complete exclusion of the aneurysm sac, seal of rupture, or coverage of the entry tear for dissections with absence of type 1 or 3 endoleak), as well as early (< 30 days) and late (≥ 30 days) mortality.
Results
Table 1 summarizes the results of treatment, and Table 2 presents analytic details for each patient. The mean age of the patients was 60.8 years, and the median age was 67 years, with a range between 17 and 79 years. Fifteen patients were men, and one patient was a woman. The mean diameter of the aneurysms was 6.2 cm (median 6 cm, range 4–8 cm). Primary technical success was obtained in 14 (87.5%) patients. In one case (false anastomotic aneurysm), a type 1 endoleak occurred during the procedure that was treated successfully at the same time with the deployment of an additional endograft. The endoleak was not apparent at the end of the EVR and, as such, was not considered a stent graft–related complication or primary technical failure. In two patients, a type 3 endoleak was observed. These patients were treated with two sequential endovascular prostheses, and the endoleaks were observed at the overlapping zones of the two components even though the overlap exceeded 2 cm in each case. Balloon remodeling during the procedure minimized the leaks but failed to eliminate them completely. The procedures were terminated, and the patients were followed up intensively. The endoleaks were spontaneously resolved after 2 days and 1 month, respectively, without the need for any additional intervention. At the latest follow-up point for each patient, no signs of endoleaks were observed in CT scans. No conversions to open repair were needed, and no additional surgical interventions were performed on any patient. In two patients, the aneurysm morphology required overstenting of the orifice of the left subclavian artery. However, none of them developed clinically claudication of the left upper extremity or subclavian steal syndrome, and, as such, the surgical revascularization of the left subclavian artery was not considered necessary. Both patients remain under close clinical follow-up.
There was no mortality in the early postoperative period in this series. The mean length of ICU stay was 1.4 days (range 1–3 days), and the mean length of hospital stay was 5.9 days (range 3–10 days) for the whole cohort, whereas for the elective cases, it was 4.7 days (range 3–7 days). A mean of 0.4 blood transfusions (range 0–2) was required during or after the endovascular procedures, and one patient required platelet transfusion because of a severe postoperative decrease (fewer than 50 × 10 3 /μL). 22 None of the patients developed neurologic deficits after the repair. In 11 cases, a mild elevation in leukocytes (10.4 × 10 3 /μL to 18.3 × 10 3 /μL) and C-reactive protein (11–59 mg/L), as well as a mild elevation of body temperature (up to 38.5°C), was recorded in the early postoperative period. This phenomenon lasted for 2 to 5 days, without any evidence of systemic or specific organ infection. A postoperative systemic inflammatory response (postimplantation syndrome) has been described to occur after thoracic EVRs. 23
The mean follow-up time was 18.4 months, ranging between 3 and 34 months. There was no late and only one early surgery-related complication. This consisted of a pseudoaneurysm formation at the catheterization point of the left radial artery by the third postoperative day. The pseudoaneurysm was treated surgically by excision of the false aneurysm and repair of the radial artery. As mentioned above, there were two early stent graft–related complications (12.5%) concerning the two type 3 endoleaks that occurred during the procedures at the overlapping zone between two endoprostheses. There was also one late stent graft complication, a type 2 endoleak related to the false anastomotic aneurysm, which was seen the first month after the procedure and was ascribed to a previous erosion of the lung by the ruptured false aneurysm. This endoleak was gradually diminished and eventually disappeared at the eighteenth postoperative month. Thus, the overall graft-related complications accounted for 18.75% of the patients. For the time being, in 8 of 13 (61.5%) patients with aneurysms of any kind, the aneurysm sac has begun to shrink (in 2 of them, it has almost disappeared), whereas in 5 cases, the sac dimensions remained unchanged. In the remaining three patients with acute dissections or a penetrating ulcer, total or partial remodeling of the descending thoracic aorta wall has been noticed, even though in two of them, the follow-up period is quite short (Figures 1 –3).

Acute Stanford type II dissection, with subsequent rupture. A, Preoperative angiogram showing the false lumen and the entry tear. B, The same picture after the deployment of two sequential thoracic stent grafts; the false lumen has disappeared.

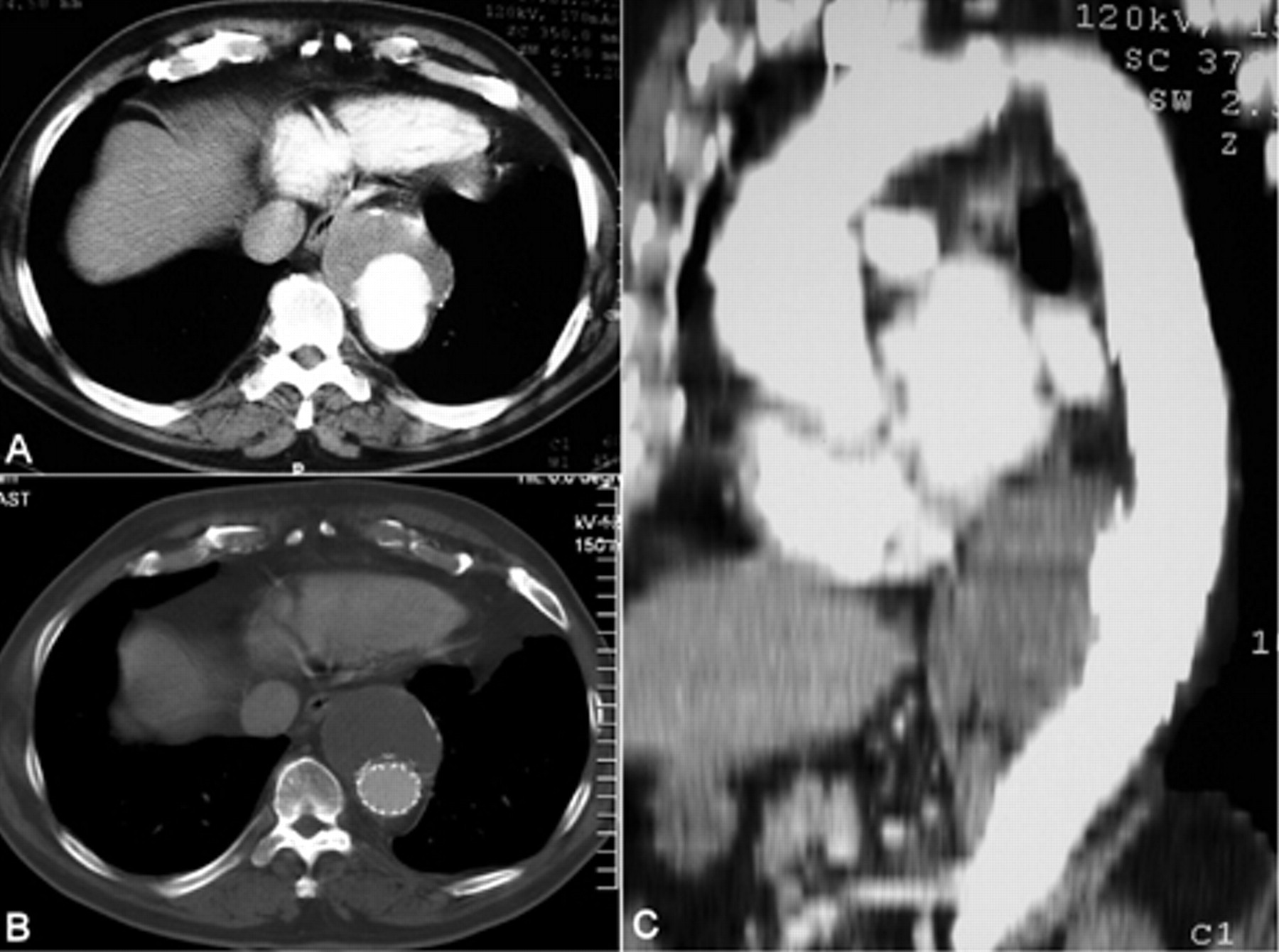
Computed tomographic (CT) scans of the case in Figure 1. A, Preoperative CT scan showing the dissection in the midportion of the thoracic aorta, with a developing hematoma around it. B, The same picture 2 days after the endovascular procedure showing the expansion of the true lumen and the disappearance of the false lumen of the descending thoracic aorta. C, A year later, complete remodeling of the aorta has occurred.
Degenerative aneurysm of the distal descending thoracic aorta. A, Preoperative computed tomographic (CT) scan showing the aneurysm just above the diaphragm. B, The same picture 6 months later, showing the exclusion of the aneurysmal sac by the endograft. C, Oblique reconstruction from CT scans, also showing the exclusion of the aneurysmal sac.
Discussion
Without treatment, most of the aneurysms and dissections of the descending thoracic aorta will rupture, with the subsequent death of the patient. 4 Open surgical repair offers great benefits in this population of patients by reducing the risk of rupture and significantly improving their overall survival. 2–4 However, surgery of the descending thoracic aorta is even now associated with considerable morbidity and mortality. In particular, the mortality rates associated with the open repair of DTAAs range between 5 and 22%, 5–12 whereas for type B aortic dissections, the rate can be even higher. 24–26 Additionally, cardiac and pulmonary complications, renal failure, stroke, and paraplegia are quite common after these operations. 8–10,27
As an alternative option, EVR seems to offer several advantages for the treatment of these diseases. The avoidance of proximal aortic cross-clamp, thoracotomy, and surgical exposure of the mediastinum might play a major role in reducing the overall perioperative complications during these procedures. Recent studies have reported very low incidences of myocardial infarction (0–2%), cerebrovascular accident (0–4%), postoperative pneumonia (4–9%), renal failure (0–2%), bleeding (up to 5%), and paraplegia (0–4%) during EVR of thoracic aortic lesions. 18,20 Additionally, the early and midterm follow-up data have shown overall mortality rates below 10%. 14–20 Although the above initial results are undoubtedly encouraging, it is too early to appraise them in comparison with the results of the open surgery procedures because of the lack of long-term follow-up and randomized clinical trials and the different patient selection criteria probably used for the EVR procedures.
Despite this incomparability, paraplegia seems to be one of the most clearly decreased complications with the endovascular approach, and the most recent studies have reported rates below 5%. 15,18–20 It is well known that paraplegia is a result of the aortic cross-clamping and the subsequent spinal cord ischemia, and it is strongly correlated with the duration of the aortic occlusion. 5,7,28 Avoidance of proximal aortic clamping with the EVR techniques may account for the reduction in spinal cord complications. Coverage of intercostal arteries by the endografts does not seem to lead so frequently to spinal cord ischemia even when long segments of the thoracic aorta are excluded. 19 However, it remains to be defined whether the risk of postoperative paraplegia is increased when lumbar arteries are thrombosed owing to a concurrent abdominal aortic aneurysm or have been sacrificed in previous abdominal aortic aneurysm surgery. In our series, we treated two patients simultaneously for DTAA and abdominal aortic aneurysm, whereas three other patients had been treated previously with open surgery for abdominal aneurysms. Although this combination resulted in circulatory exclusion of many spinal cord feeding arteries (intercostal and lumbar), none of the patients developed postoperative neurologic deficits. However, distal landing zones of the thoracic endografts in these cases did not exceed the T9 level, and, as such, the crucial segmental arteries, including the artery of Adamkiewicz, possibly had remained uncovered by the endograft.
Stent graft–related complications after EVR are primary or late endoleaks or migrations in the vast majority of patients. However, in contrast to EVR for abdominal aortic aneurysms, these complications seem to happen more infrequently in the endovascular treatment of thoracic lesions. 19 This is especially evident according to type 2 endoleaks, which are the more frequent ones during and after EVR for abdominal aortic aneurysms, whereas they are quite uncommon when treating thoracic aortic pathology. 29 In the recently published results from the European and UK registries, the early (30-day) endoleaks were mostly types 1 and 3 (6%), in contrast to 1.3% of type 2 endoleaks. 19 Furthermore, the late endoleaks at the end of the first year were at 2.5%, although no graft migration was observed. In this series, we observed two early type 3 endoleaks, which were minimized with balloon remodeling intraoperatively and spontaneously resolved in the early follow-up period. The issue of the extent of overlap when multiple thoracic stent grafts are used has not been clarified. 30 Although we used an overlap of at least 20 mm in our cases, a more extensive overlap beyond 30 mm might be safer in the long term to avoid a type 3 endoleak and a subsequent separation in the future. 31,32 There was only one late endoleak (type 2) in this series, which also spontaneously disappeared during the follow-up time. The type 1 endoleak that occurred intraoperatively was successfully treated at the same time and was not apparent at the end of the procedure. In any case, it seems that the problem of endoleaks following the EVR of the descending thoracic aorta is not as serious and common as it appears to be in the abdominal aorta.
It is known that many patients suffering from thoracic aortic diseases remain untreated because of coexistent morbidities. Severe cardiovascular or pulmonary diseases, especially in elderly patients, may be contraindications for open surgery or lead to adverse outcome after treatment. On the other hand, in most of the EVR studies, a considerable number of patients were generally suffering from several comorbidities in addition to the thoracic aortic disorder, and a large number of them were usually classified as ASA class ≥ 3. Many of these patients would have been proved unsuitable for open surgery; however, EVR was performed safely, with good results. In addition, EVR has the advantage of being performed under regional or even local anesthesia. General anesthesia may be preferable during endovascular procedures on the thoracic aorta to obtain better arterial pressure control and avoid intraoperative stent graft migration. However, for the very unfit patient, as was one in our series, regional anesthesia may be considered an alternative option and with careful management of blood pressure may also offer successful results. Therefore, EVR has the potential to be applied in a population of patients who otherwise would remain untreated and in that way expand the number of patients to whom a safe intervention can be offered. This impact of EVR on the treatment of thoracic aortic disease was quite evident in our single vascular unit experience. For a period of 3 years before EVR introduction, only 3 of 12 patients who presented with several thoracic aortic pathologies were finally treated with open surgery. In contrast, between March 2003 and November 2005, the regular application of EVR significantly increased the percentage of treated patients to 17 of 18 (16 EVRs, 1 open surgery), whereas an increase in the absolute number of the admitted patients was also observed.
The favorable results of our initial experience in terms of mortality and major complications could be attributed to the small number and relatively low mean age of the treated patients. However, the application of this minimally invasive method for the treatment of thoracic aortic disorders in our institution showed the same tendency in reducing mortality and complications as has been reported in most published series so far. Our results indicate that EVR for thoracic aortic diseases can be successfully applied even in relatively small tertiary vascular units with the appropriate outfit. Spreading of EVR in such centers would expand the applicability of treatment of descending thoracic diseases. The latter might be of great benefit for the population of patients who suffer from such pathologies.
In conclusion, EVR for the treatment of descending thoracic aortic disease seems to be a valid alternative option to open surgery, especially for high-risk patients. Short- and midterm results have been promising, whereas the long-term results are awaited to confirm this benefit. The potential of EVR for wide application among vascular centers may additionally benefit the population of patients with thoracic aortic disease.