
Abstract
The intravascular and extravascular effects of percutaneous closure devices have not been well studied. We assessed the performance and healing characteristics in dogs of two devices approved by the US Food and Drug Administration.
Nine adult male dogs were anesthesized prior to percutaneous access of both femoral arteries with a 6F sheath. All dogs were systemically heparinized to an activated clotting time (ACT) > 250 seconds. Duplex sonography was performed preoperatively to measure vessel diameter and flow velocity. In each dog, one of two devices (Perclose, Abbot Laboratories, Abbott Park, IL or Angio-Seal, St. Jude Medical, St. Paul, MN) was randomly deployed into one of the two femoral arteries. The other device was deployed on the opposite side. Duplex sonography was repeated immediately after deployment and 28 days later to measure changes in vessel diameter and flow velocity. At 28 days, angiography was performed on both femoral arteries before they were removed for histologic evaluation. The time required to excise each vessel reflected the degree of scarring.
Hemostasis time for the Angio-Seal device far surpassed the Perclose device (39 ± 7 vs 0 minutes; p < .05). Vessel narrowing was observed only at 28 days after deployment of the Angio-Seal device (p < .05). Extensive extravascular scarring was observed with the Angio-Seal device, which resulted in a longer femoral artery dissection time and greater periadventitial scar thickness compared with the Perclose device (p < .05).
When compared with the Perclose suture closure device, the Angio-Seal collagen plug closure device prolonged hemostasis time and produced greater vessel narrowing and periadventitial inflammation (extravascular scarring) in a canine model at 4 weeks.
Diagnostic and therapeutic arteriographic procedures are increasingly being done on an ambulatory basis to improve overall patient care since many patients prefer to return home after such procedures. As a result, new technologies have been developed for arterial interventional procedures to provide immediate and secure hemostasis.
The Perclose Closer (Abbot Laboratories, Abbott Park, IL) and the Angio-Seal Millennium (St. Jude Medical, St. Paul, MN) devices are two widely used puncture-site closure devices. 1,2 These devices are designed to provide immediate hemostasis and allow prompt ambulation. This eliminates the 10- to 15-minute period of arterial compression and 4- to 6-hour supine period often required after arteriographic procedures.
Furthermore, many patients undergoing coronary or peripheral arteriographic procedures require systemic heparinization and/or the administration of IIb/IIIa inhibitors. 3–5 These require prolonged manual compression and contribute to further puncture-site complications. An additional advantage of the closure devices includes their ability to achieve immediate and secure hemostasis in patients requiring continued systemic anticoagulants and platelet inhibitors. 4 , 5
There has been controversy regarding the merits and liabilities of these devices and whether they justify their costs. However, several adverse events have been associated with these devices, including distal embolization, femoral artery thrombosis, pseudoaneurysms, arteriovenous fistulae, infection, and uncontrolled hemorrhage. 6–11 Whether these complications remain device specific remains unknown. To date, no experimental studies have been reported comparing performance characteristics and histologic changes after different closure devices. We therefore compared the healing characteristics and performance of two commercially available femoral artery closure devices approved by the US Food and Drug Administration in a canine model.
Methods
Nine adult male greyhound dogs (weight 70–90 kg) were housed in an animal care facility according to the animal use protocol of the Albert Einstein College of Medicine Institutional Animal Care and Use Committee. All of the dogs underwent anesthesia with thiopental and isoflurane and were intubated with a 6.0 cm endotracheal tube. All of the dogs were then systemically heparinized to an activated clotting time (ACT) > 250 seconds after the administration of 1,500 U of heparin sodium. A prophylactic dose of 250 mg of intravenous cefazolin was also given prior to any percutaneous intervention.
Preoperative Duplex Sonography
Vessel diameter (cm) and flow velocity (cm/s) were measured by duplex sonography prior to any manipulation of the canine femoral arteries. These were recorded for statistical analysis.
Percutaneous Puncture and Device Deployment
Both groins were shaved and prepared. Six French sheaths (Avante, Cordis, Warren, NJ) were percutaneously deployed into both femoral arteries using the Seldinger technique under fluoroscopic control. Diagnostic angiography was then performed to exclude evidence of arterial dissection, thrombosis, and embolization. Either the Perclose Closure or the Angio-Seal Millenium device was randomly deployed into one of the femoral arteries by an interventionalist who was well trained beyond the learning curves of both devices. The recorded ACT was about 250 seconds, and the mean arterial pressure was 60 to 70 mm Hg at the time of device deployment. Hemostasis time was recorded after each deployment. Duplex sonography was then repeated to evaluate the presence or absence of narrowing that may have been caused by the closure device. Vessel diameter (cm) was measured with B-mode imaging, and increase in flow velocity (cm/s) was recorded using color duplex sonography (Advanced Technological Laboratories, High Definition Imaging 5000).
Techniques of Device Deployment
Perclose
The Perclose device (Figure 1) is backloaded on a guidewire and positioned exactly to ensure appropriate needle deployment. Pulsatile backbleeding from the marker lumen confirms the intra-arterial device position so that lance-like needles can be deployed in a retrograde fashion. After deployment, the needles are retracted and the sutures are tied in a square knot to close the arterial defect.
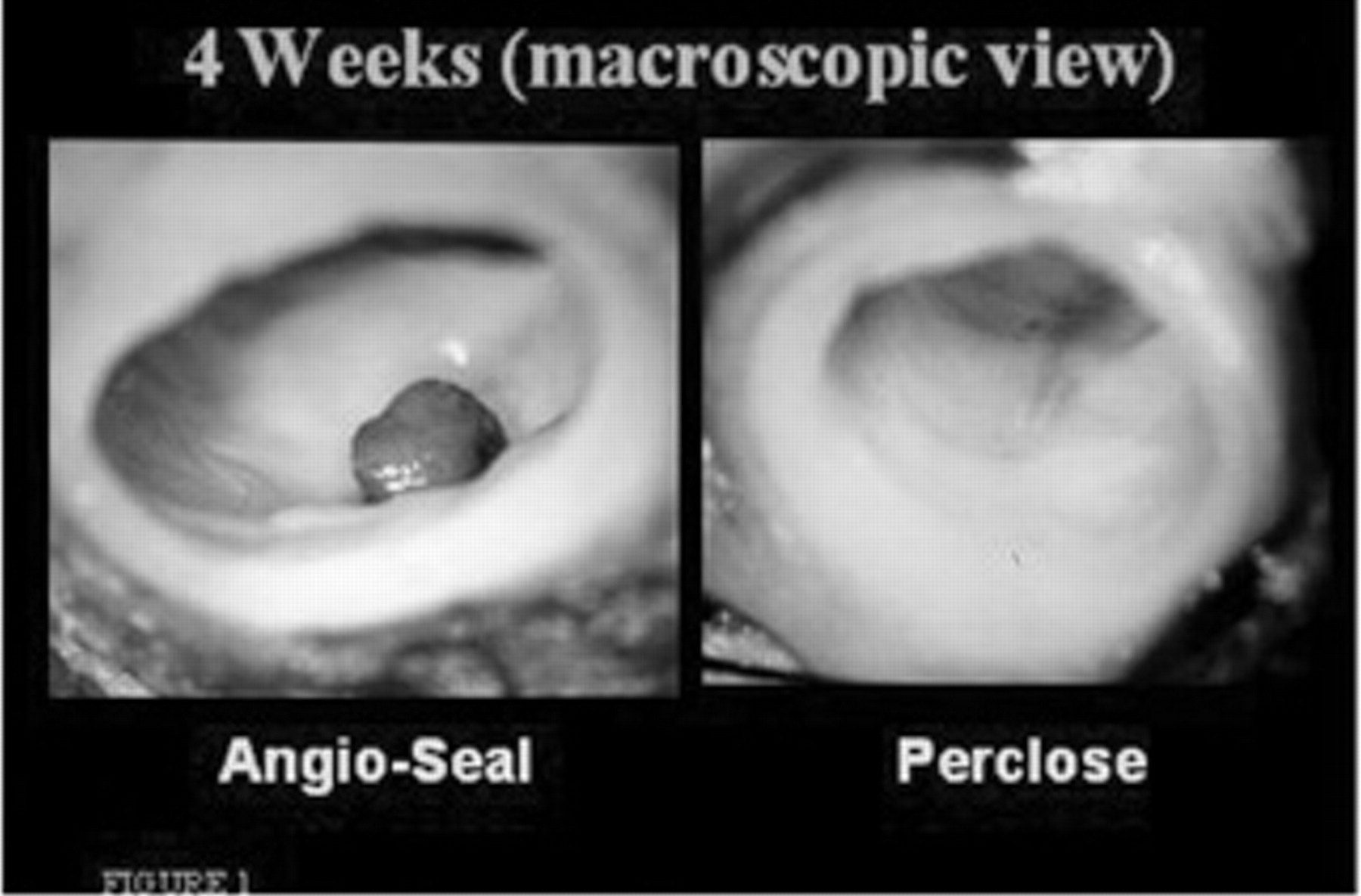
The Angio-Seal intraluminal lump (left) may be seen macroscopically on cross-sectional view of the femoral artery. Minimal intraluminal changes are made with the Perclose absorbable stitch (right).
Angio-Seal
The Angio-Seal insertion system is introduced through the locator sheath and the anchor is placed against the luminal aspect of the arterial wall. By retraction of the whole application system, anchor and collagen sponge are drawn together. The collagen sponge is tamped onto the outer arterial wall to secure the seal. A spring maintains controlled tension for 15 minutes before being disconnected. The newer-generation Angio-Seal device does not mandate spring tension for 15 minutes or tamping of the collagen plug.
Postoperative Duplex Sonography and Histologic Analysis
At 28 days, each dog was again anesthetized and intubated. Duplex sonography measuring vessel diameter (cm) and flow velocity (cm/s) was performed prior to harvesting both common femoral arteries. Diagnostic arteriography of both common femoral arteries was performed via the left common carotid artery, documenting the absence of dissection, thrombosis, embolization, and luminal narrowing. Bilateral groin incisions were made, and dissection times for both common femoral arteries were recorded. A well-trained and experienced vascular surgeon performed all femoral artery dissections. This time reflected the degree of scarring. All branches were secured with 3-0 silk ligatures.
Both common femoral arteries were then excised and irrigated with heparinized 0.9% saline. Pressure fixation of the specimens was performed with 10% formalin solution at 100 mm Hg for 72 hours.
At 72 hours, each specimen was dehydrated with serial alcohol and embedded in paraffin using standardized technique. Specimens were then sectioned and stained with hematoxylin and eosin and Evan's stains. They were then analyzed microscopically. The degree of intimal hyperplasia (intima to media ratio) and extravascular scarring was measured.
Statistical Analysis
All results are expressed as the mean ± standard error of the mean. Hemostasis time, time required for vessel dissection at harvest, change in vessel diameter, intimal hyperplasia, and extravascular scarring were analyzed for between-group differences with the paired Student's t-test. Significance was determined as a p value less than .05, as determined with SPSS sofware (SPSS Inc, Chicago, IL).
Results
The nine dogs lived for 28 days and completed the experimental protocol. Hemostasis time, time required for vessel dissection at harvest, change in vessel diameter, intimal hyperplasia, and extravascular scarring were recorded for all 18 common femoral arteries in the nine dogs. Table 1 summarizes the results.
Details of Closure Devices
*p < .05.
Hemostasis Time
Angio-Seal device deployment required 39 ± 7 minutes of additional hemostasis time with manual compression. The Perclose device resulted in immediate hemostasis following suture fixation.
Narrowing of Vessel Diameter
Arteriography
No significant abnormalities were seen on any of the arteriograms performed prior to duplex sonography and harvesting of the femoral arteries.
Duplex Finding
Mild vessel diameter narrowing was observed with the Angio-Seal device at 28 days following device deployment, as shown by an increase in flow velocity. There was no appreciable change in actual vessel diameter as measured by duplex sonography. The average vessel diameter was between 3 and 4 mm both pre- and postdeployment. The intra-arterial anchor used in the Angio-Seal was clearly seen on the B-mode image, and this resulted in increased flow velocity. There was no change in vessel luminal diameter following deployment of the Perclose device, and B-mode analysis failed to detect the presence of a foreign body intra- and extraluminally.
Macroscopic Finding (Intraluminal)
With the Angio-Seal, even at 28 days, there was an intraluminal lump caused by the plug, whereas with the Perclose, only a suture was seen. This suture was covered with thin neointimal tissue (see Figure 1).
Intimal Hyperplasia
Neither device resulted in significant intimal hyperplasia at 28 days. Of note, however, is the marked degree of intimal, medial, and adventitial disruption resulting from the Angio-Seal device compared with the Perclose device (Figure 2).
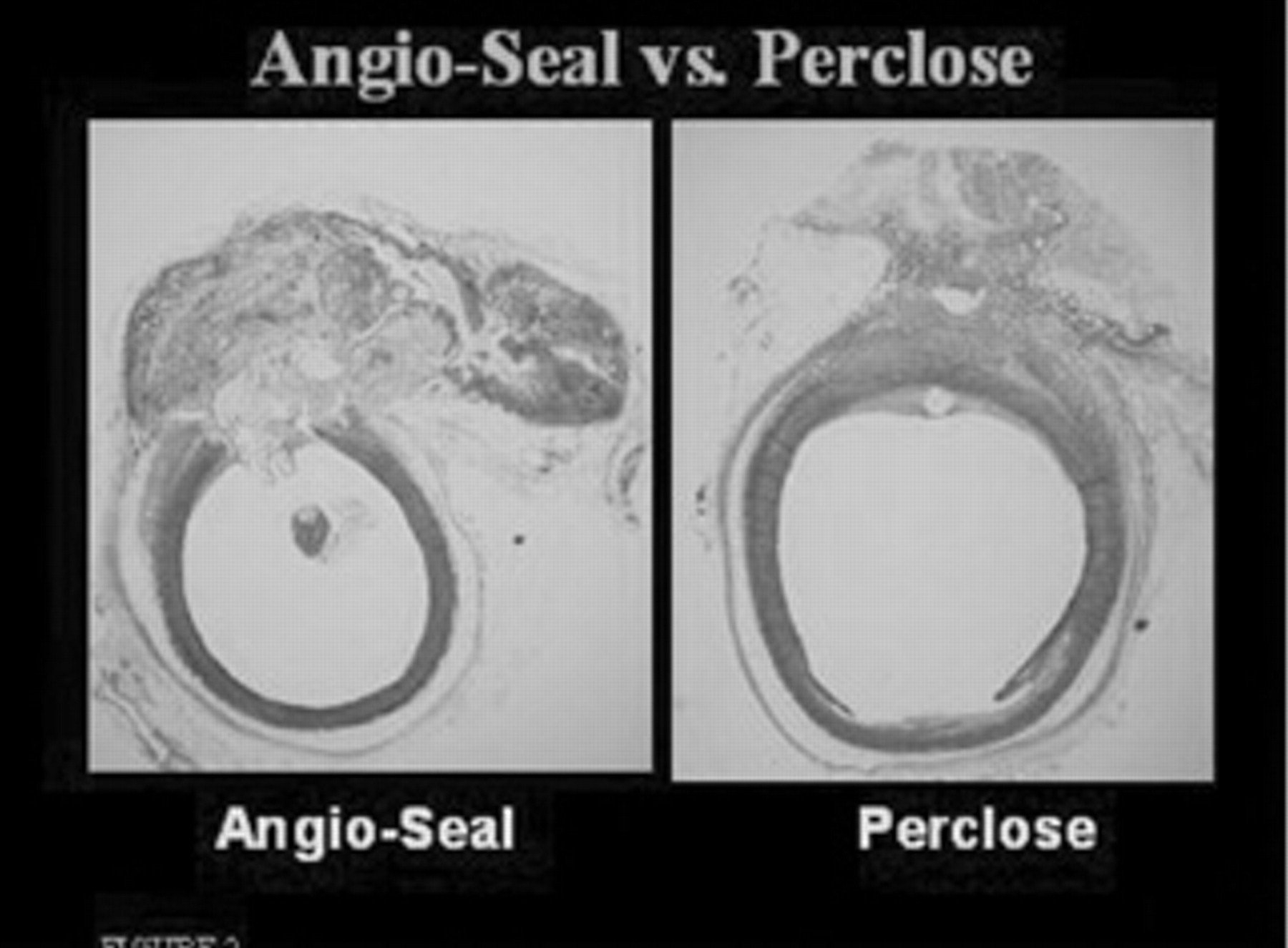
Significant arterial wall disruption may be seen histologically with the Angio-Seal device (left). Extensive destruction of intima, media, and adventitial layers is present. The Perclose device (right) maintains arterial wall integrity.
Extravascular Scarring
Extravascular scarring was most notable for the Angio-Seal device. This was determined not only by the added femoral artery dissection time but also by the intense extraluminal inflammatory response observed macroscopically and histologically.
Discussion
Percutaneous closure devices have revolutionized diagnostic and therapeutic cardiac and noncardiac arteriographic procedures. The ability to provide immediate hemostasis translates into an earlier return to ambulation, an overall improvement in patient comfort, and a reduction in hospital length of stay. These devices are especially valuable for patients who need continued heparinization or those who receive IIb/IIIa inhibitors. 12 However, not all closure devices are equal, and not all interventionalists have acquired the same level of expertise in device deployment. Complications associated with all closure devices include distal embolization, pseudoaneurysm formation, arterial thombosis, infection, and uncontrolled hemorrhage. 6–11 These complications may be fatal and thwart a successfully executed interventional procedure. As a result, closure devices have been subjected to intense scrutiny by many interventionalists.
Most of the prospective, randomized trials comparing manual compression with percutaneous closure of arteriotomies report no significant difference in overall outcome or complication rate. 13,14 However, several case reports have reported catastrophic events following the percutaneous closure of arteries. 6,10 There are currently no clinical reports comparing the different types of closure devices, namely suture-mediated closure (Perclose) versus collagen plug and anchor closure (Angio-Seal). Furthermore, there are no studies to date reporting on the histologic changes that occur in the artery after different closure device deployment.
Suture-mediated closure of a percutaneous arteriotomy has several benefits over a collagen plug and anchor closure. Immediate hemostasis and minimal foreign body are by far the main advantages, as observed in our study. Historically, surgical closure using a suture of an open arteriotomy has been the gold standard. It results in immediate hemostasis, minimal foreign body reaction, and intimal hyperplasia. Any deviation from this simple technique, such as the use of an intra-arterial anchor attached to an extraluminal collagen plug, would undergo intense scrutiny. Suture-mediated closure of a percutaneous arteriotomy is therefore an obvious application of standard open surgery. Perclose device deployment achieved the same result and required no further manual compression in this study. Angio-Seal device deployment did not achieve this result and required manual compression to achieve hemostasis in seven of nine femoral arteries.
It is unclear why the Angio-Seal device did not achieve immediate hemostasis, although the newer-generation device was not available for use in these experiments. One hypothesis may be that a larger than expected space may be created between the extraluminal collagen plug, the arterial wall, and the intraluminal anchor, hence allowing an egress of blood. This certainly contrasts with the blood impervious seal of the Perclose device. This may not be the case in the setting of severely diseased arterial walls, as experienced clinically in human cases. All of the canine arteries were 2 to 3 mm smaller than the recommended size for use of these closure devices, which may have increased overall hemostasis time. Suture-mediated closure may be hindered by plaque and calcification, which hinders a blood-tight seal. In addition, occlusion of diseased arteries has been reported. 11 One weakness of this study is that both closure devices were deployed into healthy, canine femoral arteries free of plaque and calcification.
Minimal extravascular scarring was observed with the Perclose device both surgically and histologically. The time to dissect out the femoral artery on the Angio-Seal side far surpassed that on the Perclose side. This has several important clinical ramifications for the interventionalist and the surgeon. The intense inflammatory reaction of the Angio-Seal device complicates repeat percutaneous puncture and open arterial exposure if this is required to repair a pseudoaneurysm or occlusion. Furthermore, impairing femoral arterial dissection for future elective procedures contributes to surgical morbidity.
Time to dissection of the femoral artery also correlated with histologic changes. An intense extravascular scarring was seen on the extraluminal surface of the femoral arterial Angio-Seal closure site associated with the collagen plug. Furthermore, this scarring was contiguous with intra-arterial intimal disruption associated with the anchor. These histologic findings were not observed at the femoral artery Perclose closure site.
Rather unexpectedly, no statistical difference was seen in either vessel narrowing immediately following device deployment or intimal hyperplasia at 28 days between the two devices. Vessel narrowing was observed at the femoral arterial puncture site on the Angio-Seal side at 28 days. This is due to the fact that the Angio-Seal anchor, which measures 2 × 10 mm, was deployed into the arterial lumen. This may not be clinically relevant in normal femoral arteries, but in those with significant plaque or calcification, it may be a problem.
Additonally, the intra-arterial anchor of Angio-Seal is a rather inert foreign body limiting the intra-arterial inflammatory response. Inadvertent delivery of the collagen plug intra-arterially by an inexperienced interventionalist would certainly result in profound intimal hyperplasia, as observed extraluminally with the intense extravascular scarring.
As expected, minimal vessel narrowing and intimal hyperplasia were observed with the Perclose device. When deployed correctly by an experienced interventionalist, Perclose is the preferred closure device. However, it is more technically demanding to deploy since there are more steps in deployment. Furthermore, the need to tie and secure the suture requires some experience and skill. A learning curve certainly exists. However, ease of use should not offset some of the important differences noted in this study. Absence of intraluminal and extraluminal scarring is by far more important than ease of use, especially for the patient. Additionally, difficulties in penetrating a calcified arterial wall with the Perclose needles may be one advantage of the Angio-Seal device in achieving hemostasis. Physicians who are currently using these devices need to be aware of the intra- and extraluminal changes that take place following closure devices.
Limitations
It cannot be emphasized enough that the observations made in this study are all based on canine arteries. Extrapolating these observations to human arteries should be made with caution and should in no way preclude the use of either the Perclose or Angio-Seal closure devices. Both closure devices have clearly revolutionized patient care over the past two decades and are effective and safe devices when used correctly by an experienced interventionalist.
Additionally, the canine arteries in this study were 2 to 3 mm smaller than human arteries and would, in most clinical situations, be a contraindication to the use of such closure devices. Furthermore, because of financial constraints, the canine arteries were harvested at 4 weeks instead of 6 weeks, when much of the arterial inflammation is thought to resolve after Angio-Seal use.
Footnotes
This study was sponsored in part by Abbott Vascular, Inc., Abbott Park, IL.