
Abstract
Inflammatory aortic aneurysms (IAAs) represent a rare form of aortic aneurysms. Compared with atherosclerotic aneurysms, patients with IAA have an increased risk of perioperative and long-term morbidity. This retrospective clinical study analyzed the outcome after conventional and endovascular repair of IAAs.
Patients treated for an abdominal IAA between January 1995 and November 2004 were included. Imaging (computed tomographic angiography or magnetic resonance angiography) was performed preoperatively and at the time of follow-up (mean 2.7 years). Transperitoneal open repair and endovascular aortic repair were the operative procedures used.
Over 10 years, 40 patients were treated with conventional and 5 patients with endovascular repair. The in-hospital morbidity rate was 11.1% (five patients; four conventional, one endovascular). On 10 patients (47.6%), the retroperitoneal fibrosis was no longer detectable.
After operative repair, the majority of cases presented with a distinct regression of inflammation. Endovascular treatment of IAA represents a feasible alternative procedure to open aortic repair.
THE TERM inflammatory aortic aneurysm (IAA) as a pathologic entity was first reported by Walker and colleagues in 1972. 1 They described a special pathoanatomic group of aneurysms that were characterized by a special wall composition and morphology found in 10% of the patients surveyed. A typical sign of the disease is the combination of a thickened aortic wall with an extensive perianeurysmal and retroperitoneal fibrosis, as well as adhesion to adjacent organs. 2–4 IAA usually first becomes clinically apparent owing to an inflammation-related complication such as urinary constriction (case report, first described in 1935 by James). 5 With regard to the clinical picture, IAAs are more frequent in symptomatic patients, and there is a clear predominance of male patients (proportion of males to females 30:1 to 6:1). 2,4,6,7 When compared with atherosclerotic aneurysms (AAs), the incidence of this disease, which occurs in patients 5 to 10 years younger, also stands out. Almost all patients with IAA are heavy smokers. 3,8,9 In the majority of cases, the ureter, vena cava, and proximal jejunum are included in the inflammatory process.
To lower the risk of affecting perianeurysmal structures, in 1978, Goldstone and colleagues proposed a preparation technique that reduces local mobilization to a minimum. 9 This form of operative procedure considerably reduced the morbidity and mortality rates of patients with IAA.
Postoperative follow-up examinations demonstrate different results with regard to morbidity and the course of retroperitoneal fibrosis after aortic replacement. 8,10–12 A study published in 2003 demonstrated a significantly higher percentage of proximal para-anastomotic aneurysms in contrast to patients with AAs as a disease-typical complication of IAA. 10 Information on endovascular aortic replacement for IAA was published recently as both a meta-analysis and an evaluation acquired from the EUROSTAR database. 13,14 The objective of the present report was to analyze early and late complications after aortic repair for IAA, the proportion of proximal para-anastomotic aneurysms, and the status of inflammation after open and endovascular aortic replacement in a single center.
Patients and Methods
From January 1995 to November 2004, 45 patients were operated on for an IAA in our department. Computed tomographic angiography (CTA) or magnetic resonance angiography (MRA) was performed preoperatively (MRA was performed on patients with limited kidney function). Patients who demonstrated signs of inflammation in the preoperative imaging or at the time of the operation were defined as having IAA. Radiologic signs include disease-typical vessel wall thickening with additional ventral vessel layer and venous contrast agent enhancement (Figures 1 and 2). Macroscopic signs of inflammation are characterized by a porcelain-colored onion skin–like wall thickening with accompanying massive periaortitis with connective tissue adhering to the surrounding structures (proximal jejunum or ureter) (Figure 3). For conventional aortic repair, sealed, knitted Dacron prostheses were used; the implanted endovascular devices are listed in Table 1.

Computed tomographic angiogram showing an inflammatory aortic aneurysm.
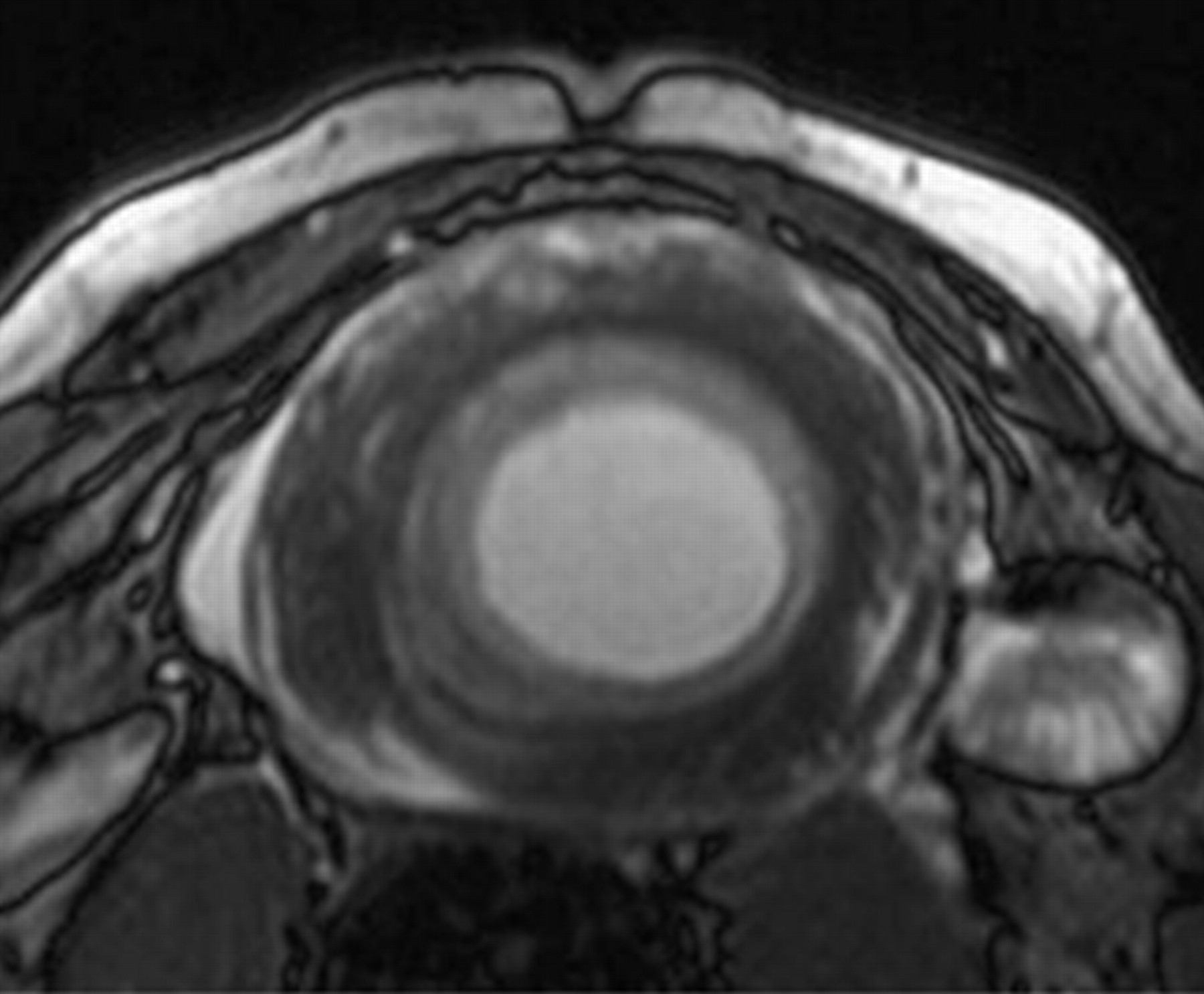
Magnetic resonance angiogram showing an inflammatory aortic aneurysm.

Intraoperative view of an inflammatory aortic aneurysm.
Stent Devices
Follow-ups were performed between April 2004 and March 2005 using clinical examination and computed tomography or magnetic resonance imaging. The patient group to be included in the follow-up investigation was assembled by analysis of retrospective case notes. The follow-up investigation (CTA or MRA) of the study was approved by the local ethics committee.
Results
Forty of 45 patients received conventional open aortic replacement and five patients underwent endovascular aortic repair (EVAR) (see Table 1). The mean age of the patients at the time of operation was 67.3 years (range 51–86 years), 96% were male (male to female ratio 43:2), and 22 patients (48.9%) were symptomatic at the time of the operation; 4 patients (8.9%) presented with a rupture (three conventional, one endovascular).
One patient demonstrated a thrombotic occlusion of an infrarenal IAA during the operation. Three patients (6.7%) presented with thoracoabdominal aortic aneurysms, and four patients (8.9%) had aneurysms of the juxtarenal segment.
In 22 patients (55%) operated on conventionally, the aneurysm was excluded using a bifurcated prosthesis, and on 18 patients (45%), a tube prosthesis was implanted; 3 patients were treated by thoracoabdominal repair. Suprarenal cross-clamping was required for 17 patients (37.8%) owing to the aneurysm's morphology. In seven cases (15.6%), renal revascularization was performed simultaneously, and in seven patients (15.6%), the left renal vein was temporarily separated and resutured after aortic repair (Table 2). At the time of the operation, 10 patients (22.2%) had limited kidney functioning (creatinine range 1.3–7.6 mg/dL). Four patients (8.9%) demonstrated urinary obstruction caused by retroperitoneal fibrosis preoperatively. The in-hospital morbidity rate of patients with IAA was 11.1% (five patients; four conventional, one endovascular), and the overall morbidity rate was 15.6% at the time of follow-up (seven patients; six conventional, one endovascular). In one patient undergoing conventional repair, dehiscence of the abdominal incision occurred. Another patient demonstrated a bypass branch infection after implantation of an aortic bifemoral prosthesis. The infection healed after operative revision with placement of a mesh plug. One patient suffered an early postoperative myocardial infarction. The third patient with thrombotic infrarenal occlusion demonstrated renal insufficiency postoperatively, making dialysis temporarily obligatory. Intraoperatively, a prosthetorenal bypass was applied to the left renal artery, and thromboendarterectomy was performed on the right renal artery. At the time of follow-up, this patient showed renal insufficiency, with an existing stenosis of the right renal artery and an occluded bypass on the left renal artery (creatinine 1.8 mg/dL) (Table 3). To treat the stenosis, percutaneous transluminal angioplasty and stent implantation were performed. Three of 10 patients with preoperatively limited kidney function returned to normal renal function after aortic repair.
Morphologic and Operative Details
Morbidity
One patient from the endovascular group needed a corrective operation after the completion of the endobifurcation failed. In this case, the contralateral leg of the device could not be probed initially owing to the rigid iliac segment. Here an endoconversion into an early elective aortounilateral iliac prosthesis was performed (patient HG; see Table 1). In two patients, endoleaks occurred after EVAR. One patient demonstrated a relevant type 2 endoleak (internal iliac artery) after implantation of a bifurcated prosthesis. The second patient, who was at the rupture stage with an extremely kinked iliac segment, presented with a type 1 endoleak over the inserted occluder (retrograde perfusion of internal iliac artery) after aortounilateral iliac prosthesis implantation with crossover bypass (see Table 1 and Figure 4).

Type 1 endoleak (arrow) after endovascular aneurysm repair.
The in-hospital mortality for the conventional treatment without rupture was 4.1% (two patients); of those three with rupture, two died. Within the group that was treated endovascularly, the mortality rate was 0.
At the time of follow-up, 33 patients were alive (29 conventional, 4 endovascular), and 3 patients were lost to follow-up (73.3%; mean follow-up 2.7 years). On 21 patients, control CTA or MRA of the aorta was performed as part of the follow-up examination; 12 patients refused the examination (older age, immobility, malignant disease). None of the patients who underwent conventional procedures demonstrated a para-anastomotic aneurysm on the proximal (or distal) anastomosis. At follow-up, only two patients demonstrated a urinary obstruction that required therapy; this corresponds to a decline of 50%. In 10 patients (47.6%), the inflammation was no longer detectable at the time of the follow-up; 9 patients (42.9%) demonstrated a distinct regression in the diagnostic findings (< 50% of the initial value), and in 2 patients (9.5%), there was no change in the inflammation wall in comparison with preoperative examinations (Table 4).
Status of Inflammation at Follow-Up
Discussion
Clinical data acquired after conventional aortic repair of IAA from the recent past vary with regard to morbidity and the status of retroperitoneal fibrosis. 10–12 Studies with long-term follow-up that include groups of more than 20 patients are rare. A case-control study published in 2003 described a high incidence of para-anastomic aneurysms of IAA after aortic replacement. 10 The data suggested that the development of para-anastomotic aneurysm may be a disease-typical complication of IAA; certainly, no other studies published focus on this subject. Based on a high incidence of IAA at our own institution, this study was initiated to examine the rate of para-anastomotic aneurysms. Furthermore, data about the course of retroperitoneal fibrosis and the results after EVAR were required.
In 1972, Walker and colleagues defined IAAs as an independent entity, based on specific morphologic prerequisites and an extremely high mortality rate of 31%. 1 More recent knowledge and investigations show that IAA is closest to an extreme course or a final stage of atherosclerotic changes to the vessel wall. 11,15 The etiology of the disease is not completely understood, but it does appear to be multifactorial. When inflammation occurs, genetic factors (autoimmune diseases, male gender, frequency of aneurysms within a family) and environmental factors (smoking) seem to represent the main prerequisites.2,8,11,16–18 At 60 to 70%, the infrarenal aortic segment is the most affected localization. In 40% of patients, the iliac vessels were also involved; in 15 to 20% of patients, there was inflammation of the perirenal segment. The rest were distributed among aneurysms of the thoracoabdominal aorta (10–15%) and the femoral and visceral vessels. 2,19 It is remarkable that the inflammation of the patients with thoracoabdominal aneurysms was mostly part of the infrarenal portion; in the suprarenal and thoracic segments, there was much less indication of inflammation. 19
In 1978, Goldstone and colleagues described an operative technique that took the special morphologic characteristics of IAA into account (“…as little dissection as possible”). 9 With an operative technique that has been adapted to the disease that includes limited mobilization of the surrounding structures, the perioperative mortality and morbidity rates could be reduced almost to the levels of AAs. 8,11,15 The in-hospital mortality rate of the present study for nonruptured IAA was also not elevated compared with patients with AAs treated at the same period of time at our institution (4.1% IAA vs 3% AA). Studies with a larger number of cases, however, show heterogeneous results with regard to long-term postoperative outcome after repair of IAA. 10,11,12,17 This can be caused by the differing postoperative follow-up time frames, the operation techniques performed, and the difference in implanted prosthetic materials.
In their study, Bonati and colleagues demonstrated a significantly higher percentage of proximal para-anastomotic aneurysms of IAA. 10 In our own patients, despite long follow-up intervals of up to 10 years, no para-anastomotic aneurysms could be detected. Of the 33 patients who were still alive, we could acquire 64% for the follow-up investigation; the other 12 patients refused the imaging. This was the result of older age, immobility, or malignant disease. Despite this, our study represents an investigation with one of the highest case loads (21 patients) for long-term follow-up of IAA in the literature.
With regard to signs of inflammation, an analysis of the literature revealed different data. Depending on the follow-up time, the information on the unchanged status of the inflammation differs postoperatively up to a decline in more than half of all cases. 10,11,12,15,17 Our data also demonstrate a significant decline in retroperitoneal fibrosis in 42.9% of patients; in 47.6% of all cases, there were no signs of inflammation. In only 9.5%, the inflammation was unchanged in comparison with the preoperative status (see Table 4). The regression in inflammation clearly reflects the 50% decrease in urinary obstructions postoperatively.
Recently, a meta-analysis and an evaluation of the EUROSTAR database with reference to EVAR of IAA were published. 13,14 In addition to individual reports from the past, 20–24 they currently represent the most well-followed-up collection of IAAs after EVAR. With regard to mortality and the conversion rate, there was no difference in comparison with AAs. The morbidity was significantly higher in the group with inflammation (EUROSTAR), however, owing to stent stenosis of the device branch in the area of the iliac vessel. This can be primarily traced back to an increased rigidity of the inflamed vessels. On the other hand, the secondary cause appears to be the triggering of an inflammatory episode after manipulation and finally through contact with the reclining endoprosthesis.
The mortality of our own group of patients after EVAR was 0. In the follow-up, four of five patients treated by EVAR repair were still alive (mean follow-up 4 years; range 1.5–5.5 years). The indication for EVAR with IAA corresponded to that of patients with AAs (increased operative risk profile or rupture). Corresponding to the results of recent publications, our patients demonstrated a rigid iliac segment, making the procedure more difficult. On one patient, the bridging maneuver could not be performed after placement of the main body of an endobifurcation. The rigid iliac artery made control of the guidewires impossible. Furthermore, two patients developed endoleaks after EVAR. One patient presented with a type 2 endoleak from the internal iliac artery after implantation of an endobifurcation. On one other patient with rupture, the occluder in the common iliac artery could not be sufficiently placed after aortounilateral iliac stent implantation (with crossover bypass) owing to vessel rigidity with maximum kinking (type 1 endoleak) (see Figure 3).
Despite these technical limitations, the morbidity rate within the group repaired endovascularly was not higher than that of the conventional group. In every case, the complications that occurred after EVAR could be treated with an additional corrective procedure (operation or interventional embolization). With regard to inflammation after EVAR, in one case, the signs of inflammation had completely disappeared at the time of follow-up. The other cases represented a signification regression 1 year after the operation.
Conclusion
Aortic repair of IAA could be performed with the same mortality rate compared with AAs. Para-anastomotic aneurysm does not represent a disease-typical complication after inflammatory aortic repair. A number of cases resulted in a significant regression or complete disappearance of the signs of inflammation after the operation. Endovascular treatment of IAA represents a feasible alternative surgical procedure.