
Abstract
Excision of atheromatous plaque is an attractive option for the minimally invasive treatment of peripheral arterial disease. Approved for use in 2003, the SilverHawk Plaque Exicison System (FoxHollow Technologies, Redwood City, CA) is a catheter-based plaque excision device allowing percutaneous removal of atheromatous material. This device represents the most recent generation of atherectomy tools. Overall experience with plaque debulking in the peripheral arteries spans almost two decades, and understanding of the technique continues to evolve. This article reviews the technology, current practices, and data on plaque excision.
Keywords
Despite 40 years of experience with percutaneous lower extremity revascularization, outcomes remain limited by restenosis and plagued by patency rates markedly below those of open lower extremity bypass procedures. 1 The majority of percutaneous lower extremity revascularization procedures involve the use of angioplasty. Inflation pressures range from 6 to 40 atmospheres of pressure. One of the potential inciting events for restenosis is theorized to be the barotrauma associated with angioplasty and exposure of subendothelial elements.
Atherectomy is the earliest term used to describe the procedure that removes atheromatous plaque to recreate or expand a lumen within a vessel. The more modern term of plaque debulking connotes the process of luminal expansion without associated barotrauma. Removal of atheromatous lesions has traditionally been accomplished via surgical endarterectomy. Certain vascular territories, such as the carotid artery, are amenable to endarterectomy owing to the presence of a well-defined end point of disease. However, in the infrainguinal vascular bed, this is often the exception. Atherosclerotic lesions in the lower extremity tend to be diffuse and ill-defined, even if a lesion appears to be focal on angiography. In addition, the most commonly affected segment of the superficial femoral artery at the adductor hiatus is relatively inaccessible surgically.
The escalation in the use of minimally invasive techniques for lower extremity revascularization is a response to the risks, complications, and imperfect patencies of open surgical bypass. In studies of pedal artery bypasses, primary patency rates were established at 67% at 1 year and 38% at 10 years. 2,3 More proximal targets have higher degrees of patency. Bypass with saphenous vein from the common femoral to the above-knee popliteal segment has a patency rate as high as 76% at 5 years. 4,5
When an intact autogenous saphenous vein is not available, patency suffers dramatically. Saphenous vein grafts perform better than all other conduits, with a secondary patency rate of 68% compared with 46% for all other conduits used in pedal bypasses. 3 In a study of 240 infrainguinal bypasses with cryopreserved vein, the primary patency rate was 30% at 12 months and dropped to 18% at 2 years. 6 A meta-analysis of studies evaluating the durability of alternate venous conduits demonstrated a primary patency rate of 47% at 5 years. 7 A prospective randomized study of polytetrafluoroethylene or saphenous vein to the above-knee popliteal artery had patency rates of 76% and 52%, respectively. 5
The morbidity and mortality associated with bypass procedures cannot be overlooked in a risk-benefit analysis. Although most studies conclude that the mortality rate following infrainguinal bypasses is low, there is an inherent bias in that some patients are deemed to be too high risk to even be considered for bypass procedures. Of those patients who undergo bypass, the 30-day perioperative mortality rate ranges from none to 1% and as high as 5.2%. 2,3,5,8,9 In addition to mortality, significant morbidity is associated with bypasses, including lower extremity edema, wound complications, and lymphatic complications.
Despite a successful bypass, the goal of relief of ischemic pain, healing of tissues, or even a return to a patient's premorbid state is not always met. In a study evaluating the ability of patients to return to their baseline status after bypass, many patients required reoperation within 3 months. Half of the population studied required readmission to the hospital within 6 months. The mean time to heal the wounds that prompted the bypass was greater than 3 months in over half of the patients evaluated. 10 Revision of bypasses is not uncommon to maintain primary patency. Despite what are largely thought to be benign procedures, revision has proven to have an independent set of perioperative risks, proportional to the degree of revision required. 11
Catheter-Based Infrainguinal Arterial Interventions
Minimally invasive methods seek to approximate the durability of bypasses while reducing the risks to the patient. In comparison with surgical bypass, angioplasty is associated with a 30-day periprocedural mortality under 3%. 9,12 However, as is the bias with open bypass, many patients are selected to undergo minimally invasive methods owing to the presence of comorbidities, which obviate the safe performance of a bypass. One of the main barriers to the wide adoption of minimally invasive methods is the disparity of patencies when compared with open bypass. The most commonly performed method of percutaneous revascularization is percutaneous transluminal angioplasty (PTA). Initial series of PTA in the infrainguinal circulation established a patency rate of 30 to 50% over a 5-year follow-up. 13–15 Patency was found to depend on lesion site (proximal or distal segments), lesion type (stenosis or occlusion), and runoff. 16 More recent evaluations have failed to illustrate improvements in patency despite improvements in technology and pharmacotherapy. However, in a recent study of 180 patients, the cumulative primary patency rate (at the 2-year follow-up) was 75% for femoropopliteal angioplasty and 60% for infrapopliteal angioplasty. The rate of restenosis (more than 50% lumen loss at 2 years after the intervention) was also significant (65%). 9 Patency was not found to be significantly affected by the selective use of stents, with a documented primary patency rate of 49% in the femoropopliteal segment and 24% in the infrageniculate arteries. 17,18 A recent prospective study evaluating isolated PTA against mandatory stent placement in the femoropopliteal segment revealed a 12-month patency rate of PTA alone of 37% and 63% after nitinol stent placement. 19 There are studies demonstrating better patency rates (ie, 55% at 5 years), but these remain the minority. 20
Lower Extremity Arterial Plaque Excision
Given the poor patency associated with angioplasty compared with bypass, despite the reduction in morbidity, additional technologies have been pursued. The concept of percutaneous plaque excision is not novel. The Simpson atherectomy (Guidant Corp, Indianapolis, IN) catheter was introduced into peripheral use in 1987. 21 This dual-lumen catheter featured a high-pressure balloon that served to push its cutting blade against the arterial wall. Several clinical studies of the Simpson atherectomy catheter were carried out. Most of these were small series from single institutions with relatively small numbers of lesions treated. 22–25 Despite the high-pressure centering balloon of these devices and the associated potential for barotrauma, the published reports were positive. In one study of 10 patients with 12 lesions, 40% of patients had objective evidence of postprocedural hemodynamic improvement (the remaining 60% were not evaluated). All of the patients evaluated were either symptomatically improved or had salvaged limbs over the interval they were studied (6–14 months). 23 A larger study of 77 patients with 85 treated lesions showed that the probability of 1-, 2-, and 3-year patency for atherectomy was 92%, 84%, and 84% (68 lesions available for follow-up; mean 13.5 months). 22
The mechanism of plaque excision as opposed to alternate methods of luminal expansion by the Simpson atherectomy catheter was investigated in 1995 by analysis of quantitative angiography, endovascular ultrasonography, and angioscopy in the coronary circulation. 26 This study concluded that the lumen achieved by plaque debulking was not as regular by angioscopy and endovascular ultrasonography compared with evaluation by angiography. Luminal enlargement was due to excision of plaque and not other modes of arterial expansion. Other investigations as to the mechanism of the efficacy of atherectomy include a study of 218 peripheral arterial stenoses resected from 100 patients by atherectomy. 27 Primary stenoses were composed of atherosclerotic plaque (150 lesions), fibrous intimal thickening (15 lesions), or thrombus alone (5 lesions). Atherosclerotic plaques had a variable morphology and, in one-third of cases, were accompanied by abundant surface thrombus, which probably added to the severity of stenosis. Pathologic examination of tissues recovered by peripheral atherectomy is an important adjunct that may provide insight into the efficacy of vascular interventions and the phenomenon of postintervention restenosis. Other authors have also used the material retrieved from atherectomy for histologic analysis with the same hypothesis that lesion analysis can provide insight into the underlying disease process. 28 Additional studies in the coronary circulation suggest that optimal stent implantation is more easily achieved after plaque excision compared with angioplasty. 29
Additional devices, such as the Bard Rotary Atherectomy System (BRAS) (CR Bard, Murray Hill, NJ), the rotoblator Boston Scientific, Natick, MA) and the Xtrak device (Xtrak Medical Inc, Salem, NH), have also been evaluated in the periphery, have shown poor results, have been met with limited clinical enthusiasm, and have no significant current clinical use. 30–32
Silverhawk Plaque Excision System
In 2003, the US Food and Drug Administration approved the SilverHawk Plaque Excision System (FoxHollow Technologies, Redwood City, CA). The system consists of a catheter with a mounted blade and collection area and a handheld battery-powered drive unit. The SilverHawk device is made up of a 135 cm shaft with a cutting assembly, which consists of a cutting blade at the proximal end of a nosecone designed to collect the plaque shavings (Figure 1). The blade is activated by a switch on the handle or battery pack. The shaft is flexible throughout its length, except at the distal end near the cutting assembly, where it has a slight double-curve such that the blade, when exposed and engaged, sits at the apex of the curve and engages the luminal surface (Figure 2). The collecting nosecone on the larger catheters has a packing mechanism that compresses the shavings into the cone for increased carrying capacity. The nosecone is emptied by either forceful saline flushing or mechanical evacuation using specially designed instruments.

Close-up view of the cutting blade of the SilverHawk plaque excision catheter system.
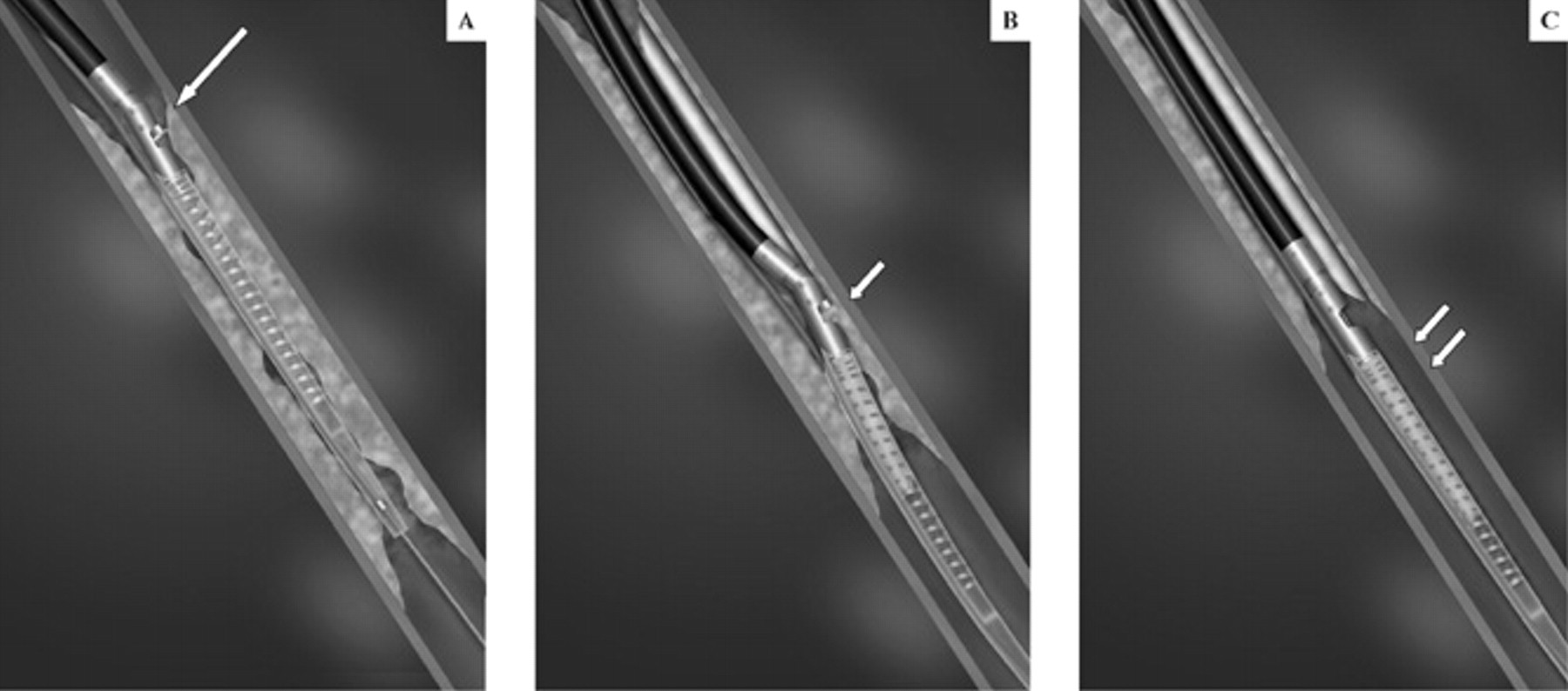
A, Activation of the SilverHawk catheter enables the cutter blade (long arrow) to appose the vessel wall plaques. B, By slowly advancing the SilverHawk atherectomy catheter in a forward fashion, the rotating cutting blade excises the luminal plaques (small arrow) and stores them in the distal nosecone chamber. C, Plaques are excised (double arrows) by rotating the catheter in various directions, which allows circumferential debulking of the luminal lesions.
The catheter comes in several sizes to treat vessels of differing diameters (Table 1). The catheters are introduced via vascular sheaths that vary with device size from French sizes 6 through 8. This contrasts with the older-generation devices, which required up to an 11F delivery sheath. They are monorail catheters meant for rapid exchange and operate over a 0.014-inch diameter wire system. In addition to the smaller size, the most notable difference from the older-generation devices is the lack of the centering balloon. The other changes since the initial device are the material of the cutting blade (steel to carbide), the speed of the device (2,500 – 8,000 revolutions per minute), and the device delivery (from over-the-wire to rapid exchange monorail).
Available SilverHawk Catheter Systems and Device Descriptions
Clinical Results of the Silverhawk Catheter
Experience with the current device has been extensively documented in meeting presentations and in the Fox Hollow Corporation's TALON registry. The TALON (Treating PeripherAls with SiLverHawk: Outcomes CollectioN) registry is an observational, consecutive, nonrandomized, multicenter registry. This registry has enrolled more than 800 patients with over 600 infrainguinal arterial lesions that have been treated with the Silverhawk device. Data from this registry have been analyzed by several groups. Twelve-month freedom for target lesion revascularization (TLR) has been reported out of this registry at 87% (n = 169 lesions) for femoropopliteal lesions treated for claudication (corporate data). A more recent analysis of this registry including patients with infrapopliteal arterial occlusive disease was reported. 33 From the registry data, 212 patients were diagnosed with 391 lesions in 264 limbs in the infrapopliteal region. All patients were treated with the SilverHawk atherectomy device. The lesion localization was the tibioperoneal trunk, 27%; peroneal artery, 21.5%; posterior tibial artery, 19.6%; anterior tibial artery, 28.7%; dorsalis pedis artery, 2.5%; and calcaneal artery, 0.6%. The mean lesion length was 36 mm. The preprocedure mean diameter stenosis was 91.1%, and post–plaque excision alone, the residual diameter stenosis was 8.3%. Postprocedure follow-up hemodynamic measurements were available for 34% of the patients, revealing an average ankle brachial index of 0.86. Freedom from reintervention was 84% at 6 months and 77% at 12 months. The procedure-related complication rate was low, which included perforation (1.9%) and dissection (1.9%). The limb loss rate at 1 year was 9.8%. The below-the-ankle amputation rate was 4% at 1 year. 33 Based on the findings of this study, the authors concluded that the SilverHawk is an effective treatment modality in patients with infrapopliteal arterial occlusive disease, with favorable freedom from reintervention at 1 year.
In a peer-reviewed analysis of plaque excision in patients with tissue loss, the SilverHawk was used in 69 patients (76 limbs, 159 lesions) and clinical outcomes were prospectively assessed for 6 months at 7 institutions. Plaque excision was found to be a safe and effective method for percutaneous revascularization. 34 Procedural success was achieved in 99% of patients enrolled in the study, and major adverse events occurred in 1% of patients at 30 days and 23% at 6 months. The authors reported a low TLR rate of 4%, with no unplanned limb amputations. 34 Evidence of successful revascularization after therapy with the SilverHawk device has been presented at various meetings documenting an average improvement in ankle brachial indices from 0.38 preoperatively to 0.76 immediately following intervention (p < .01). 35
Angioplasty of arteries at flexion areas such as the common femoral and the popliteal artery is plagued by the potential of requiring adjunctive stenting to treat a dissection. Owing to the risk of stent fracture or arterial rupture by repetitive motion, stenting is traditionally avoided in these areas. 36 Plaque debulking has the ability to treat lesions in these areas without this added risk. 23,37,38
Other technologies seeking to address the relatively poor patency of PTA of the infrainguinal circulation include cryoplasty. In the femoropopliteal circulation, cryoplasty is associated with a clinical patency rate of 82.2% at the 9-month follow-up, but the patency rate as determined by color duplex ultrasonography was 70%. 39 In a small series of 15 patients, angiographic follow-up at 14 months exhibited a primary patency rate of 83%. 40 Remote endarterectomy is also an option for plaque debulking through a small arterial access incision with adjunctive stenting to seal the end point. 41 Although minimally invasive, this does require at least one incision and, in some instances, the use of interposition grafting as an adjunct. In another analysis with follow-up of 19 months, the primary patency rate of this procedure by life table analysis was 70% at 30 months and limb salvage was 94%. 42 A separate study documented the primary cumulative patency rate by life table analysis of 68.6 ± 13.5% (standard error) at 18 months. 43
Conclusions
Based on the available literature, there are some arguments for plaque debulking in the periphery. The data available support the contention that the current device can be safely used and is effective. Early data support excellent patency rates and the ability to use the SilverHawk plaque debulking system in multiple clinical settings. The device has been safely and effectively used in stenoses, chronic total occlusions, restenotic lesions, and lesions in which PTA and stenting are typically avoided. The larger question of long-term durability and superiority or inferiority to other technologies is still under investigation. Despite this, the safe use of the SilverHawk is one component of the endovascular specialists' armamentarium.