
Abstract
Endothelial progenitor cells (EPCs) are the key cellular effectors of postnatal vasculogenesis and play a central role in wound healing. In diabetes, there is a significant impairment in the number and function of circulating and wound-tissue EPC. Recent evidence indicates, that tissue-level hyperoxia achieved by therapeutic hyperbaric oxygen protocols (HBO2) can increase the mobilization of EPC from the bone marrow into peripheral blood. In this paper we review the recent reports on hyperoxia-mediated mobilization of bone marrow-derived EPC and postulate avenues of future research in this area as it applies to improving healing in chronic wounds affected by diabetes and peripheral arterial disease (PAD).
Diabetes mellitus refers to a range of conditions characterized by an elevation of the blood glucose level, and the disorder is divided into two principal varieties. Type 1 accounts for less than 10% of all diabetics and is due to an autoimmune attack on the pancreatic β-cells that results in their destruction. Type 2 diabetics exhibit impairments of both insulin secretion and insulin action. Type 2 diabetes is reaching epidemic proportions in Western societies and is predicted to affect 300 million people worldwide by 2025. 1 Nearly 800,000 new cases of diabetes mellitus are diagnosed per year in the United States, and approximately 15% of patients will develop a lower extremity ulcer at some point in their lives. 2–5 It has been estimated that up to 2 million Americans suffer from nonhealing lower extremity wounds, accounting for 162,500 annual hospitalizations and 1 billion dollars per year in health care costs in the United States. 1,5–11
Wound healing occurs because of events in two compartments. Within the bone marrow, various signaling pathways lead to mobilization of bone marrow–derived endothelial progenitor cells (EPCs) and other stem progenitor cells involved in the healing cascade. Within the wound, neovascularization occurs because of local factors that stimulate adjacent cells (angiogenesis) and because of recruited circulating EPCs that differentiate into vascular channels (vasculogenesis). In diabetic patients and diabetic murine models, the number and function of circulating EPCs are severely impaired, and this defect is highly correlated with the long-term cardiovascular and wound healing complications. 12–15 Increasing evidence suggests that wound healing processes in both the bone marrow and within the peripheral wound are compromised by diabetes as a result of EPC impairments, and both can be improved by wound management practices that influence EPC mobilization, homing to wounds, and other intrinsic wound characteristics.
Hyperbaric oxygen therapy (HBO2) is an adjunctive therapy used to stimulate wound healing in situations in which the microvasculature has become attenuated. Patients typically receive 20 or more treatments breathing 100% O2 in a pressurized chamber at 2.0 to 2.8 atmospheres absolute (ATA), once or twice daily. Although successful as an adjunct therapy in some clinical situations, HBO2 is not uniformly effective. 16–20 Moreover, the clinical protocols in current use were arbitrarily determined because the fundamental mechanisms are unclear. Thus, active research continues to explore the mechanisms for HBO2therapeutic efficacy in diabetic wound healing as an avenue to potentially expand its use in other types of delayed healing or vascular pathologies and in the hope of one day increasing its effectiveness by synergistic pharmacologic intervention.
Etiology of Chronic Diabetic Wounds
The pathophysiology of diabetic lower extremity ulcerations and delayed healing has been well described. Contributing factors include progressive development of a sensory, vasomotor, and autonomic neuropathy leading to loss of protective sensation; deformity that increases plantar foot pressure; and alterations in autoregulation of dermal blood flow. Most significantly, diabetics show earlier development and progression of lower extremity peripheral arterial occlusive disease with a predilection for the trifurcation level of vessels just distal to the knee. In addition, the tissue microcirculation is severely diseased (microangiopathy), even in patients with patent proximal vessels. Impaired host response to infection and other cellular dysfunctions also contribute to the refractory nature of wound healing.
Approximately 20% of diabetic lower extremity ulcers have arterial flow insufficiency as their primary etiology, approximately 50% will have primary diabetic neuropathy, and approximately 30% will have both conditions. 3,4 Even after correction of large blood vessel dysfunction (revascularization), only about 47% of patients will heal in a span of 20 weeks with standardized treatment, including glycemic control, débridement of necrotic tissue, control of infection, use of moist dressings, and protection from pressure or trauma related to ambulation. 21 The probability of healing decreases progressively among patients whose wounds are older than 2 months or larger than 2 cm 2 or who have a full–skin thickness ulcer with exposed tendons or deeper tissues. 9 Beyond standard treatment practices, the topical application of becaplermin (platelet-derived growth factor BB) and platelet releasate have been shown to increase healing. 22–24 Bioengineered human skin or dermis equivalents have also shown benefits. 25 These therapeutic modalities have received approval from the US Food and Drug Administration only to treat wounds that do not extend to fascia, muscle, or bone in individuals with adequate arterial flow. The effectiveness of HBO2 as an adjuvant therapy for the treatment of lower extremity ulcerations in diabetics has been supported in six randomized trials and evaluations by a growing number of independent, evidence-based reviews. 16–20,26–34 Although, in general, “an angiogenesis effect” has been implicated, there is only a paucity of information on its basic mechanisms of action.
Vasculogenesis and Angiogenesis in Wound Healing
Normal wound healing proceeds through an orderly sequence of steps, involving removal of necrotic debris and infection, resolution of inflammation, repair of the connective tissue matrix, angiogenesis, and resurfacing. Problem or chronic wounds are those that have failed to follow this sequence and do not achieve a sustained anatomic and functional result. 6 The hypoxic nature of all acute wounds has been demonstrated, but when hypoxia is pathologically increased, wound healing is impaired and the rate of wound infection increases. 9,21–23,35,36 Local oxygen tensions in the vicinity of the wound are approximately half the values observed in normal, nonwounded tissue. 36 Fibroblast recruitment, collagen deposition, angiogenesis, and intracellular leukocyte bacterial killing are oxygen-sensitive responses involved with normal wound healing. 37,38 It is now well established that an essential part of normal healing is the formation of new vessels within the provisional wound matrix that is referred to as granulation tissue formation. Neovascularization of wound granulation tissue occurs by the processes of angiogenesis and/or vasculogenesis. 39 Angiogenesis refers to the process by which resident endothelial cells of the wound's adjacent mature vascular network proliferate, migrate, and remodel into neovessels that grow into the initially avascular wound tissue aided by mature stromal cells, such as fibroblasts. Vasculogenesis is a de novo process by which EPCs recruited to the wound differentiate into endothelial cells and give rise to a replacement vascular network. 39–41 We have identified a critical role for EPCs in ischemic wound healing. 42
It was once believed that vasculogenesis occurred only during embryonic life; however, EPCs have been identified in peripheral blood in adults and increased with traumatic or surgical wounds. 43 EPC mobilization can be stimulated by peripheral ischemia, vigorous exercise, chemotherapeutic agents, and hematopoietic growth factors. 44–50 EPCs also can be obtained by direct bone marrow harvesting and ex vivo manipulations. 51 Hematopoietic progenitor cells are typically obtained for the purpose of bone marrow transplantation by administration of chemotherapeutic agents and growth factors. 52 Using these agents to obtain EPCs for purposes such as wound healing or therapeutic neovascularization has been considered, but generalized application is thwarted owing to risks such as acute arterial thrombosis, angina, sepsis, and death. 52–54 Nevertheless, some experimental data suggest that parenteral administration of granulocyte colony-stimulating factor can reduce the rate of amputation and other surgical procedures in patients with diabetic foot infections. 55 EPCs given to animals can be incorporated into the foci of neovascularization in surgically induced ischemic organs and limbs. 44,46,56 Transplantation of autologous bone marrow cells and purified EPCs into ischemic areas, including the wounds of diabetic animals, has been shown to improve perfusion and accelerate healing. 47,51,56–58
Therapeutic Mechanisms for Tissue Hyperoxia Induced by HBO2
If periwound tissue is normally perfused, a steep oxygen gradient from the periphery to the hypoxic wound center supports a normal wound healing response. 35,59 Eradicating this gradient will arrest capillary growth. Data pertaining to radiation necrosis suggest that in the setting of microangiopathy, the O2 gradient across a wound is inappropriately flat. 60 HBO2 will raise arterial O2 tension to several thousand Torr and tissue tension to ≅300 Torr. 61 It has been hypothesized that HBO2 creates a steep gradient, and this increases migration of macrophages into the center of the wound and release of angiogenic growth factors. 60 This mechanism remains unproven, however, and some data argue that the O2 gradient per se is not necessarily an element of refractory wounds. 62
Production of superoxide radical (O2
.) is increased in many organs by hyperoxia.
34
In recent years, we have also found that HBO2 increases nitric oxide (
HBO2 increases synthesis of several growth factors that could stimulate angiogenesis and production of granulation tissue. Vascular endothelial growth factor (VEGF)-A is the most specific growth factor for neovascularization, and it is increased in experimental wounds by HBO2.
67–70
HBO2 will also stimulate synthesis of basic fibroblast growth factor and transforming growth factor β1 by human dermal fibroblasts and angiopoietin 2 by human umbilical vein endothelial cells, and it up-regulates platelet-derived growth factor receptor in experimental wounds.
19,67–70
Whereas hypoxia-inducible factor 1 (HIF-1) is the major mediator of VEGF transcription under hypoxic conditions, VEGF synthesis by macrophages is also stimulated by oxidants and by
The bone marrow is the major reservoir for adult organ-specific stem cells, including hematopoietic stem cells and endothelial progenitors.
44–46,76
Many chemokines or cytokines trigger EPC release via induction of metalloproteinase 9 (MMP-9) in bone marrow, and
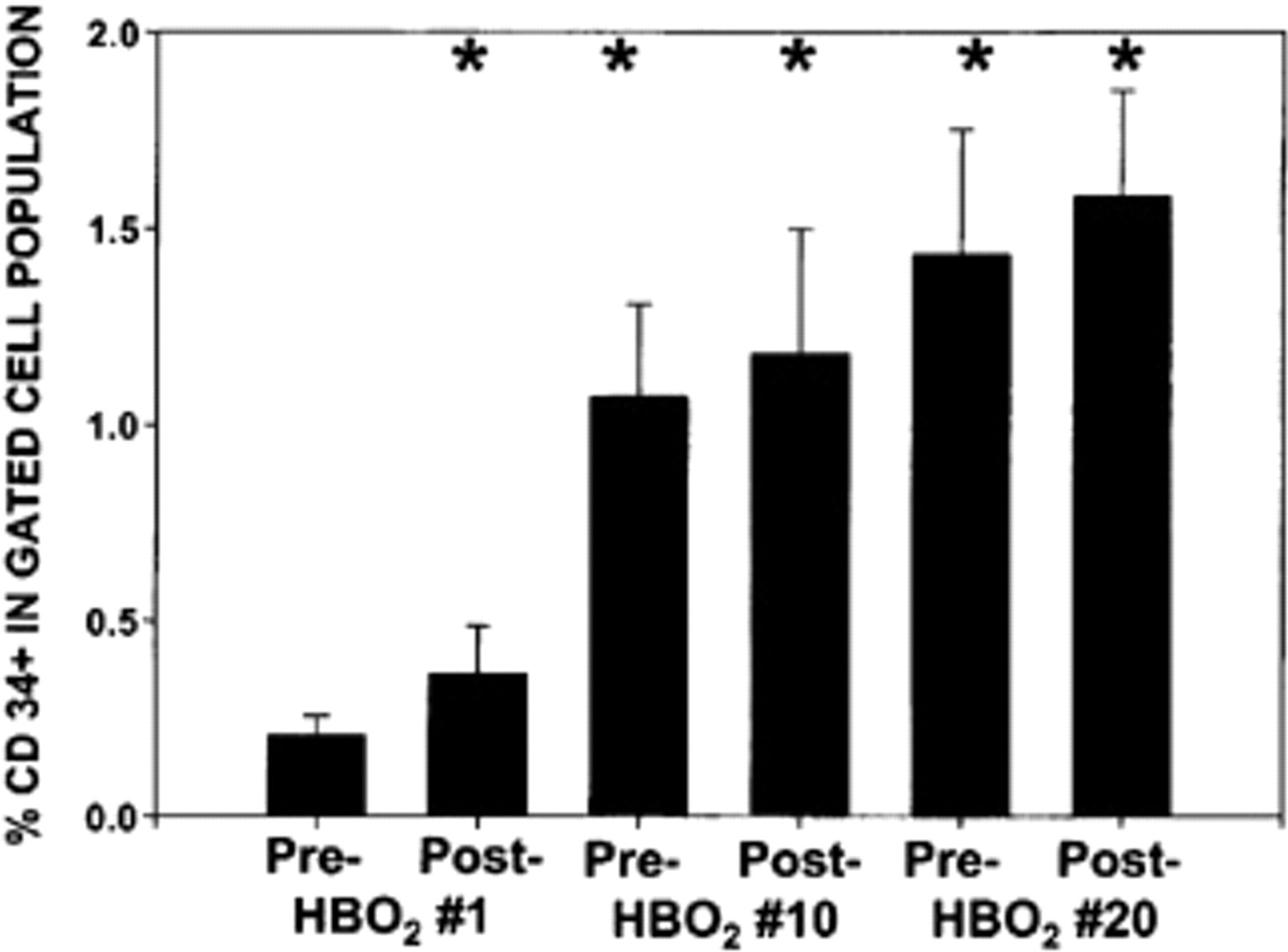
Mean CD34+ population in the blood of humans before and after hyperbaric oxygen (HBO2) treatments. Data are the fraction of CD34+ cells within the gated population using leukocytes obtained from 26 patients before and after their first, tenth, and twentieth HBO2 treatment. *Repeated measures one-way analysis of variance, p < .05 versus the pre-HBO2 first treatment value.
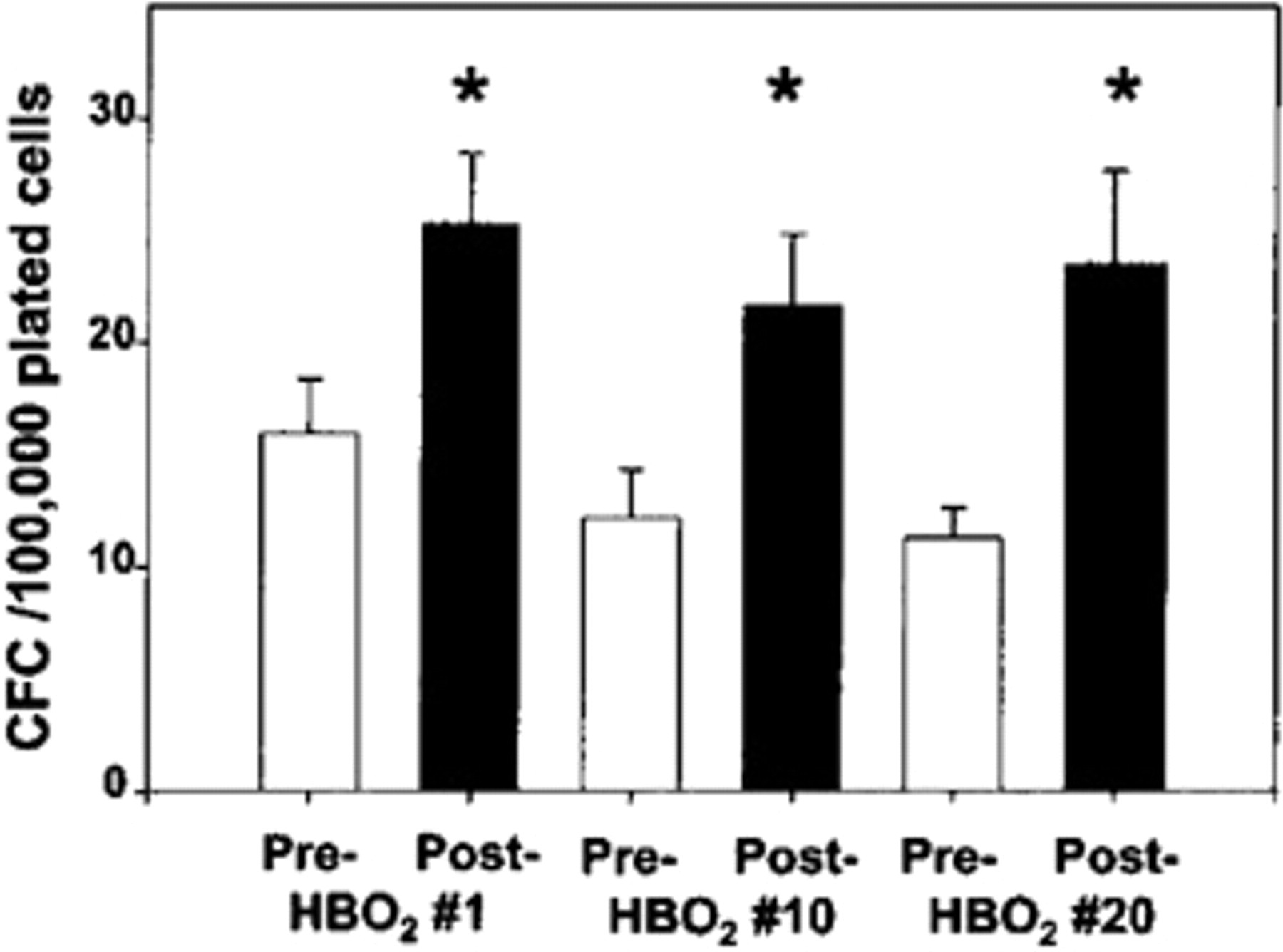
Colony-forming cells (CFC) in the blood of humans before and after hyperbaric oxygen (HBO2) treatments. Data are the colonies counted after a 14-day incubation. *t-test performed on each data set before and after the first treatment, p = .036; before and after the tenth treatment, p = .041; and before and after the twentieth treatment, p = .049.
HBO2 Increases Circulating EPCs In Humans
In initial human studies on the mobilization of EPCs by HBO2, blood was obtained from 26 patients before and after their first, tenth, and twentieth HBO2 treatments for osteoradionecrosis prophylaxis (the standard preoperative course of therapy is 20 treatments). Blood leukocytes were harvested and analyzed for the presence of EPCs based on flow cytometry and colony-forming cells (CFCs). Control human subjects included patients breathing 100% O2 but not pressurized and pressurized attendants not breathing 100% O2 in whom tissue-level hyperoxia is not achieved. 66 In HBO2-treated patients (but not controls), the CD34+ population in blood (see Figure 1) and the number of CFCs in peripheral blood were significantly increased in response to each exposure to HBO2 (see Figure 2). 66 Of note, we did not find elevations in CFCs prior to the tenth and twentieth treatments (see Figure 2), although the numbers of CD34+ cells were elevated (see Figure 1). This suggested that only cells recently mobilized by HBO2 exhibit an increased propensity to grow and form colonies, a subject that is currently being actively investigated in our laboratory.
To specifically address whether the increased CFCs were coming from the fraction of cells expressing CD34, the circulating monocyte population of nine patients before and after their twentieth HBO2 treatment was isolated and fractionated using paramagnetic polystyrene beads coated with antibody to CD34. In the CD34+ fraction, prior to treatment, there were 13 ± 0.3 colonies, and after HBO2treatment, 23 ± 3 colonies grew (p < .05), whereas in the CD34− fraction, 12 ± 0.7 colonies grew prior to treatment and 13 ± 0.6 (not significant) grew after HBO2treatment. 66 These data indicate that the CD34+cell fraction (that contains the EPC pool) was the one that exhibited improved growth potential in response to hyperoxia. We were also interested in characterizing these cell-surface antigenic phenotypes of the cell colonies. Colonies were harvested, washed, and stained with antibodies. Figure 3 shows a typical flow cytometry scatter plot demonstrating that a large number of these cells express chemokine receptor 4 (CXCR4) and vascular endothelial growth factor receptor-2 (VEGFR-2), which are highly specific markers for EPCs. 71 As CXCR4 is required for EPCs homing to sites of injury or ischemia, 71 and both CXCR4 and VEGFR-2 are coexpressed on EPCs, 75 our findings suggest that the cells mobilized by HBO2 are EPCs and may be functional in improving neovascularization.
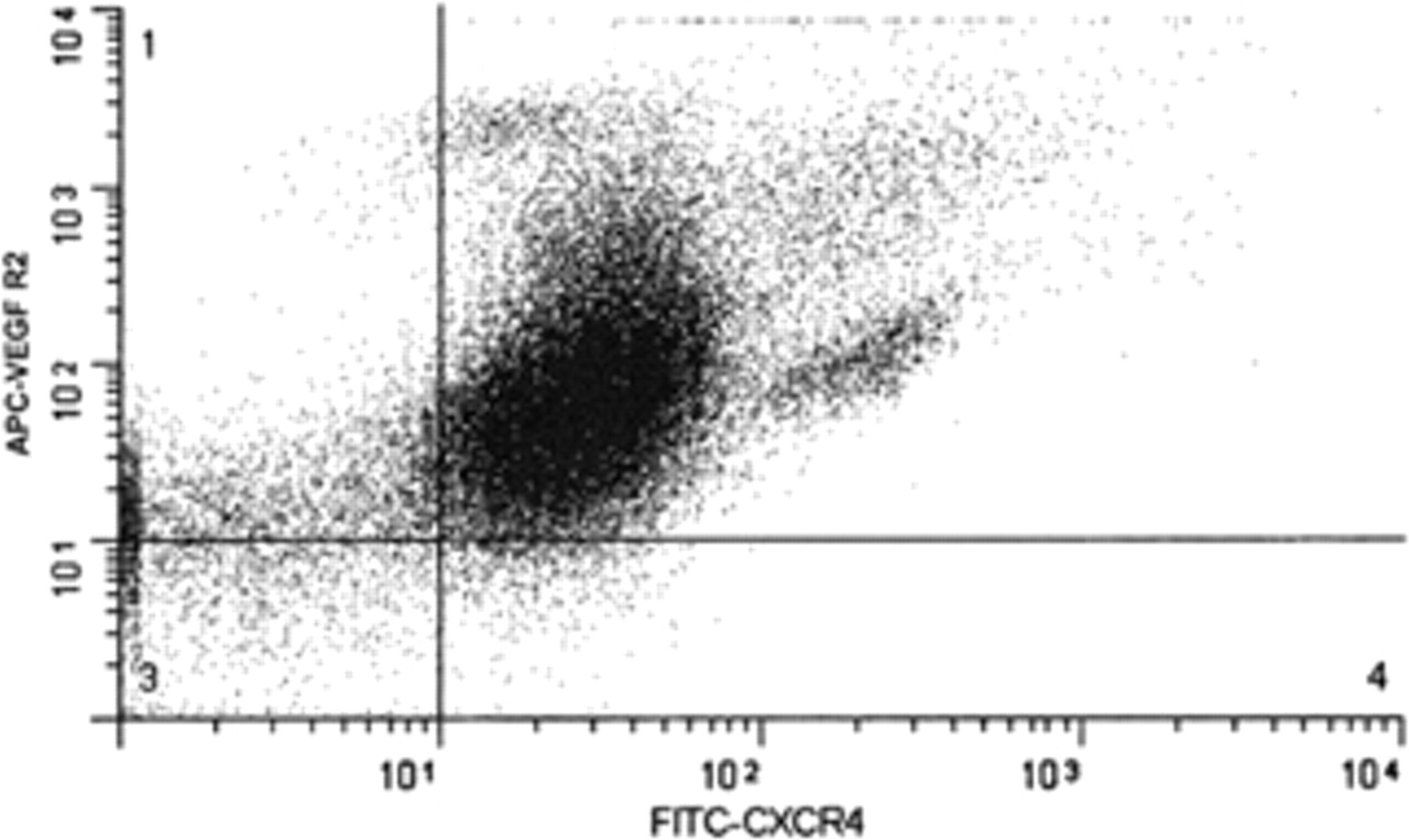
Expression of surface markers on the progeny of mobilized CD34+ cells. The figure shows the results from 50,000 cells. APC = allophycocyanin; CXCR4 = chemokine receptor 4; FITC = fluorescein isothiocyante; VEGF R2 = vascular endothelial growth factor receptor 2.
HBO2 Increases Circulating EPCs in Mice via NOS
In our initial studies searching for the mechanisms for EPC mobilization with HBO2,we also evaluated EPCs (assessed as cells that coexpressed CD34 and stem cell antigen 1) in the peripheral blood of mice. We subsequently demonstrated (with a number of specific EPC markers in both diabetic and nondiabetic mice models) that HBO2 induces EPC release via a
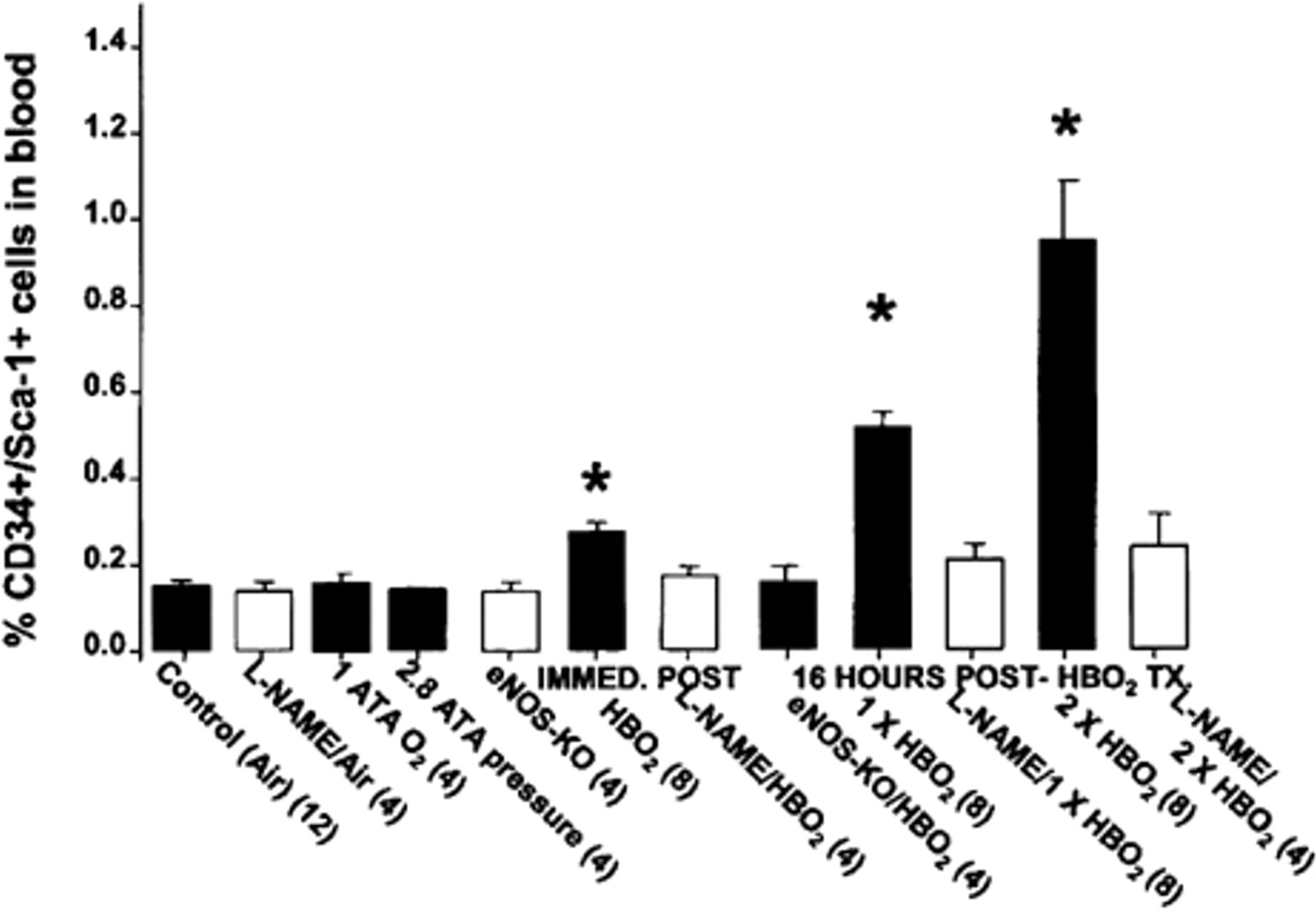
Mean CD34+/stem cell antigen 1 (Sca-1)+ cells in blood from mice undergoing hyperbaric oxygen (HBO2) treatment (Tx). From left to right, the bars show the control conditions (air;
There is a precedence for rapid mobilization of stem cells from bone marrow, but most emigration is believed to occur after a period of cell proliferation within the marrow niche. 48,49 We found that the number of EPCs peaked at 16 hours after mice were exposed to 2.8 ATA 100% O2, and if mice were exposed to 2.8 ATA 100% O2 for 90 minutes on 2 successive days, the number increased even more (see Figure 4). There was no additional increase in peripheral blood EPCs if mice were exposed to more than two HBO2 treatments. The leukocyte count in peripheral blood and bone marrow did not increase in response to HBO2 (Table 1), but there was a significant elevation in CFCs in both blood and bone marrow, indicating the activation of these cells to grow as colonies with the hyperoxia stimulus.
Effects of Hyperbaric Oxygen (HBO2) Treatment on Bone Marrow and Blood Parameters
ATA = atmospheres absolute; CFC = colony-forming cell;
Data from mice show mean ± standard error for studies conducted with air-breathing mice (control) and mice killed 16 hours after one hyperbaric oxygen treatment (six mice in each group).
*t-test, p = .019 for blood CFC data; p = .001 for marrow CFC data; p = .020 for plasma SCF data. Mouse SCF was measured using the Quantikine M immunoassay kit from R & D Systems (Minneapolis, MN), following the manufacturer's instructions.
EPC mobilization did not occur in mice lacking genes for eNOS (see Figure 4). If wild-type mice were injected before HBO2 with the nonspecific NOS inhibitor
HBO2 Increases .NO Concentration in Bone Marrow
In early studies, we hypothesized that HBO2 augments stem cell mobilization because it stimulates
Mice were placed in a hyperbaric chamber where, while breathing air, baseline measurements were obtained. The chamber was then flushed with 100% O2 and compressed to 2.4 ATA O2. The results (Figure 5) demonstrated a pronounced elevation of
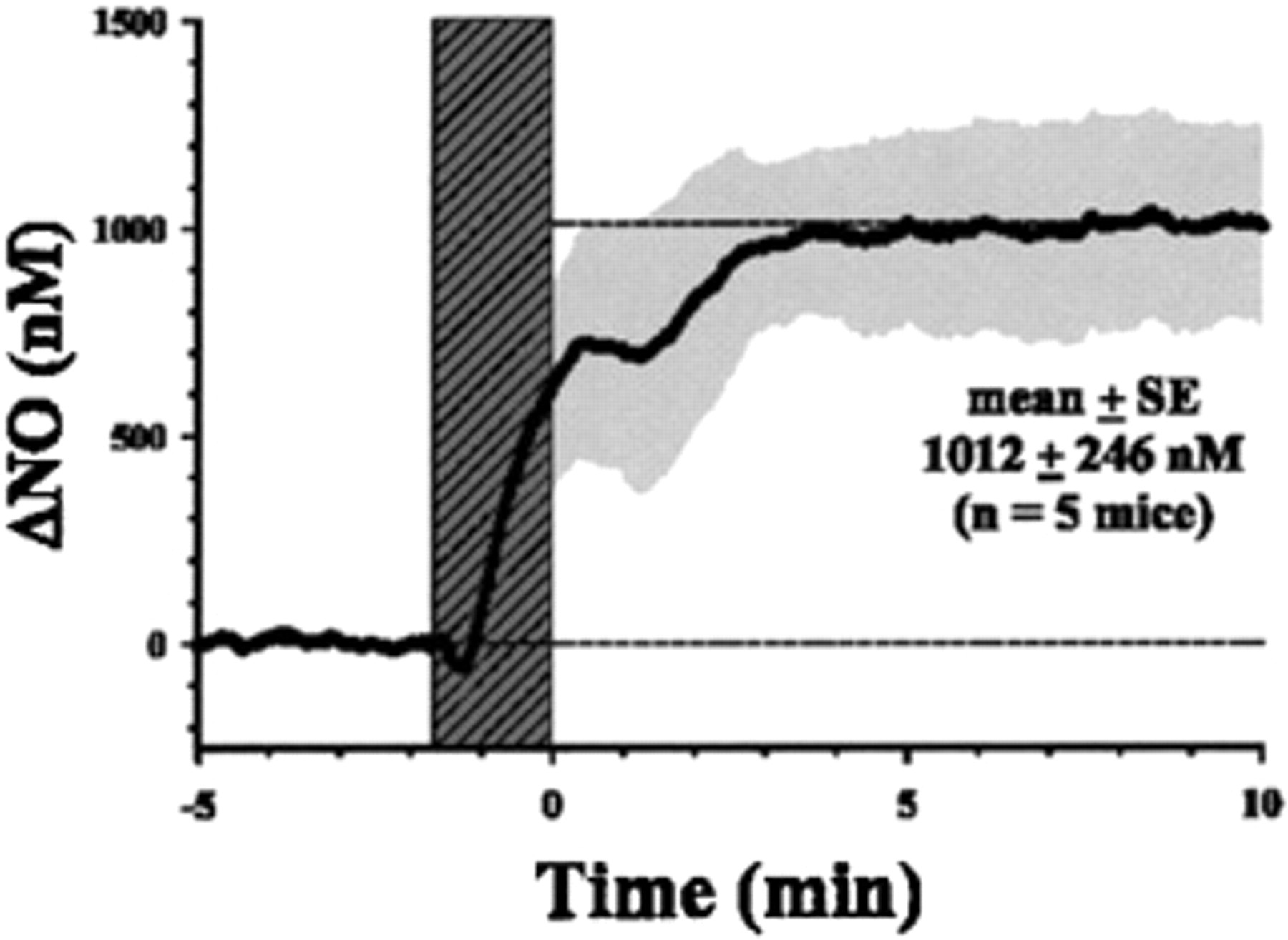
Hyperbaric oxygen stimulates nitric oxide (.NO) synthesis in mouse bone marrow. Data show mean and standard error (SE), depicted by the gray shading; dark vertical (hatched) shading shows the time required to pressurize the mice to 2.4 ATA after flushing the chamber with 100% O2.
In addition, we observed that HBO2daily treatments (2.4 ATA 100% O2 for 90 minutes) improved hindlimb perfusion by laser Doppler imaging after femoral ligation or excision (Figure 6) and increased the bone marrow–derived EPCs within the incisional wounds 3 days postwounding (with four HBO2treatments) (Figure 7). By day 8 after wounding, ischemic excisional punch biopsy wounds treated daily with HBO2healed faster (Figure 8). These wound healing improvements were not observed in mice that received intraperitoneal treatment with
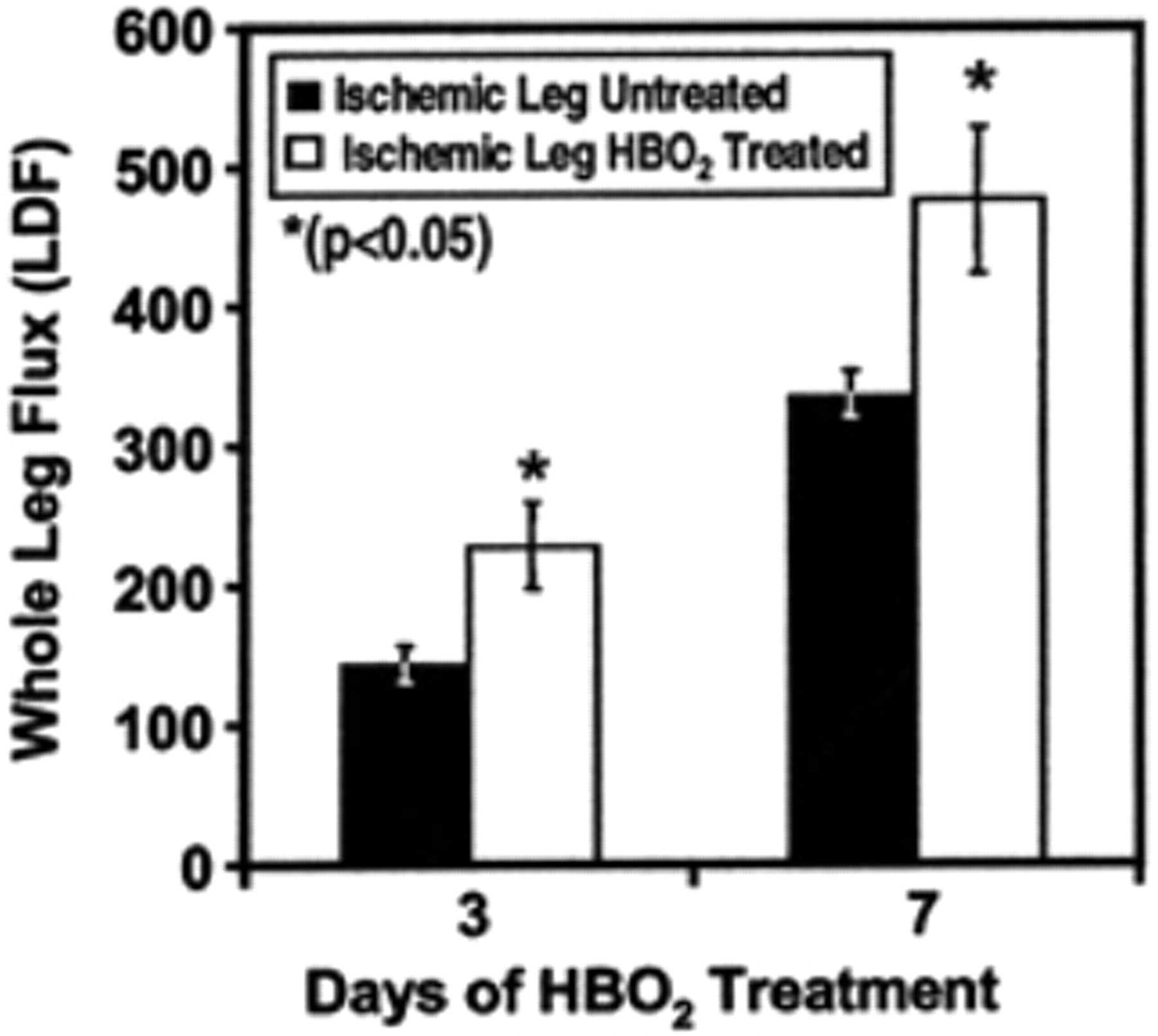
Ischemic hindlimb blood flow by laser Doppler flux (LDF) is significantly improved in friend virus B (FVB) mice by daily hyperbaric oxygen (HBO2) treatment. Mice underwent femoral ligation, and LDF was measured at days 3 and 7 of HBO2 treatment (n = 7 mice per group).
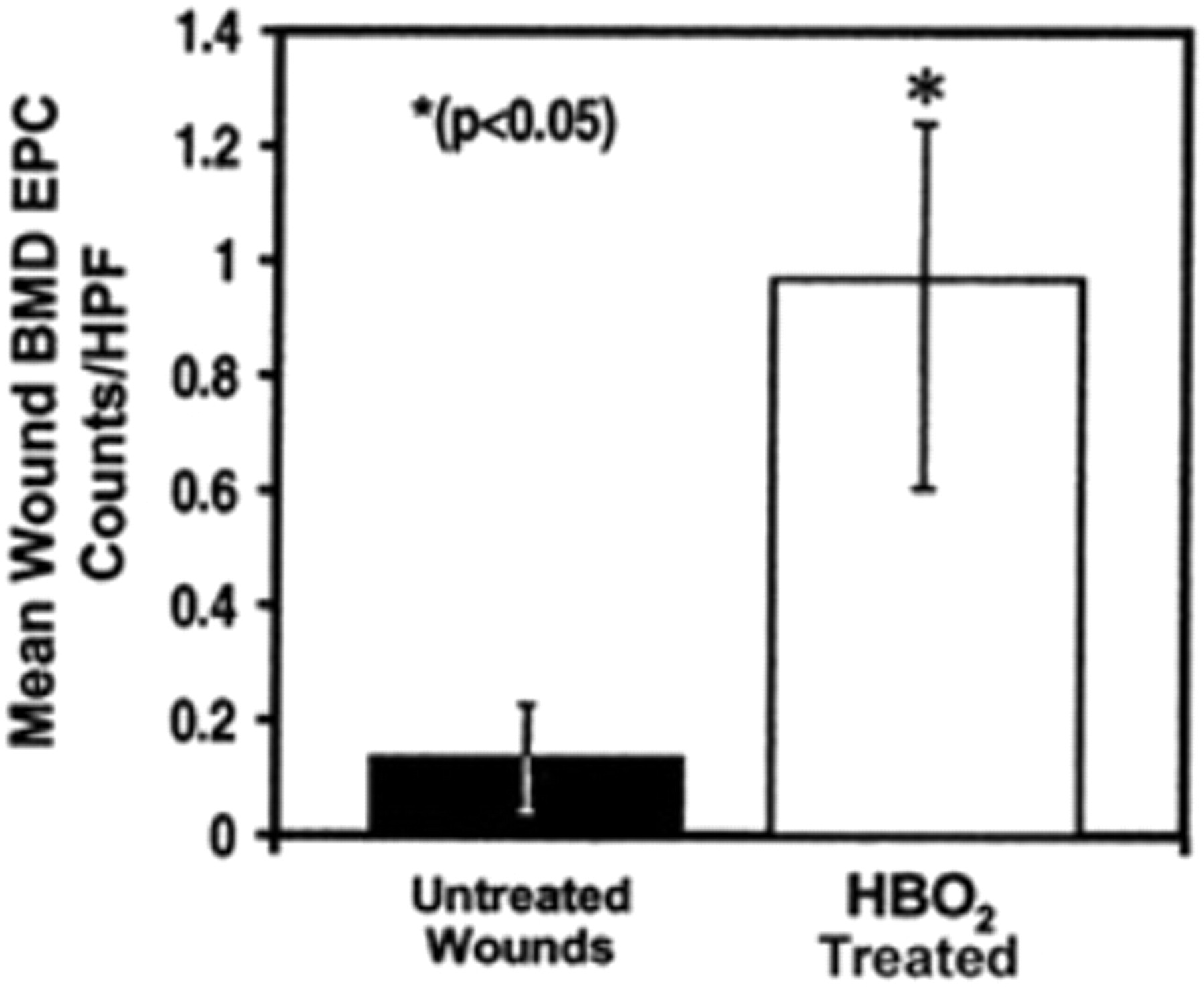
Bone marrow–derived endothelial progenitor cells (BMD EPC) are significantly increased in incisional wounds with daily hyperbaric oxygen (HBO2) treatment. BMD EPCs were tracked to wounds using the friend virus B (FVB)/Tie-2-LacZ chimeric mice. Wound biopsies were obtained after four HBO2 daily treatments; HBO2was started on the day of wounding (n = 3 mice per group). HPF = high-power fields.

Ischemic excisional wounds close significantly faster with hyperbaric oxygen (HBO2). Friend virus B (FBV) mice underwent femoral ligation and excisional hindlimb wounds and were treated daily with HBO2for 8 days, starting on the day of wounding. Wound closure was digitally monitored, and the surface area was calculated using Image J software (National Institutes of Health).
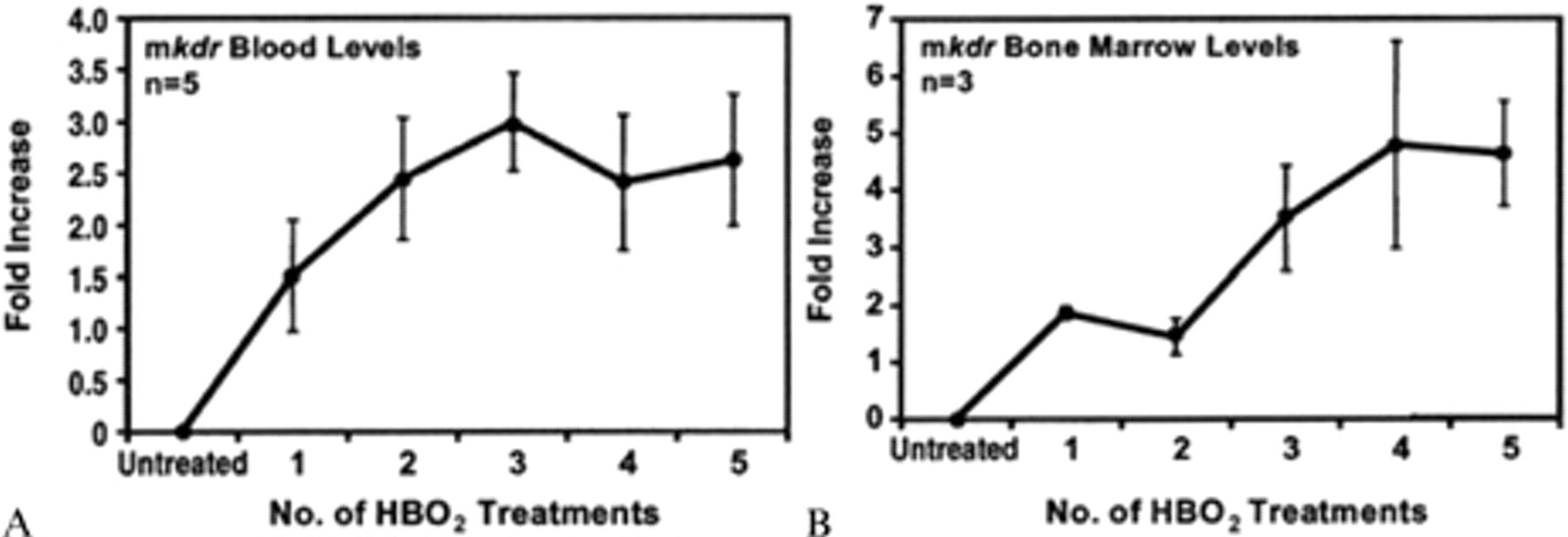
Reverse transcriptase polymerase chain reaction (RT-PCR) for bone marrow–derived endothelial progenitor cell marker vascular endothelial growth factor receptor 2; kinase insert domain receptor (Kdr) after hyperbaric oxygen (HBO2) treatment in friend virus B (FVB) mice blood (A) and bone marrow (B). FVB mice underwent HBO2 treatments, and each day blood and bone marrow were collected for VEGFR-2 RT-PCR; n = mice per time point; the x-axis indicates the number of daily HBO2 treatments; and the y-axis shows the relative fold increase in VEGFR-2 messenger ribonucleic acid (p < .05, starting at two treatments for blood and three treatments for bone marrow) mkdr = messenger RNA for kinase insert domain receptor.
Summary
Our data indicate that exposure to HBO2 will mobilize EPCs from the bone marrow in humans and mice and that this appears to be a