
Abstract
The gold standard conduit for bypass of diseased small-diameter arteries remains autologous vascular tissue. In the absence of such tissue, patients are offered bypass with prosthetic material, with far less durable results. Vascular tissue engineering, the creation of a vascular conduit by seeding a tubular scaffold with various cells, may offer an alternative approach to this difficult situation. Herein we review some of the significant challenges that remain in designing an ideal vascular conduit and outline potential solutions offered by a graft created by seeding natural vascular tissue (decellularized vein allograft) with readily available autologous cells (adipose-derived stem cells).
Attempts to improve the durability of prosthetic grafts began in the 1970s with the concept of seeding the luminal surface of the graft, considered to be thrombogenic, with endothelial cells. 1 The major technical feat overcome by extensive work in the 1980s and 1990s centered on preventing the cells from being dislodged by luminal blood flow on implantation of the graft. Strategies to overcome this problem include precoating the graft with various adhesives, 2 pressure sodding, 3 modification of the graft surface with RGD moieties, 4 prolonged culture of the graft, 5 and flow conditioning. 6–8
Although cell retention is critical to the creation of a successful graft, overcoming this problem has not led to widespread use of this approach. Significant concerns over the prosthetic nature of the scaffold and difficulty in obtaining autologous endothelial cells still remain. With these two issues in mind, we describe the evolution and bench-top testing of a new tissue-engineered vascular graft.
Scaffold Choice
As noted, prosthetic material has served as the traditional scaffold for vascular graft creation. Its availability and biocompatibility make it attractive for use; however, in spite of seeding, it remains prone to infection and anastomotic intimal hyperplasia owing to compliance mismatch. 9,10 Bioresorbable scaffolds, such as polyglycolic acid, may yield a more compliant construct. In theory, the extracellular matrix proteins secreted by the seeded cells eventually replace the scaffold as it dissolves. This has not proven to be the case as the microenvironment of the decomposing scaffold has deleterious effects on the cells. 11,12
A logical alternative is tissue allografts. Vascular transplants are prone to rejection, however, and have not proven durable even with immunosuppression. 13 Methods to alter the immunogenicity of the transplanted tissue include cryopreservation and removal of the cellular elements. This latter strategy may mandate additional modifications of the graft to restore endothelial and smooth muscle cell function.
We have investigated decellularized vein allograft as a scaffold for bypass graft creation. 14 Sodium dodecyl sulfate renders human saphenous vein acellular without significant disturbance of the underlying extracellular matrix proteins elastin and collagen (Figure 1). Type IV collagen, an important component of vascular basement membrane to which cells adhere, also appears to be preserved after cell removal. In vitro study demonstrates comparable burst and suture-holding strength of these specimens to native vein. When implanted into the arterial circulation for up to 2 months, decellularized vein allografts remain sturdy, demonstrate reduced hyperplasia and immunogenicity compared with nondecellularized allograft controls, and support intramural repopulation of cells that stain positive for α-smooth muscle cell actin. 15 Not surprisingly, the luminal surface of these scaffolds was covered in a compact fibrin layer (Figure 2), suggesting a role for further tissue engineering strategies, such as vascular cell seeding.

Microscopic examination of decellularized vein allograft. Light micrograph of human saphenous vein before (A) and after (B) decellularization with 0.075% sodium dodecyl sulfate (SDS) (hematoxylin-eosin stain; ×40 original magnification). Greater than 94% of cells are removed from the vein wall by this process. Scanning electron micrograph of human saphenous vein before (C) and after (D) decellularization with 0.075% SDS (×500 original magnification). The luminal surface of the decellularized vein is completely devoid of endothelial cells. Light micrograph of human saphenous vein before (E) and after (F) decellularization with 0.075% SDS (Verhoff-van Gieson stain; ×40 original magnification). Collagen and elastin fiber morphology is preserved following SDS decellularization. Immunohistochemical examination using a monoclonal antibody against human type IV collagen. Comparison of human saphenous vein before (G) and after (F) decellularization reveals that this important protein appears to be preserved following SDS decellularization.
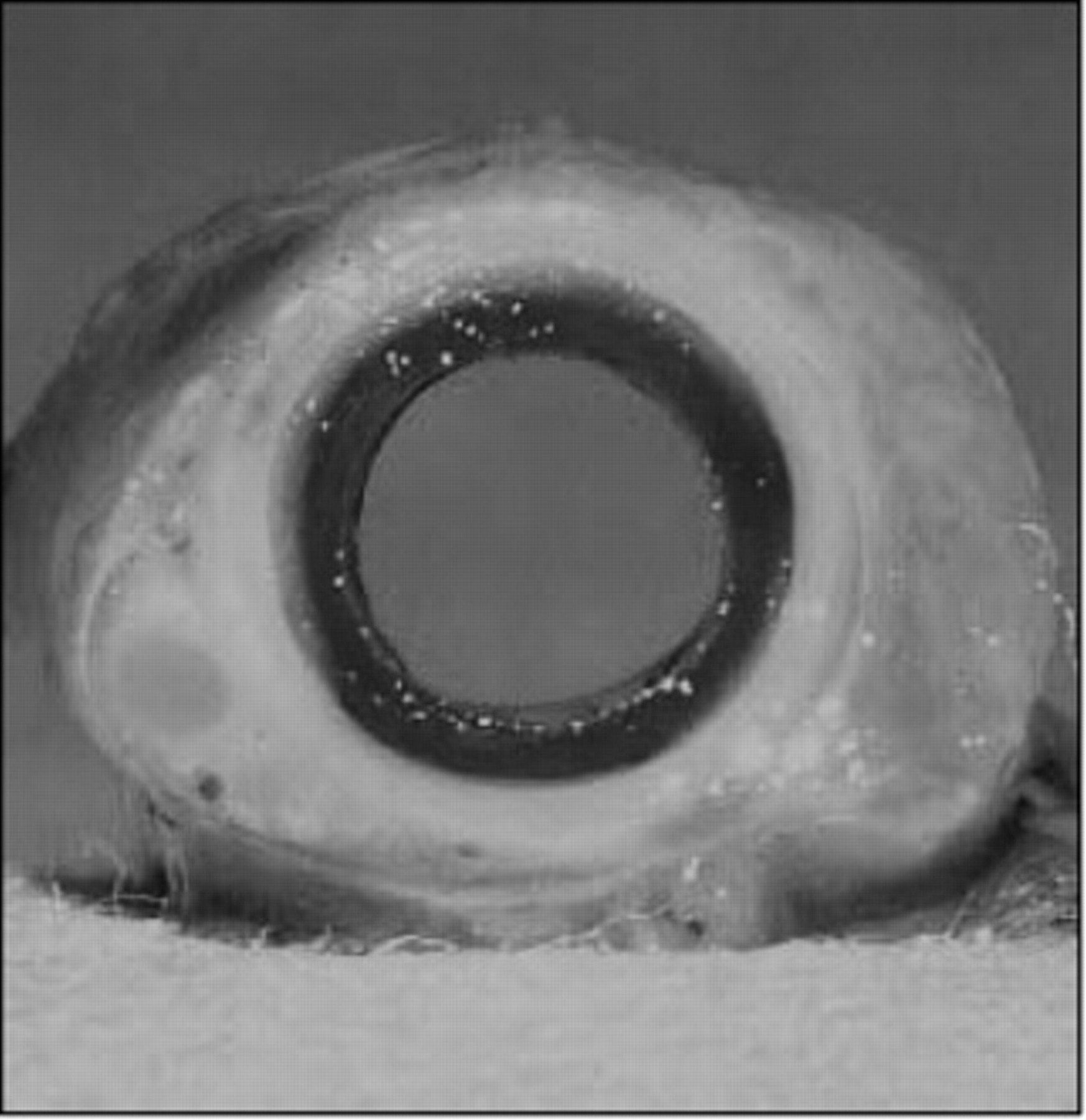
Gross examination of a decellularized vein allograft implanted into the arterial circulation for 2 months. A compact fibrin layer is seen on the luminal surface, indicating that the scaffold itself is thrombogenic secondary to the loss of endothelium. Strategies to remedy this include seeding of the lumen with vascular cells prior to implantation.
Cell Choice
The traditional cell used for luminal seeding is the differentiated endothelial cell obtained from jugular or saphenous vein segments. This strategy is disadvantaged by the need for ex vivo cell culture to obtain the number of cells necessary to seed the graft lumen. Harvest of microvessel endothelial cells from liposuctioned adipose tissue appeared promising in terms of immediate cell number 3 ; however, subsequent evaluation has suggested that contaminating cells in the isolates leads to the development of hyperplasia within the seeded grafts. 16
Endothelial progenitor cells isolated from peripheral blood hold promise for vascular tissue engineering. These cells originate from bone marrow and are a source of autologous cells for vascular repair. Their presence in peripheral blood varies with patient characteristics and may diminish with aging; therefore, use of this cell for vascular tissue engineering would also likely require ex vivo expansion. 17
We are currently investigating adipose tissue as a source of stem cells for use in graft creation. Adipose-derived stem cells (ASCs) can be isolated in abundance from liposuctioned abdominal wall fat, making them attractive for seeding. In a study of patients undergoing peripheral vascular surgical procedures, an average of 210,000 ASCs/g of adipose tissue was obtained. 18 Isolation efficiency appeared to be independent of age, gender, and peripheral vascular disease. These data indicate that in the patient population most likely to benefit from this technology, less than 50 g of adipose tissue would be required to seed a 40 cm bypass graft.
The ASC is multipotent, having been shown to differentiate into bone, cartilage, adipose, muscle, and neuron cell lines. 19,20 Germane to vascular tissue engineering, we have begun to define its ability to differentiate into cells with an endothelial phenotype. Endothelial characteristics in these experiments were defined as realignment in the direction of luminal flow, cord formation in response to extracellular matrix (Matrigel), and the expression of endothelial cell message and protein (endothelial nitric oxide synthase, von Willebrand's factor, CD31).
Two specific stimuli for differentiation have been examined in vitro: chemical stimuli with vascular endothelial growth factor and other growth factors (unpublished data, 2006) and physical stimuli with shear stress. 21 Prior to stimulation, ASCs are negative for each of the above-noted endothelial characteristics. After culture in differentiating media for up to 3 weeks, the stem cells realign with flow and form cords in response to Matrigel (Figure 3). Additionally, the cells express endothelial nitric oxide synthase and von Willebrand's factor, as demonstrated by reverse transcriptase polymerase chain reaction and immunohistochemical analysis. CD31 was further expressed after exposure to physiologic shear stress (10 dynes/cm 2 ) for 2 days (Figure 4). Taken together, these studies suggest a role for ASCs in vascular tissue engineering strategies.
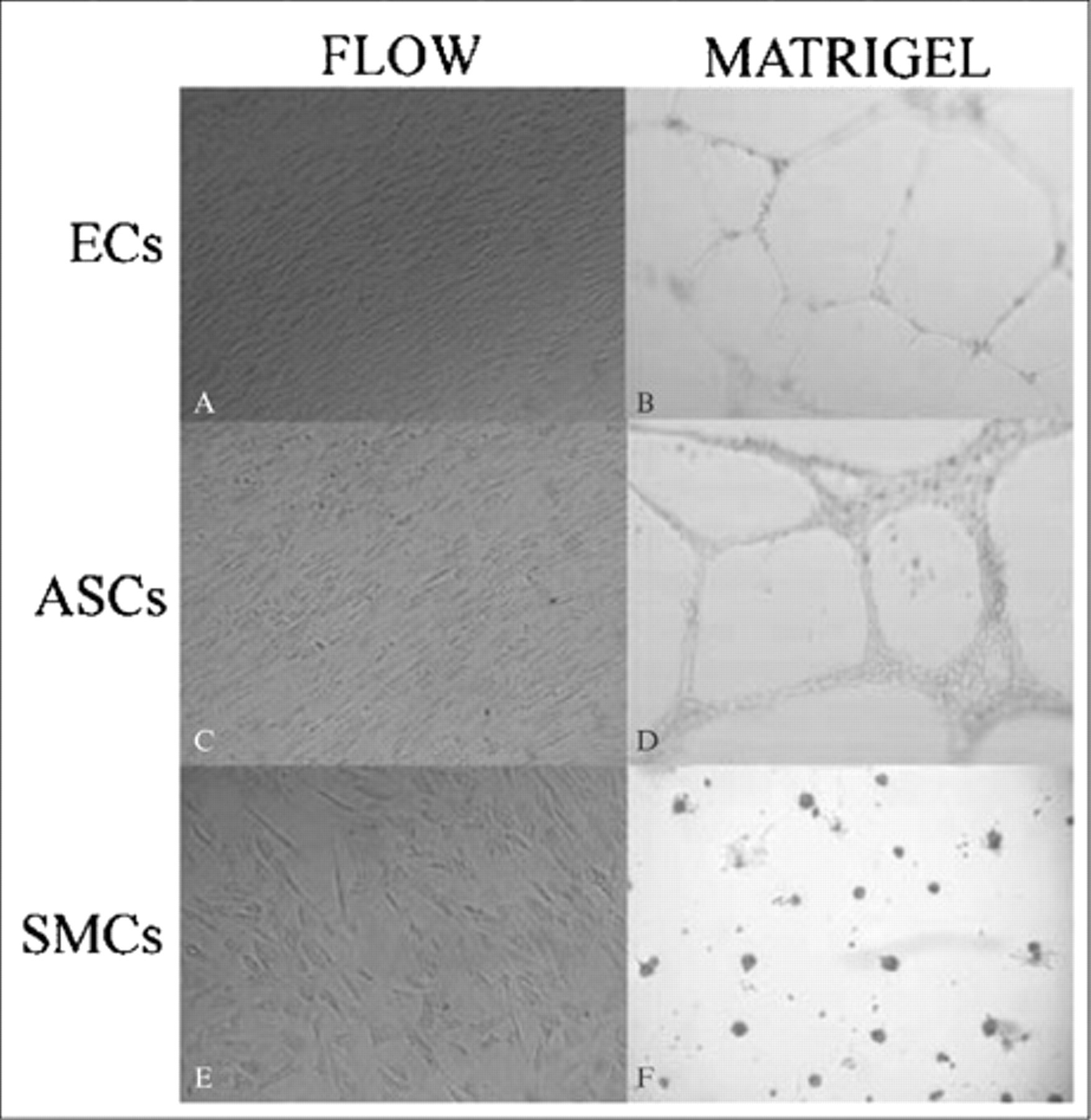
Acquisition of endothelial cell phenotype by differentiating adipose-derived stem cells (ASCs). ASCs naive to differentiating media are not responsive to shear stress, nor do they form cords in response to Matrigel (not shown). After growth in the media, they realign with flow (C) and form cords (D) similar to endothelial cell (EC) controls (A and B). Smooth muscle cell (SMC) responses (E and F) are shown as a negative control (×40 original magnification).
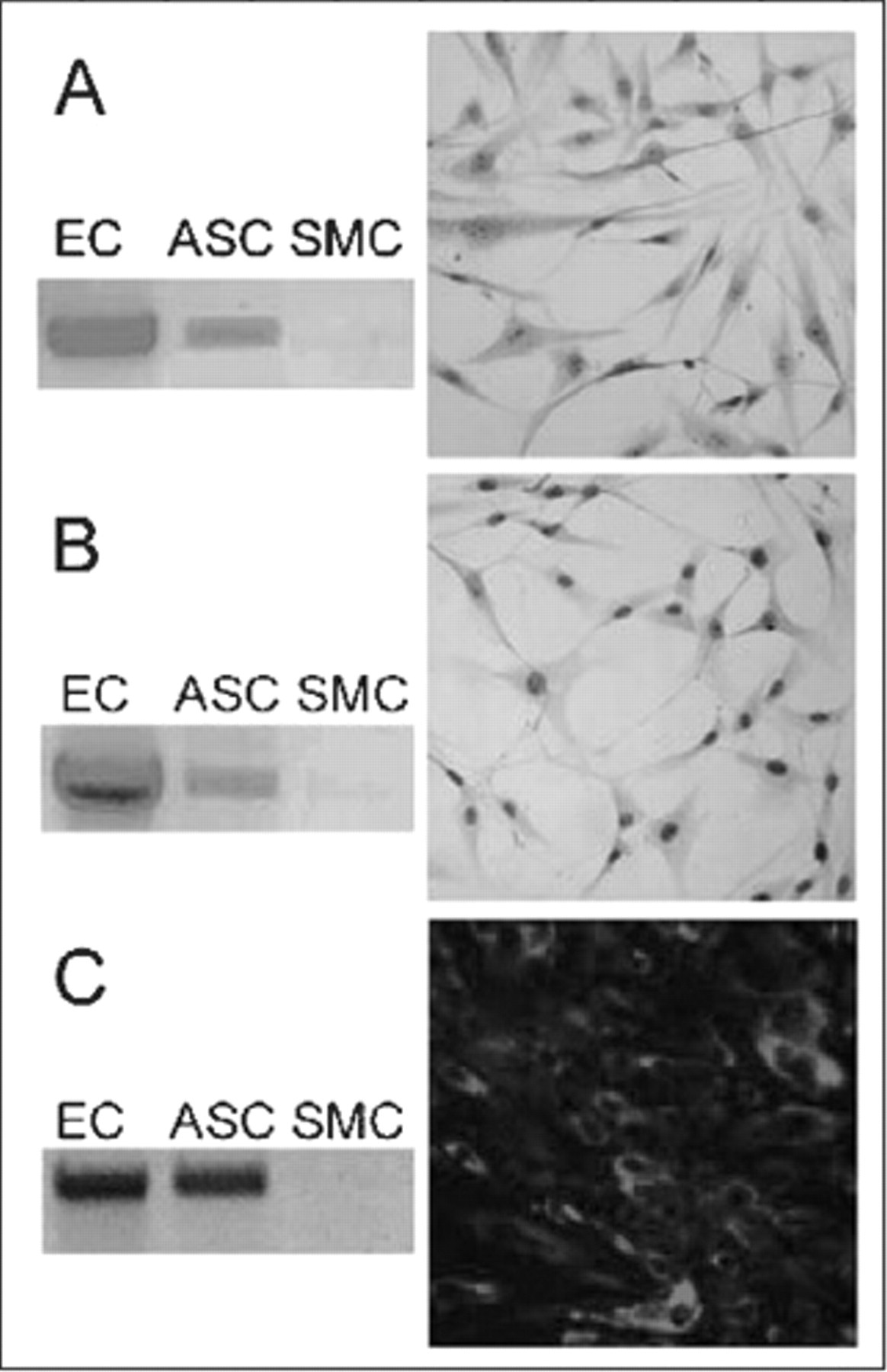
Expression of endothelial cell (EC) protein by differentiating adipose-derived stem cells (ASCs). After growth in differentiating media, ASCs express endothelial nitric oxide synthase (A) and von Willebrand's factor (B), as demonstrated by reverse transcriptase polymerase chain reaction and immunohistochemical staining. After exposure to the media and subsequently to shear stress, CD31 is also expressed (C). EC and smooth muscle cell (SMC) controls are shown (×40 original magnification; stains to human eNOS, vWF, and CD31).
Graft Creation and In Vivo Testing
ASCs have been seeded onto the luminal surface of decellularized vein within a bioreactor that maintains the necessary culture conditions for cell survival. 22 Under gravitational force, cell attachment and spreading typically occur within 2 hours. Seeding with a minimum of 2 × 105 cells/cm2, ASCs form a confluent monolayer on the luminal surface (Figure 5).
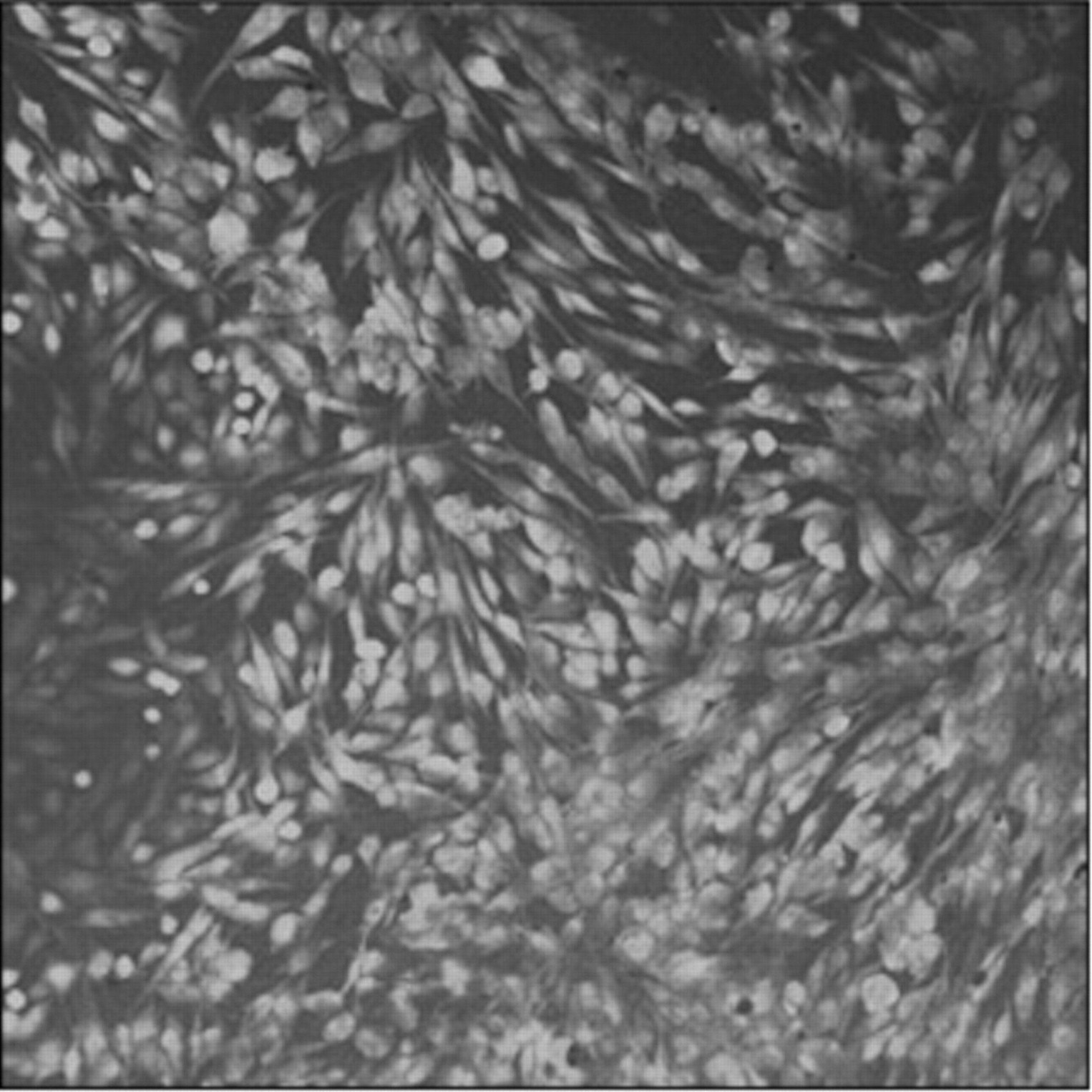
Attachment of stem cells onto the luminal surface of the scaffold. Laser confocal microscopy reveals a confluent monolayer of adipose-derived stem cells 1 day after seeding (Cell Tracker Green, Invitrogen Corp., Carlsbad, CA). (×40 original magnification).
In vivo examination of the graft prototype has recently begun using a canine model (unpublished data, 2006). In these experiments, ASCs were isolated from the falciform ligament and seeded onto decellularized canine vein allograft (external jugular vein). After 1 day in culture, the grafts were placed as carotid interposition grafts for a 2-week period. Preliminary study revealed a thin layer of fibrin on the graft surface, suggesting that undifferentiated ASCs may not immediately form a nonthrombogenic layer. These early results indicate that differentiation of these cells prior to implantation may be necessary for ultimate clinical success.
Future Directions
These studies demonstrate the feasibility of using decellularized vein allograft as a scaffold for creating a tissue-engineered graft. Ideally, this would be manufactured as a readily available “off-the-shelf” product to be seeded by a patient's autologous cells as the need arises. For example, saphenous vein could be harvested from cadaver tissue donors, decellularized, and cryopreserved. Future investigation of the effect of cryopreservation on the conduit as a scaffold is necessary. It is likely that this process will further decrease the immunogenicity of the matrix, but its impact on strength and seeding is unknown.
The use of stem cells in vascular tissue engineering is going to increase dramatically in the future, especially when funding for embryonic stem cell research comes to fruition. For now, autologous adult stem cells, such as those derived from adipose tissue, appear to have significant potential given their availability and multipotency. Additionally, the concept of seeding a single cell type that can acquire multiple vascular cell phenotypes (ie, both endothelial and smooth muscle) is certainly attractive. Continued study of various physical and chemical stimuli that alter the microenvironment of these cells both in vitro and in vivo will better define a role for ASCs in vascular tissue engineering.
Summary
Developing a tissue-engineered bypass graft is replete with technical and practical challenges. Ideally, the construct would be readily available, biocompatible, and durable. With every new scaffold-cell combination, significant issues concerning scaffold strength and compliance, cell availability, and retention on seeding must be addressed. In vivo testing becomes critical as it helps define both the efficacy of the graft and the practicality of producing it. Keeping graft creation simple and keeping it compact in terms of time are likely the two biggest hurdles blocking the widespread use of this technology.
Footnotes
Grant support: National Institutes of Health, National Heart, Lung, and Blood Institute K08, American Heart Association, American Vascular Association, Pacific Vascular Research Foundation, Cardiovascular Institute of Philadelphia, and Kidney Foundation of Central PA