
Abstract
Popliteal artery aneurysms are relatively uncommon but potentially limb-threatening lesions that can thrombose or cause distal embolization. Identification of these aneurysms, especially in patients with abdominal aortic aneurysms, is imperative, and prophylactic treatment with either surgical exclusion and bypass or endoluminal stent grafting is critical to prevent these poor outcomes. Endovascular approaches currently using the Viabahn stent graft offer several advantages, including a minimally invasive approach, fewer perioperative complications, and a faster recovery. This must be balanced with a potentially higher failure rate or requirement for reintervention, although contemporary series report comparable short-term outcomes. We present our approach to the evaluation and diagnosis of popliteal aneurysms, the technical aspects of endovascular popliteal aneurysm repair, and a representative case study.
Keywords
Endovascular treatment for popliteal artery aneurysms has gained public exposure following the repair of bilateral aneurysms in Vice-President Dick Cheney using a minimally invasive stent graft approach in September 2005. 1 Although the true prevalence of popliteal artery aneurysms is not clearly known, it is thought that they account for 70 to 80% of all peripheral aneurysms. 2,3 In a recent study using duplex ultrasonography, the normal popliteal artery in men aged 50 years and older measured 6.8 mm on average, 4 which is smaller than previously thought 5 but consistent with other recently published series. 6–9 As expected, normal popliteal arteries in women measured smaller, at 6.0 mm on average. By comparison, they found the average diameter of male aneurysmal popliteal arteries to measure 15.7 mm, with maximal dilation found in the mid–popliteal artery segment. Therefore, by way of definition, any popliteal artery with focal dilation of 1.5 cm or greater in maximal diameter may be considered an aneurysm for the purposes of treatment planning. Popliteal aneurysms occur more frequently in men than in women, with a ratio perhaps as high as 19:1. 3 There is a clear association between popliteal and abdominal aortic aneurysms (AAAs). Based on several studies, the prevalence of popliteal aneurysms in patients with known AAA ranges between 2.4 and 10%. 5,8,10 Conversely, an AAA is found in 36 to 50% of patients with a popliteal aneurysm, and popliteal aneurysms are bilateral in approximately 50% of cases. 3,5,10
The natural history of popliteal aneurysms likewise is not well defined. Small aneurysms (1.5–2.0 cm) are likely to be asymptomatic and therefore may go largely undiagnosed. Like aneurysms in other locations, if left untreated, popliteal aneurysms will expand with time. Although not well documented, it is estimated that popliteal aneurysms expand by approximately 10%/year. Pittathankal and colleagues, using serial duplex surveillance of 24 popliteal aneurysms, reported that aneurysms < 2 cm grew on average by 1.5 mm/yr, those 2 to 3 cm in size grew by 3 mm/yr, and those larger than 3 cm grew by 3.7 mm/yr on average. 11 Symptoms are primarily due to thromboembolic complications and distal ischemia, mass effect in cases of large aneurysms, and, rarely, rupture. 2,5,12–16 Several observational studies of asymptomatic popliteal aneurysms suggest that the risk of complications is greatest in aneurysms larger than 2 cm and ranges from 24% at 1 year, to 35% at 4 years, to as high as 74% at 5 years. 5,13,16 Symptoms seem to correlate in some studies with the increasing size of the aneurysm, 17 whereas others have shown smaller aneurysms to be as likely to produce symptoms owing to the mere presence of mural thrombus leading to distal embolization and thrombosis. 18 Previous silent embolic phenomena is also a predictor of worse outcome, with the risk of limb-threatening ischemia increasing from 36% at 3 years in patients with palpable distal pulses to as high as 86% if pedal pulses are absent. 5,19
Recommendations regarding when to intervene for popliteal artery aneurysms vary. 19–24 There appears to be a general consensus that symptomatic popliteal aneurysms should be repaired irrespective of size and that intervention be considered for asymptomatic aneurysms larger than 2 cm in diameter, particularly if they contain significant mural thrombus. Most qualify that intervention be considered for a 2 cm popliteal aneurysm in a “good-risk” patient but that in “high-risk” patients, 2 to 3 cm aneurysms may be safely observed if closely followed. 22 Minimally invasive endovascular approaches may be particularly well suited for this latter subset of patients. Given that the severity of outcomes associated with symptomatic popliteal aneurysms includes a risk of major amputation as high as 30 to 40%, 13,14,19 endovascular stent graft repair is an attractive, percutaneous alternative to watchful waiting.
Anatomic considerations for endovascular repair of popliteal aneurysms differ from aortic aneurysms. Whereas the primary limitation for endovascular repair of aortic aneurysms is the presence of an adequate proximal and distal neck, it seems that many popliteal aneurysms are amenable to endovascular approaches based on proximal and distal anatomy. Whereas the proximal and mid–popliteal arteries are susceptible to aneurysmal dilatation, the distal popliteal artery is typically uninvolved. A mean distal popliteal artery diameter even in patients with popliteal aneurysms of 6.4 mm makes stent graft repair feasible in most cases. 4 Therefore, the primary anatomic limitation for endovascular popliteal aneurysm repair may be the presence or absence of adequate tibial runoff. The first endovascular popliteal aneurysm repair was reported by Marin and colleagues in 1994 using a homemade noncommercial stent graft. 25 Since then, several single-institution experiences have been reported documenting high technical success and low complication rates and shorter hospital stays associated with endovascular popliteal aneurysm repair. 26–30 In all cases, the technical success of the procedure ranged from 96 to 100%. Patency rates in early experiences ranged from 47 to 78% primary patency and 75 to 86% secondary patency at 1 year, whereas more contemporary experiences report rates of 80 to 96% primary patency and 90 to 100% secondary patency at the same interval. This can be compared with reported patency rates of open popliteal aneurysm repair of 90 to 100% 1-year and 77 to 100% 5-year primary patency. 2,13,21,31–35 Factors associated with improved success with endovascular repair include operator experience, improvements in stent graft design, clopidogrel use, elective repair, and distal runoff.
Few level I data are available, but the results from one small prospective randomized trial comparing open and endovascular repair of asymptomatic popliteal artery aneurysms were recently reported. 36 In this study, they randomized 30 aneurysms in 26 patients with asymptomatic popliteal aneurysms ≥ 2 cm with suitable anatomy for either an open or endovascular approach, 15 to open and 15 to endovascular repair. Open repair included a medial approach in all cases, with reversed great saphenous vein bypass in the majority (73%) and prosthetic bypass (27%) reserved for those with inadequate autogenous conduit. The Hemobahn stent graft (W.L. Gore, Flagstaff, AZ) was used exclusively for all endovascular repairs. Technical success was 100% in both treatment arms. They reported 100% 1-year primary patency in the open cohort and 87% primary, 100% secondary 1-year patency in the endovascular cohort. They experienced only one stent graft thrombosis in the endovascular group occurring on the first postoperative day owing to technical difficulties at the time of implantation. This patient was successfully treated with an additional endovascular procedure. Three-year patency rates of 91% and 80% were reported for the open and endovascular approaches, respectively. Despite their small numbers, the authors concluded that both procedures were equally effective and safe in the treatment of popliteal aneurysms. The endovascular group demonstrated shorter operative times, shorter hospital stays with less perioperative morbidity, and faster recovery.
Technique
Imaging
Preoperative imaging consists of noninvasive duplex ultrasonography as the initial study to determine diameter measurements, delineate the extent of arteriomegaly, detect the thrombus burden within the aneurysm, and assess distal runoff. 4,37 Computed tomographic angiography (CTA) with three-dimensional reconstruction has also become important for preoperative case planning (Figure 1). 38–41 Conventional angiography (Figure 2) is usually reserved for acute cases in which thrombolysis may be a consideration or when the status of tibial runoff needs to be delineated.

A three-dimensional computed tomographic reconstruction (TeraRecon, Inc., San Mateo, CA) of a lower extremity computed tomographic angiogram showing both a common femoral artery aneurysm proximally and a popliteal artery aneurysm distally.

Angiographic imaging of the lower extremities in a patient with bilateral popliteal aneurysms. Note the left aneurysm thrombosed acutely, leading to limb threat and the requirement for emergent bypass. The right remains patent but demonstrates significant tortuosity of the popliteal artery and demonstrated evidence for chronic distal embolization (not shown).
Setting
All procedures in the authors' institution are performed by endovascularly trained vascular surgeons working in an operating room equipped with a fixed angiographic suite (Infinix, Toshiba America, New York, NY). Either local anesthesia with sedation or continuous spinal anesthesia is used for all cases.
Access
In contrast to most percutaneous infrainguinal interventions in which a contralateral approach is favored, antegrade ipsilateral femoral access is preferred for endovascular popliteal aneurysm repair. The devices required for this procedure typically require 8F or larger introducer sheaths to be advanced into the superficial femoral artery (SFA). Even with stiff guidewire support, in the presence of significant iliac ectasia, common in these patients, especially with concomitant aortic aneurysms, these large-diameter sheaths can pose a challenge during advancement over the aortic bifurcation. Furthermore, if an AAA has been previously repaired with a bifurcated graft or an endograft, this would preclude a contralateral approach.
Stent Grafting
Currently, the only covered stent graft that has a peripheral vascular indication is the Viabhan stent graft (W.L. Gore; Figure 3). It is constructed of expanded polytetrafluoroethylene graft material with a continuous external nickel-titanium (nitinol) stent framework with minimal inter-ring junctions, resulting in significant flexibility with considerable radial force. It has significant improvements over its predecessor, the Hemobahn, in that it is 0.035- or 0.025-inch guidewire compatible, has concentric expansion rather that spiral unfolding, and has a distal to proximal deployment mechanism offering better precision. Overall, Viabahn sizes range from 5 to 13 mm in diameter with 2.5 to 15 cm lengths, although only the 6 to 8 mm–diameter devices are approved for use in the femoropopliteal segment. The 6 to 8 mm grafts are delivered through an 8F or 9F guide sheath, depending on the diameter.

Viabahn stent graft from W.L. Gore demonstrating its expanded polytetrafluoroethylene graft material with a nickel-titanium exoskeleton. The range of diameters and lengths is shown, as well as its flexibility. Courtesy of W.L. Gore and Associates, Inc.
Stent graft sizing is initially based on measurements taken from preoperative CTA with three-dimensional reconstruction. The device is relatively intolerant of oversizing, therefore, precise diameter measurements and balloon postdilation are important for full expansion and apposition of the device to the vessel wall. In general, graft diameter is selected, allowing for 10% oversizing to minimize the risk of infolding. As in endovascular repair of other aneurysms, there must be suitable proximal and distal landing zones of at least 20 mm of nonaneurysmal femoropopliteal artery. Therefore, length selection is based on a minimum of 20 mm seal above and below the popliteal aneurysm and 20 to 30 mm overlap between stents if more than one device is required. These measurements are confirmed with intraoperative arteriography. Of note, because of the significant longitudinal mobility and flexion-torsion that can occur in this arterial segment, if the anatomy permits, the devices should ideally be deployed a minimum of 5 cm proximally into the nonaneurysmal SFA and to the distal-most segment of the infrageniculate popliteal artery. The concern for crossing the knee joint should not impact the decision to land the device as distally as possible.
Through a small transverse groin incision, the anterior aspect of the common femoral artery is exposed. No attempt is made to circumferentially dissect and control the artery. A 5-0 polypropylene purse-string suture is placed on the anterior aspect of the artery to facilitate later closure of the arteriotomy. Arterial puncture is made under direct vision precisely in the center of the purse-string, and the guidewire is directed into the SFA. After insertion of an appropriately sized introducer sheath, a lower extremity runoff is obtained to determine the patency of the tibial outflow. A 0.025- or 0.035-inch guidewire is directed preferentially into the peroneal artery if patent but may be introduced into any of the other patent tibial vessels. The patient is fully anticoagulated with intravenous heparin (100 IU/kg initial dose) to maintain an activated clotting time in excess of 250 seconds. The stent graft is inserted and positioned using roadmap imaging and deployed with the distal end proximal to the anterior tibial artery origin. Additional stent grafts are deployed proximally with 20 to 30 mm of junctional overlap to securely seat the proximal end of the stent graft in the nonaneurysmal segment of the SFA or suprageniculate popliteal artery. The proximal and distal landing zones and interstent junctions are postdilated with standard angioplasty balloons.
Completion arteriography, including runoff images, is performed.
Follow-Up
All patients are recovered in a postanesthesia care unit and then admitted to the general surgical care ward for observation overnight. They are discharged the following day when able to ambulate and tolerate diet. They are reevaluated in the outpatient clinic in 4 weeks. Physical examination, ankle-brachial indices, and duplex ultrasonography 42 are obtained for postoperative surveillance at this initial postoperative visit and then at 6-month intervals. The patients are maintained on antiplatelet therapy with clopidogrel and aspirin indefinitely.
Case Study
A 78-year-old male with a remote history of aortobiiliac reconstruction for an infrarenal aortic aneurysm and a right leg bypass for a popliteal aneurysm, both done at an outside institution, was referred to the University of Florida Teaching Hospital for the evaluation of further aneurysm development, including iliac, femoral, and popliteal aneurysms. Computed tomography revealed multiple peripheral aneurysms, including a 3 cm left femoral and a 4.5 cm left popliteal aneurysm (see Figure 1).
He underwent conventional open left femoral artery reconstruction with a Dacron interposition graft and, at the same setting, endovascular repair of the left popliteal aneurysm. A 12F sheath was placed in an antegrade fashion through the femoral graft. Initial angiography confirmed the preoperative CTA findings (Figure 4). Three Viabahn endoluminal stent grafts placed distal to proximal were then used to repair the aneurysm (Figure 5). The devices included a 9 × 100 mm and two 10 × 100 mm grafts from distal to proximal to completely exclude the aneurysm. The larger size was sequentially placed inside the smaller-sized graft for adequate device to device seal, and grafts were sized according to the native anatomy. A minimum of 20 mm overlap was allowed between each stent, and a minimum of 20 mm seal above and below the aneurysm was achieved. There was no periprocedural endoleak. Duplex ultrasonography follow-up at 6 months revealed the patency of his stent graft without complications.
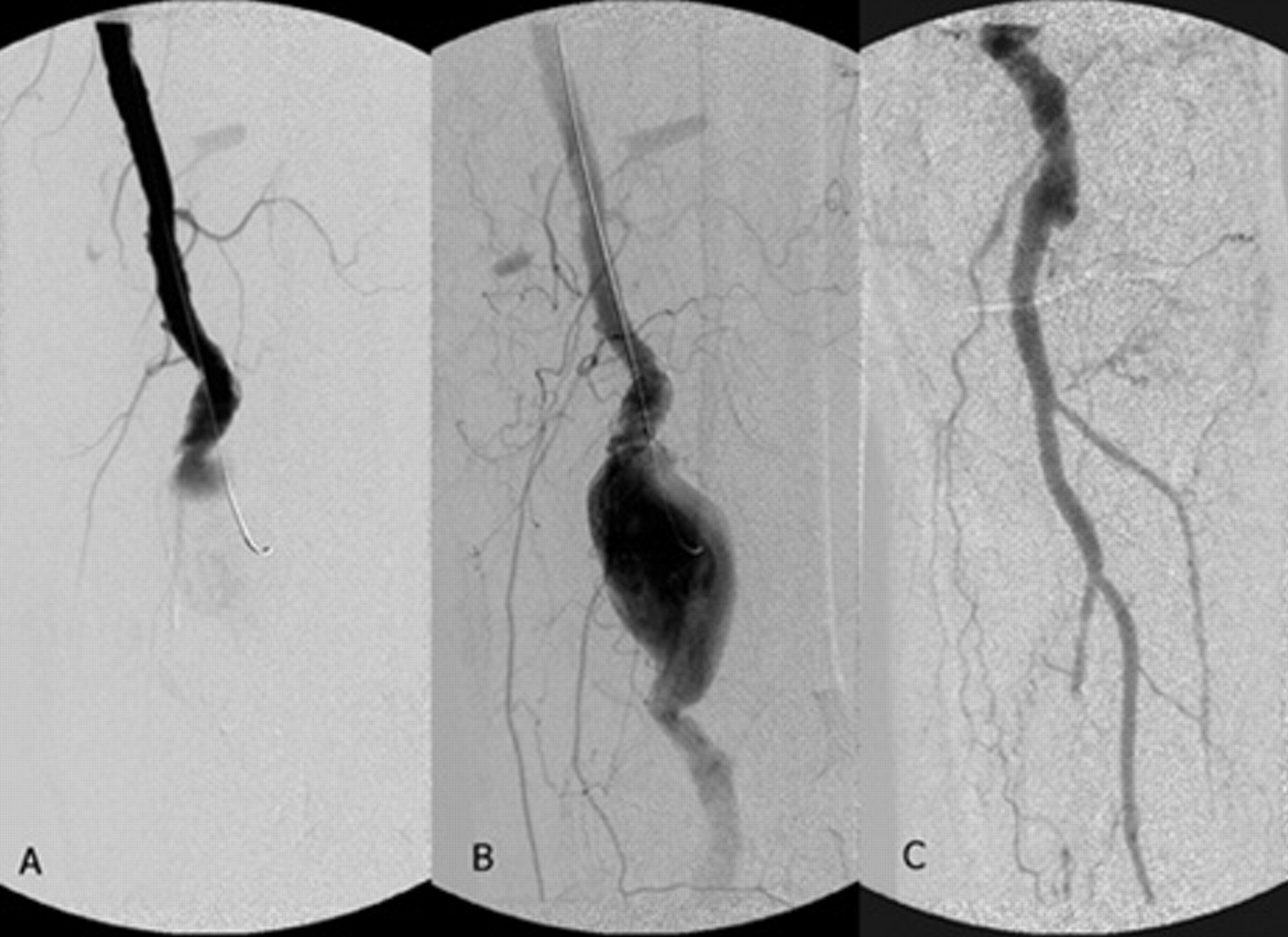
Case images: preintervention angiogram of a patient with a left popliteal artery aneurysm. The proximal superficial femoral artery appears to be normal, with minimal tortuosity or ectasia (A). Patent popliteal aneurysm depicted in the above-knee segment (B) with two-vessel tibial runoff with evidence of chronic embolization to the posterior tibial artery (C).
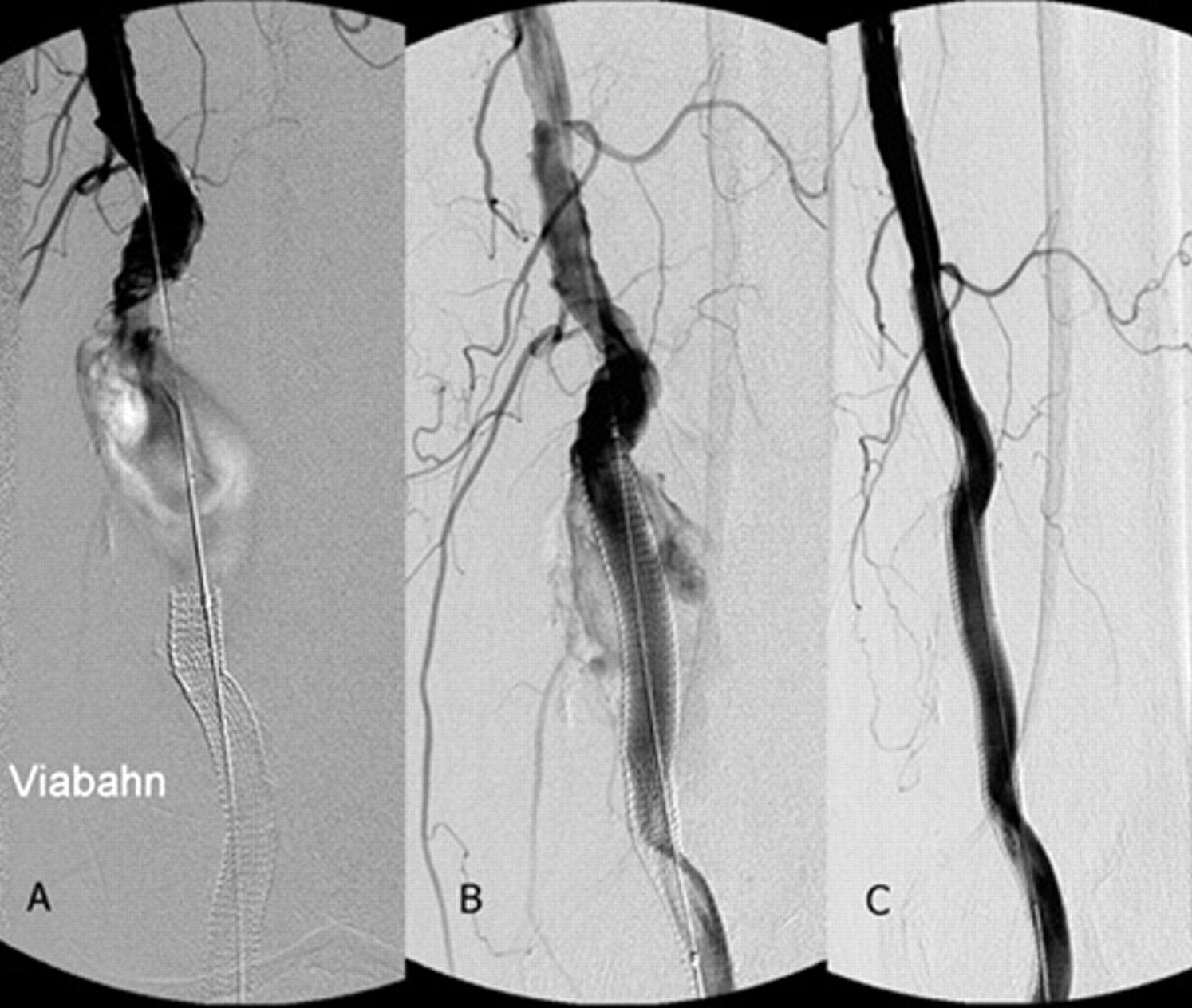
Case images: following stent graft repair of the same patient shown in Figure 4. The first stent was placed with adequate distal purchase (A), the second stent with exclusion of the aneurysm (B), and the third and final stent for proximal purchase with successful exclusion of the aneurysm on a completion angiogram (C).
Discussion
In 1998, Burger and colleagues first reported the use of the Hemobahn stent graft for treatment of a popliteal artery aneurysm. 43 In this small case series, they reported the successful treatment of three lesions: an iatrogenic popliteal pseudoaneurysm and arteriovenous fistula, popliteal entrapment syndrome, and a degenerative popliteal aneurysm. All cases were successfully performed percutaneously using 6 and 7 mm–diameter devices. Since then, larger series have further documented the successful use of Hemobahn and Viabahn for endoluminal exclusion of popliteal artery aneurysms ranging from 1.5 to 6.5 cm in diameter. 27,28,30,36 Symptomatic and asymptomatic and elective and urgent cases have all been reported. From these experiences, open antegrade exposure for access is favored, although successful percutaneous repair has been reported. All authors emphasize meticulous measurement of the proximal and distal landing zone diameters and lengths using a combination of duplex ultrasonography and CTA. Some authors advocate prophylactic coil occlusion of geniculate branches originating from the aneurysm sac to prevent type 2 endoleak, but endoleak has been rare even without this preemptive approach. Others caution to prevent stent fracture, kinking, or migration and avoid landing a stent graft or an overlap zone between stents in the “bending zone” of the knee, which correlates with the upper margin of the patella radiographically. In addition, at least 2 cm of seal in the distal popliteal artery below the knee joint proper seems optimal. With these approaches, device thrombosis, kinking or fracture, separation, and migration have rarely been observed. Other factors associated with success include operator experience, the quality of tibial outflow, improvements in stent graft design, and the use of clopidogrel antiplatelet therapy.
Because of the potential for limb-threatening complications, little disagreement exists that all symptomatic and most asymptomatic popliteal artery aneurysms ≥ 2 cm in diameter, especially those containing mural thrombus, warrant repair. Controversy does exist over the optimal treatment approach. 26,44 Open surgical exclusion and bypass have been standard therapy, with long-term patency rates in excess of 75 to 90% and low surgical mortality of 0 to 2% but potentially high morbidity rates of 30 to 40% from wound and other complications. Endovascular popliteal artery aneurysm repair is technically feasible and safe, with less perioperative morbidity than, and with early outcomes comparable to those of open popliteal aneurysm repair. The majority of popliteal aneurysms are anatomically appropriate for endovascular repair, it can be performed under local or regional anesthesia in most cases, and a 1-day hospital stay is standard for elective cases. Its main limitations are (1) profile of the devices requiring at least an 8F or 9F guide sheath and (2) the limited success of nitinol-based stents across the knee joint susceptible to fracture and kinking leading to thrombosis. With the advent of smaller-profile, more flexible, fracture-resistent devices and the evolution of percutaneous arteriotomy closure approaches, these limitations can be overcome. Endovascular popliteal artery aneurysm repair can no longer be considered an experimental procedure. Rather, it is now an important aspect of the treatment of patients with complex aneurysmal disease as that presented here in our representative case study.