
Abstract
Carotid angioplasty and stenting are progressively earning a role as a less invasive alternative in the treatment of carotid occlusive disease. The most common approach for carotid artery stenting involves transfemoral access and use of a filter or balloon device for neuroprotection. This approach has limitations related to both the site of access and the method of neuroprotection. Specifically, an aortoiliac segment with advanced occlusive or aneurysmal disease or an anatomically unfavorable or atheromatous arch and arch branches can significantly limit the safety of the retrograde transfemoral pathway to the carotid bifurcation. Additionally, data provided by the use of transcranial Doppler monitoring and diffusion-weighted magnetic resonance imaging in patients undergoing filter- or balloon-protected carotid artery stenting demonstrate that currently available devices are associated with a considerable incidence of cerebral embolization. To address these limitations, we, along with others, have employed a direct transcervical approach for carotid artery stenting that incorporates the principle of flow reversal for neuroprotection. The technique bypasses all of the anatomic limitations of transfemoral access and simplifies the application of flow reversal, which is one of the safest neuroprotection techniques. The purpose of this review is to describe our method of transcervical carotid artery stenting, review the accumulating outcomes data, and discuss the clinical advantages of and indications for this increasingly popular technique.
Carotid angioplasty and stenting (CAS) are progressively earning a considerable role as a less invasive alternative for stroke risk reduction in patients with carotid artery stenosis. The percutaneous transfemoral approach has been the preferred approach for access to the extracranial carotid arteries in the majority of the CAS trials published in the past. However, adverse anatomic situations, including severe aortoiliac occlusive or aneurysmal disease, poor aortic arch or arch branch anatomy with advanced atheromatous disease, and common carotid artery coiling and kinks, can significantly limit the safety of transfemoral catheter delivery for treatment of the diseased carotid artery (Figure 1). Furthermore, although distal filter and balloon occlusion devices are the most commonly used neuroprotection systems, data provided by the use of intraoperative transcranial Doppler (TCD) monitoring and diffusion-weighted magnetic resonance imaging (MRI) demonstrate a significant incidence of bilateral cerebral embolization in filter- or balloon-protected CAS.
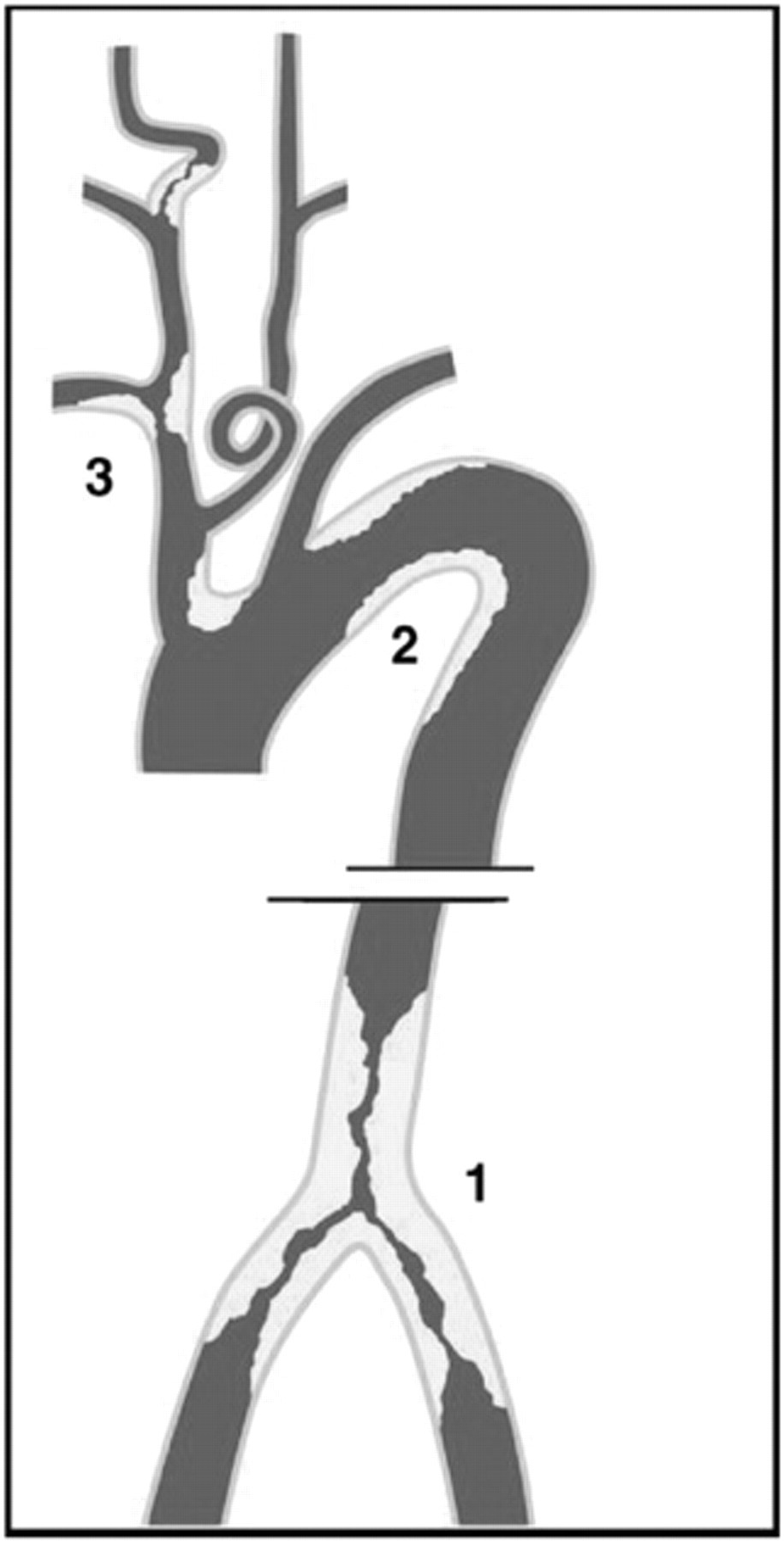
Pitfalls of transfemoral access for carotid angioplasty and stenting. Transfemoral access and delivery of sheaths to the common carotid artery (CCA) may be limited by anatomic problems. (1) At the level of the aortoiliac segment: advanced occlusive or aneurysmal disease and tortuosity. (2) At the level of the aortic arch: significant elongation of the arch, with the takeoff of the supra-aortic trunks located lower than the superior arch border; atheromatous disease; or anatomic anomalies, such as bovine takeoff of the left CCA. (3) At the level of the supra-aortic trunks and CCAs: acute takeoff angles, anatomic anomalies, substantial occlusive disease, and tortuosity. Reproduced with permission from Pipinos II et al. 6
To address the limitations and risks posed by transfemoral access and the currently available protection devices, our group, as well as others, has employed a direct transcervical approach for CAS that incorporates the flow reversal principles described by Parodi and colleagues for neuroprotection. 1–8 The purpose of this review is to describe our method of transcervical CAS with flow reversal, review the available data on its application, and discuss the clinical advantages of and indications for this alternative CAS technique.
Description of Technique
Preoperative Workup
Every candidate for the transcervical approach undergoes complete assessment of the aortic arch, arch branches, and extra- and intracranial circulation with carotid or vertebral duplex imaging and computed tomographic angiography (CTA) or magnetic resonance angiography (MRA). These noninvasive tests establish the severity and morphology of the internal carotid artery (ICA) stenosis and delineate the anatomic details of the arteries supplying the brain. Theoretically, flow reversal may pose problems for patients with occlusion of the contralateral ICA or vertebral arteries and/or poor intracranial collaterals. In our practice, patients with poor collaterals (≅10%) on preoperative imaging are identified and have either endarterectomy or filter-protected transfemoral or transcervical CAS. If the patient and surgeon choose to proceed with the transcervical approach, a test ICA reversal is attempted. If the patient tolerates it, then CAS is performed with flow reversal; otherwise, the transcervical CAS is completed with the use of a filter device for neuroprotection.
Preoperative Preparation
All patients are treated with clopidogrel (75 mg/d) and aspirin (325 mg/d) for at least 1 to 2 weeks prior to the operation. Patients with renal insufficiency (creatinine ≥ 1.4 mg/ dL) are given N-acetylcysteine (Mucomyst) before and after the procedure in addition to a periprocedural bicarbonate fluid solution. Anesthesia is based on the preference of the patient and anesthesiologist, with local or regional anesthesia being the preferred method for patients at a higher cardiopulmonary risk.
Patient Positioning and Neck Evaluation with Portable Ultrasonography
The procedure is performed in the operating room with an OEC 9800 portable C-arm with a 12-inch image intensifier (OEC Medical Systems, Salt Lake City, UT) and a carbon fiber table with a four-way motorized tabletop (Allegro 6800 Mobile Imaging Table, Orthopedic Systems, Inc., Union City, CA). With the patient supine on the angiographic table, a portable ultrasound device is used to identify the proximal common carotid artery (CCA), just above the clavicle, and the CCA bifurcation. Both of these positions are marked on the neck, and the relative length of the CCA available for cannulation is identified. The patency of the contralateral internal jugular (IJ) vein is verified, and its location is marked. The patient's lower face, lower aspect of the ears, neck, and chest to the nipples are then prepared and draped in the standard fashion.
Contralateral IJ Vein Cannulation, CCA Access, and Initial Arteriograms
A 9F, 10 cm–long introducer (Pinnacle, Boston Scientific, Natick, MA) is inserted in the contralateral IJ vein using real-time ultrasonographic guidance and standard percutaneous technique (Figure 2). The sheath is secured in place with a silk suture. The contralateral IJ vein is preferred because it keeps the venous sheath away from the primary operative site. A 2 to 3 cm transverse incision is then made directly over the ultrasonographically identified CCA (which usually, but not always, is directly underneath the sternal head of the sternocleidomastoid muscle), 2 cm cephalad to the clavicle. The sternal head is retracted laterally, and dissection proceeds longitudinally through the underlying fat pad to the carotid sheath. In our initial experience, we separated the sternal and clavicular heads of the sternocleidomastoid muscle and dissected transversely until we reached the carotid sheath. We now feel that simple lateral retraction of the sternal head of the muscle combined with a longitudinal dissection through the sternocleidomastoid fat pad allows for similar exposure with less dissection and appears to minimize oozing from the operative site. The carotid sheath is entered with caution to avoid injury to the vagus nerve. In our experience, the vagus at this level is usually located posterolaterally, with the IJ vein usually positioned anterolaterally and the CCA posteromedially. Only once did we see the vagus in an anterior position at this level. The CCA is dissected circumferentially for 2 to 3 cm and encircled with a vessel loop (see Figures 2 and 3). Following that, a U-shaped, full-thickness 6-0 polypropylene suture is placed through the wall of the proximal CCA precisely at the level where the arterial access will be established. The artery is then accessed with a micropuncture introducer set (Cook Inc., Bloomington, IN), making certain that the wire and minisheath stay below the CCA bifurcation. If the working CCA length is less than 6 cm, a different guidewire that has a shorter (2 cm) flexible tip (0.014-inch, 80 cm Nitrex, EV3 Inc., Plymouth, MN) is preferred. The sheath enters the skin just below the ipsilateral clavicle and is advanced over the clavicle and through the subcutaneous tissues to enter the CCA (under direct vision) at the level of the U stitch. Using the micropuncture minisheath for contrast injection, a ‘‘best view'' cervical carotid angiogram (usually 30° ipsilateral oblique) is obtained. Additional obliquity may be required for ideal separation of the external carotid artery (ECA) and ICA at the level of the CCA bifurcation. Using this roadmap, a 0.035-inch sizing guidewire (Magic Torque, Boston Scientific) is placed in the third-order branches of the ECA. The micropuncture sheath is then exchanged for a 9F sheath (Flexor Check-Flo Introducer, Large Valve Assembly Cook Inc., Bloomington, IN, or Super Arrow-Flex, Arrow International, Reading, PA), and the tip of the sheath is advanced into the mid-CCA below the carotid bifurcation. The sheath is secured in place with two silk sutures. Because the tip of the arterial sheath may fray as it is advanced through the subcutaneous tunnel, making entry into the CCA potentially more traumatic, we start by placing a 12F sheath (Cook Inc.) in the tunnel and cut it just above the skin. We then use this sheath segment as a tunnel to guide and protect the sheaths placed in the CCA. Heparin is then given to elevate the activated clotting time to a level between 250 and 300 seconds. 9 Ipsilateral intracranial arteriograms in lateral and anteroposterior views and a repeat arteriogram of the carotid bifurcation are obtained. After appropriate calibration based on the Magic Torque guidewire markers, the diameter of the CCA and ICA and the length of the stenosis are measured for selection of an appropriately sized stent (we most commonly use the 8 or 10 mm–diameter Carotid Wallstent Monorail [Boston Scientific]) and balloon (we most commonly use the 5 or 6 mm–diameter Ultra-soft SV Monorail Balloon Dilatation Catheter [Boston Scientific]).

A, An introducer sheath is percutaneously placed in the contralateral internal jugular vein (IJ). Access to the common carotid artery (CCA) is established via a 2 to 3 cm transverse incision. A micropuncture set is used to obtain an initial arteriogram and place a 0.035-inch sizing guidewire in the tertiary external carotid artery (ECA) branches. B, A second sheath is placed over the wire in the CCA and flow in the internal carotid artery is reversed and shunted (arrows) into the IJ vein by connecting the side ports of the arterial and venous sheaths after clamping the CCA proximal to the entry site of the sheath. If collateral flow from the ECA results in forward internal carotid artery (ICA) flow or flow stagnation and incomplete emptying (rarely encountered), the ECA is occluded using an over-the-wire arterial embolectomy catheter. Adapted with permission from Pipinos II et al. 6
Cerebral Protection
The CCA proximal to the entry site of the sheath is clamped, and then the CCA sheath side port is connected to the port of the IJ sheath using a double male Luer-lock adapter (Medline, Mundelein, IL), which allows passive direct flow from the CCA to the lower pressure IJ venous system. Using subtraction angiography and short contrast injections through the CCA sheath, the flow reversal is then confirmed by evaluating the retrograde flow of contrast into the IJ vein (see Figures 2B and 3B). In about 15% of the cases, collateral supply from the ECA allows forward ICA flow or flow stagnation and incomplete emptying despite CCA clamping and a functional arteriovenous fistula, thus precluding adequate cerebral protection. In these cases, the ECA is occluded (see Figure 3) using a 4F over-the-wire arterial embolectomy catheter (Arrow International). At this time, with the ECA intraluminally occluded and with the fistula turned off, the carotid occlusion pressure can be easily measured to indicate the adequacy of cerebral perfusion. Stenting and postdilatation are then performed under continuous flow reversal. In patients with soft symptomatic plaques, we occasionally use active suction using a 60 cc syringe to supplement passive flow reversal because it has been postulated that these particular plaques may be more prone to atheroembolism. 10 In these cases, active suction is used at the time of stent positioning and deployment and at the time of deflation of the postdilating balloon.
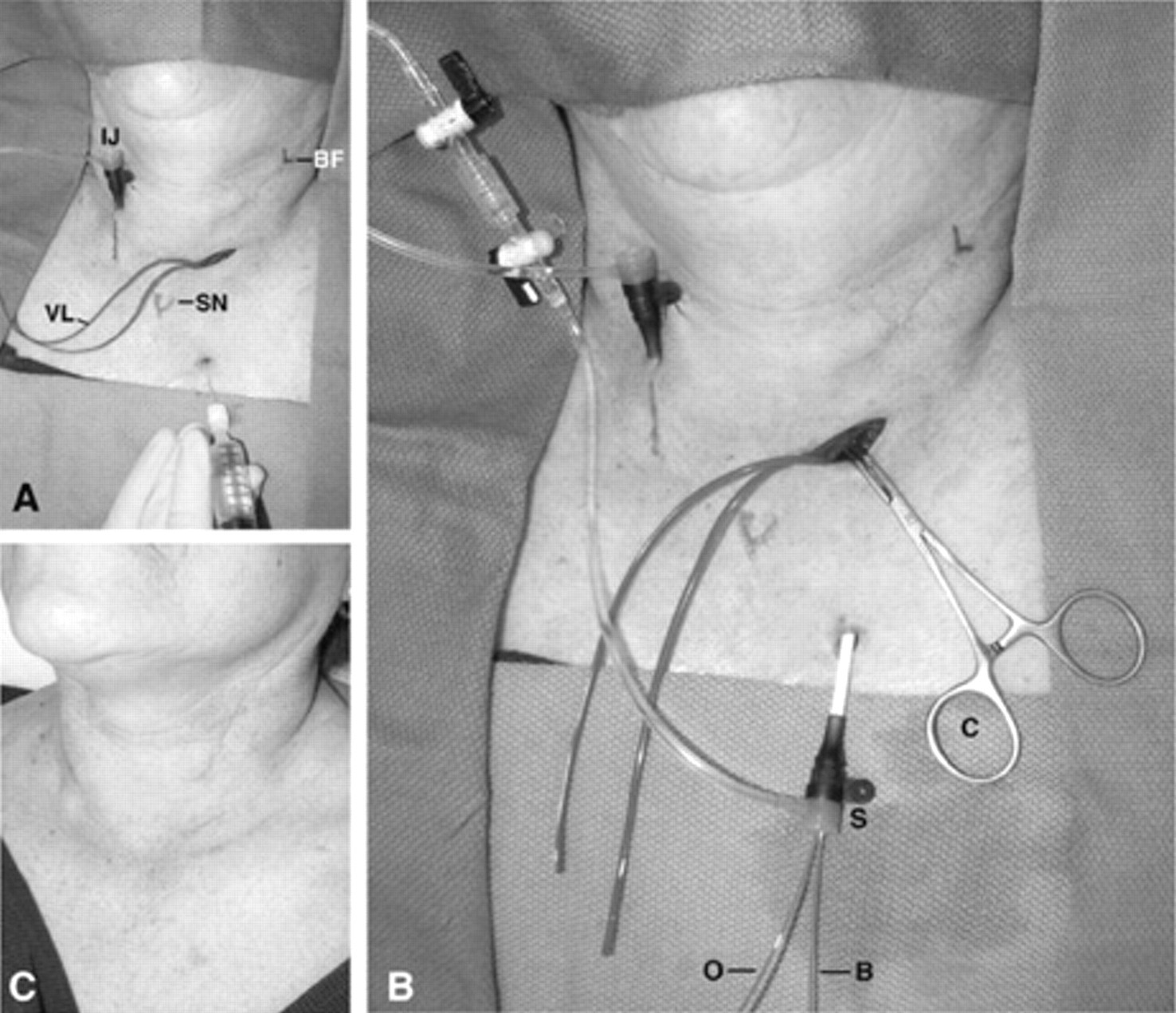
Patient with symptomatic recurrent stenosis 9 months after left carotid endarterectomy. A, In this patient, an introducer sheath is percutaneously placed in the contralateral internal jugular (IJ) vein. The common carotid artery (CCA) is accessed via a 2 to 3 cm transverse incision, carefully dissected, and controlled with a vessel loop (VL). A micropuncture set is used to obtain an initial arteriogram. Please note that the introducer enters the skin just below the ipsilateral clavicle and is advanced over the clavicle and through the subcutaneous tissues to enter the CCA under direct vision at the level of the cutdown. B, As described in Figure 2, internal carotid artery flow reversal is established by connecting the side ports of the arterial (S) and venous sheaths after placing a clamp (C) on the CCA proximal to the entry site of the arterial sheath. An over-the-wire embolectomy catheter (O) was used to occlude the external carotid artery (required in only 15% of the cases). Note that the arterial sheath (S) is large enough to accommodate both the embolectomy catheter and the stent delivery or balloon catheter (B) while allowing an adequate channel for flow reversal. C, The patient at the time of her 1-month follow up. The mini–cutdown incision is barely visible at the base of the neck, below the older carotid endarterectomy incision. BF = carotid bifurcation; SN = sternal notch.
Stenting and Postdilation
With flow reversal established, the ICA stenosis is crossed using a flexible 0.014-inch guidewire (0.014-inch, 80-cm Nitrex; EV3 Inc., Plymouth, MN, USA); the stent is positioned under roadmapping, deployed, and balloon dilated. One or 2 minutes prior to stent deployment, we administer 0.5 mg of atropine intravenously to prevent the reflex bradycardia frequently seen with carotid bulb manipulation. The balloon is then slowly deflated over several seconds and removed under fluoroscopic guidance. Completion cervical and intracranial arteriograms are then obtained.
Once satisfactory treatment of the stenosis is confirmed, the arterial sheath and wire are removed. The CCA is then bled, backward and forward, through the arterial puncture site to flush out any debris that may have accumulated in front of and behind the CCA clamp site (between the CCA origin and the CCA clamp, as well as between the CCA clamp and the tip of the sheath). The arterial puncture site is repaired with the previously placed U stitch.
Wound Closure
A moderate amount of oozing from the dissected soft tissues under the sternocleidomastoid muscle may be encountered owing to the blunt dissection under heightened anticoagulation; thus, mild compression and thrombin-soaked Gelfoam are applied on the oozing surfaces. Unless the oozing stops completely, a small drain is placed through the arterial sheath skin puncture site because a significant hematoma may develop in the setting of intense antiplatelet therapy. The platysma is approximated with interrupted Vicryl sutures, and the skin edges are approximated in a subcuticular fashion (see Figure 3C). A sterile occlusive dressing is placed over the closed incision. Heparinization is allowed to taper physiologically, and reversal with protamine sulfate is avoided. The IJ sheath is removed in the recovery room with the patient upright to minimize the hydrostatic pressure at the puncture site.
Review of Available Clinical Data on the Transcervical Approach with Flow Reversal
In the last 2 years, several publications from four groups have successfully described the technique for transcervical CAS and established its safety, effectiveness, and multiple conceptual advantages over percutaneous femoral options (Table 1). Chang and colleagues first used the transcervical approach to perform CAS after failing to establish CCA access using the transfemoral technique owing to the tortuosity of the proximal left CCA. 1 After this, the same authors performed a clinical study to evaluate the results of the transcervical approach on 20 patients. Compared with our technique, Chang and colleagues' approach is different in two details: these are the use of an ipsilateral (rather than contralateral) IJ sheath for venous access and the use of a second arterial sheath when ECA occlusion is necessary. There were no technical failures, and the stroke and mortality rate at 30 days was 0%. Angiographic confirmation demonstrated resolution of all stenoses. There were no access-site complications or hematomas. All operations were done under local anesthesia. All patients tolerated continuous ICA flow reversal without any problems. Follow-up at 12 months showed the patency of the treated ICA, without evidence of recurrent stenosis. The authors concluded that their series demonstrated the safety and many conceptual advantages of the technique over percutaneous femoral approaches or carotid endarterectomy.
Clinical Data on Transcervical Carotid Angioplasty and Stenting with Flow Reversal for Neuroprotection
See text for additional details.
*Lin and colleagues reported three technical failures (defined as residual stenosis of greater than 30% after carotid stenting and angioplasty). They all underwent endarterectomy.
†Chang and colleagues reported one episode of amaurosis fugax; Criado and colleagues reported two episodes of transient upper extremity paresis; Lin and colleagues reported two transient ischemic attacks.
‡Chang and colleagues reported one patient with hoarseness; Criado and colleagues reported two wound hematomas (one required surgical drainage; in our series, there were five wound hematomas, and one required surgical drainage); Lin and colleagues had two cervical hematomas (one required surgical drainage).
§Criado and colleagues reported one asymptomatic occlusion of the carotid stent at 1 month; our group had one similar event.
At present, Criado and colleagues have the largest reported experience with this technique. 2–4,7 Compared with our technique, their approach is different in two details: the use of an ipsilateral (rather than contralateral) IJ sheath for venous access and the use of a longitudinal rather than a transverse incision for the CCA exposure. At the time of their last report, 90 patients had undergone transcervical CAS, whereas data analysis was complete for the first 50 patients. 7 All patients were preoperatively evaluated with duplex ultrasonography of the extracranial carotid and vertebral arteries only. The procedure was performed under local anesthesia in 54% of the patients. In the initial 12 procedures, 1 major and 3 minor distal CCA dissections occurred. The minor dissections did not require additional treatment. The major dissection necessitated repair with an interposition graft. The group has had no subsequent dissections after reducing their arterial access from two arterial sheaths to a single 8F sheath approach. The mean duration of the procedure was 62 minutes, with a mean ICA flow reversal time of 21.4 minutes. Ninety-six percent of the patients tolerated flow reversal without problems; this included all patients with a patent contralateral carotid artery. However, two of seven patients (both had old contralateral strokes) with an occluded contralateral ICA did not tolerate flow reversal. One of these two patients had immediate intolerance to CCA occlusion and underwent CAS without protection. The other patient developed transient loss of conciousness at the end of the operation but recovered immediately on reestablishment of antegrade ICA flow. Early in the group's experience, there was one postoperative ipsilateral hemispheric transient ischemic attack (TIA) with upper extremity hemiparesis and aphasia. An additional intraoperative contralateral hemispheric TIA occurred in a patient with contralateral ICA occlusion, which resolved immediately after reestablishment of antegrade flow. There were no deaths or strokes 30 days following surgery. Only one patient was found to have carotid occlusion on follow-up 1 month after the procedure. All other stents remained patent, without residual or recurrent stenosis, with a mean follow-up of 7 months (range 1–12 months). The authors also reported two wound hematomas, one of which required surgical drainage under local anesthesia. Criado and colleagues concluded that transcervical CAS can be accomplished safely with a low stroke rate, is comparable in outcome to other CAS approaches, and is well tolerated under local anesthesia in most patients.
Our group has performed 38 transcervical CAS procedures on 38 patients to date. Access and CAS were successful in all cases. The initial 17 patients in our series have been previously reported. 6 Twelve procedures were performed under local anesthesia with intravenous sedation, with the remaining under general anesthesia. Flow reversal as a means of cerebral protection was well tolerated by all patients. The mean carotid backpressure measured at the time of flow reversal was 60 mm Hg (range 40–80 mm Hg). The mean operative time was 134 minutes. The mean ICA flow reversal time was 26 minutes (range 12–44 minutes). The patients tolerated the procedure well and had no neurologic events (0% neurologic event rate). Four patients developed small neck hematomas postoperatively. An additional patient developed a larger hematoma requiring operative drainage. All patients were discharged from the hospital on the first postoperative day after carotid duplex ultrasonography demonstrated the patency of the stented carotid artery. There were no deaths or strokes over a mean follow-up of 18 months (range 1–42 months). One patient was found to have an asymptomatic carotid occlusion on follow-up 1 month after the procedure. All other stents remained patent, without residual or recurrent stenosis.
Lin and colleagues prospectively compared, in a nonrandomized fashion, 24 transfemoral and 31 transcervical cases of CAS. 5 Of the 24 transfemoral patients, 2 had neurologic events (1 TIA and 1 stroke). One patient had an asystolic cardiac arrest but was successfully revived with inotropic agents, two patients had groin hematomas, and two had technical failure defined as residual stenosis of greater than 30%. The patients with technical failure were treated with endarterectomy. The total amount of contrast used in the transfemoral approach was 113 ± 39 mL. Of the 31 cases treated using a transcervical approach, 2 patients developed TIAs, 2 had postoperative cervical hematomas, and 3 had technical failure and were also treated with endarterectomy. All failures (with both approaches) appeared to be secondary to incomplete stent expansion owing to circumferentially calcified plaques. All patients had either local or regional anesthesia, and all tolerated ICA flow reversal during the procedure, even though nine patients had contralateral occlusion. The total amount of contrast used in the transcervical approach was 68 ± 18 mL. The authors concluded that the transcervical technique, when compared with the transfemoral approach, is less expensive, requires a smaller amount of contrast and radiation, and shortens the overall procedural time because there is no need for aortic and aortic arch arteriography during the procedure.
Discussion
In the last 10 years, we have witnessed increasing interest in the development and optimization of CAS as an alternative to endarterectomy for stroke risk reduction in patients with carotid artery stenosis. 11–14 To avoid the potential shortcomings of the transfemoral access site and the risks associated with the use of filter and balloon occlusion devices, our team has joined others to describe and evaluate a technique that uses transcervical access and flow reversal for the performance of CAS. 1–7
Why Transcervical Access?
Transfemoral CAS has considerable technical limitations, with reported technical failure rates between 2 and 20%. 15–22 The predominant mechanism of technical failure for the transfemoral approach is the inability to safely navigate the introducer sheath through unfavorable aortoiliac or arch and supra-aortic trunk segments. Specifically, an aortoiliac segment with advanced occlusive or aneurysmal disease and/or an anatomically unfavorable or atheromatous arch and/or supra-aortic trunks can make the retrograde transfemoral pathway to the CCA unnecessarily difficult and unsafe or even impossible (see Figure 1). The greatest advantage of the transcervical approach is the avoidance of these anatomic limitations and the risks associated with remote transfemoral management (Table 2). Equally important as the technical challenge is the concern for atheroembolization at the time of sheath and wire navigation through the arch and supra-aortic trunks. This risk has been extensively confirmed by studies using intraoperative TCD ultrasonography and postoperative diffusion-weighted MRI. In these studies, considerable numbers of microembolic signals were detected not only during stent deployment, predilation, and postdilation but also during sheath placement and guidewire or catheter manipulation. 23,24 Additionally, brain imaging with diffusion-weighted MRI after filter-protected CAS has demonstrated that approximately 50% of the embolic strokes involve territories other than the ipsilateral hemisphere, suggesting that the interaction of catheters and wires with the arch and its branch arteries is potentially responsible for more adverse consequences than initially thought. 24–29 Other approaches described to avoid the limitations of transfemoral access include radial or brachial access, transseptal access, and percutaneous CCA access. 30–34 The radial and brachial artery access does not overcome unfavorable supra-aortic trunk anatomy and provides meaningful advantages on the right side only. The transseptal technique requires special skills and support and again does not avoid the anatomic challenges introduced by an unfavorable or diseased arch and supra-aortic trunks. Finally, percutaneous CCA access is problematic because of an uncomfortably acute angle for the introducer sheath entry and difficult access-site management after sheath removal.
Advantages of the Transcervical Carotid Angioplasty and Stenting Using Flow Reversal for Neuroprotection in Comparison with Transfemoral Access with Filter or Balloon Protection
The proximity of the transcervical access site and the target carotid lesion provides a considerable mechanical advantage, allowing for easier negotiation of tight stenoses and/or a tortuous ICA (see Table 2). Although some may argue that the distance from the puncture site to carotid bifurcation is limited, we have not found this to be an issue, especially when using the micropuncture needle and introducer sheaths for initial access. The transcervical approach allows the use of short and soft guidewires (because extra stiffness is unnecessary), which leads to faster and safer catheter exchanges and permits the use of 0.014-inch systems. Furthermore, the need for predilation is essentially eliminated because no relatively stiff and large neuroprotection devices have to be introduced through the stenotic carotid artery and the maneuverability of all balloon and stent catheters is optimized because of the proximity to the treated lesion. Finally, management of the access site is significantly more straightforward because direct CCA access enables secure suture closure of the artery without the need for reversing anticoagulation.
Shortcomings of the Transcervical Access Site
The main disadvantage of the transcervical approach is the current requirement for open CCA cutdown, making it more invasive than percutaneous access. At this point, open access appears to be the optimal approach for safe CCA access until an appropriate closure device for percutaneous CCA entry is available. Another necessary advancement in that direction would be the customization (significant shortening) of the two flow reversal devices currently available for transcervical application. The two devices, the Parodi antiembolism system (ArteriA device, W.L. Gore, Flagstaff, AZ) and the Mo.Ma Device (Invatec, Roncadelle, Italy), are currently produced in lengths appropriate for the transfemoral approach only. 35,36 Such an adjustment (shortening) of these devices would offer the additional advantage of reduced resistance to flow. 7 A shorter sheath effectively lowers the resistance of the external fistula and allows for easier maintenance of adequate flow reversal in the ICA without the need for ECA occlusion. In our experience, contraindications to the transcervical technique include significant athero-occlusive disease of the CCA at the anticipated level of cannulation, a very low carotid bifurcation, and a large thyroid or goiter or some other anatomic abnormality overlying the CCA at the base of the neck. 7
Why Flow Reversal?
Another significant source of concern for the safe application of CAS stems from the risk of distal embolization of plaque fragments. A recent analysis of results from single-center studies has shown that the use of cerebral protection devices appears to reduce thromboembolic complications during CAS. Specifically, the study found that the 30-day stroke and death rate was 1.8% in 896 patients treated with cerebral protection devices and 5.5% in 2,537 patients treated without protection devices. 37 Similarly, the Safety Committee of the European Endarterectomy Versus Angioplasty in Patients with Symptomatic Severe Carotid Stenosis trial, which has been designed to compare CAS, with or without cerebral protection, with carotid surgery, has recommended limiting the trial to patients with protection during CAS because of an approximately threefold higher incidence of stroke in unprotected CAS. 38 The main neuroprotection techniques being currently used are distal balloon occlusion, distal filtration, and flow reversal. There are four main types of problems with both balloons and filter devices. 39 First, their placement necessitates traversing the plaque without any neuroprotection and frequently requires predilatation that needs to be done prior to neuroprotection. In fact, it appears from studies using intraoperative TCD ultrasonography that it may be exactly this step that is related to the generation of clinically significant emboli. 9–11 Second, the devices may produce spasm, dissection, or other trauma at their deployment site in the ICA. 21,40 Third, at present, they remain relatively stiff, with suboptimal maneuverability. This introduces significant challenges interfering with the safe advancement of these devices through diseased carotid arteries. 7,18 Finally, and probably most importantly, they do not completely eliminate the risk of cerebral embolization even when they are fully deployed. In a study comparing the in vitro efficacy of different filter devices in three carotid anatomic variants (normal anatomy versus mild tortuosity versus severe tortuosity), considerable numbers of emboli were detected in all conditions. The numbers of emboli were directly proportional to the tortuosity of the ICA. 28,36 A series of studies using diffusion-weighted MRI have also described an alarmingly high incidence of “silent” strokes with filter-protected CAS. New focal ischemic lesions were detected in 23 to 43% of patients with filter-protected CAS. 26,27,29 The analysis of the location of the infarcts is equally important to their incidence. It appears that more than half of the infarcts involve either the contralateral hemisphere or posterior circulation, leading the authors of all of these studies to conclude that manipulation of endoluminal devices in the arch and supra-aortic vessels is the major risk factor for cerebral embolism during neuroprotected CAS. 27,29 Considering this, the authors of one of the studies suggested that direct puncture of the CCA could be a valuable technique and stated that the development of an adequate puncture-site closure device should be a priority. 27
Balloon occlusion neuroprotection has similar difficulties. Specifically, in a recent study, patients underwent CAS with either ICA balloon protection alone or simultaneous ICA and ECA balloon protection and were evaluated for distal embolism with diffusion-weighted MRI. 25 Ischemic regions were identified in 55% of those patients with ICA balloon protection and 36% of those with simultaneous ICA and ECA balloons. Similar to the findings associated with filter-protected CAS, approximately 40% of the new ischemic areas were in the ipsilateral hemisphere, whereas the rest were either in the contralateral hemisphere or in a posterior circulation distribution. In another study, TCD ultrasonography was used to assess the efficacy of distal balloon protection in preventing embolic neurologic events during CAS. 24 Balloon protection reduced by half but did not eliminate Doppler ultrasonography–detected microembolic signals during CAS. The authors speculated that factors contributing to microembolic signals with balloon protection are a nonocclusive distal balloon, possible embolization via the ECA, and trapped emboli within the “shadow zone” of the aspiration catheter that were inaccessible for removal. The findings from a recent study using TCD ultrasonography to compare the incidence of microembolic signals during the time of maximum expected neuroprotection (when the protection device was fully deployed and active) using filter, balloon, or flow reversal illustrate some of the fundamental differences between the three protection concepts. The data clearly demonstrate the absence of intracranial microembolic signals in patients with flow reversal. The balloon-protected patients experienced embolic signals during angioplasty (probably owing to ECA embolism) and at the time of balloon deflation, whereas the patients with filter protection had embolic signals throughout the entire time the filter was deployed. 8,20
Although 90% of MRI-identified ischemic lesions appear to be clinically silent with standard neurologic assessment, 18,37,40,41 it is well known that detection of any clinical aberration is dependent on the sensitivity of the method used for its evaluation. 42 Therefore, this high rate of microembolization raises questions about the possible short- and long-term consequences on cerebral cognitive functions. A recent large population-based study has shown that silent brain infarcts seen on diffusion-weighted MRI are associated with a steeper decline in cognitive function and may be associated with dementia. 43
Shortcomings of Flow Reversal
The patient's inability to tolerate flow reversal is the main shortcoming of the technique. That said, Criado and colleagues reported an intriguing study suggesting that reversal of flow may be better tolerated than balloon occlusion of the ICA and speculating that flow reversal enhances collateral flow to the circle of Willis. 3 Interestingly, the reported rate of intolerance to ICA flow reversal is 3 to 4%, 4,42 which is slightly better than the intolerance rate of 5 to 15% for ICA balloon occlusion. 40,44 The only two reported cases of neurologic intolerance at the time of transcervical CAS had contralateral ICA occlusion and an old contralateral stroke. 4 Unfortunately, no mention of intracranial collateral patterns was made. 4 In our experience, patients with at least one patent intracranial collateral (present in 90% of patients in need of ICA revascularization) tolerate ICA flow reversal without problems even if they have a contralateral ICA occlusion. 45 The patency of these collaterals (anterior communicating or ipsilateral posterior communicating artery) can be easily ascertained with CTA or MRA. We therefore recommend CTA for the preoperative workup of all CAS patients, which provides simultaneous evaluation of the anatomy, characteristics, and extent of occlusive disease in the cerebral circulation and patterns and adequacy of intracranial collaterals. For those few patients with inadequate collateral circulation, transcervical access can be attempted with intraoperative test ICA reversal. If the patient tolerates it well, then flow reversal is continued and CAS is performed; otherwise, transcervical CAS is completed with the use of a filter device for neuroprotection. 46
When Should Transcervical CAS with Flow Reversal for Neuroprotection Be Used?
The answer to this question is “It depends on the experience of the carotid operator.” Specifically, for those carotid operators with advanced expertise in transfemoral CCA cannulation, the transcervical approach should be reserved for patients with challenging anatomy or disease in the aorta, the iliac arteries, and the arch and its branches. However, for those operators less experienced with the challenges of transfemoral CCA catheterization and the remote management of its complications, the transcervical technique becomes the ideal approach because it bypasses all of the challenges of femoral access and allows for performance of potentially safer and consistently successful CAS while reducing the need for expensive neuroprotection devices.