
Abstract
Use of endovascular interventions for arterial occlusive lesions continues to increase. With the evolution of the technology supporting these therapeutic measures, the results of these interventions continue to improve. In general, a comparison of techniques for revascularization of iliac occlusive diseases shows similar initial technical success rates for open versus percutaneous transluminal angioplasty. Angioplasty is often associated with lower periprocedural morbidity and mortality rates. Conversely, surgery frequently provides greater long-term patency, although late failure of percutaneous therapies may occur but still can be treated successfully with reintervention. The perpetual buildup of experience with angioplasty and stenting will eventually characterize its role in the management of occlusive disease. This review outlines the current consensus and applicability of endovascular management of iliac occlusive diseases.
In this era of “endovascular revolution,” it is crucial for a vascular surgeon to keep apprised of the latest surgical approaches to treating iliac artery occlusive diseases, bearing in mind that treatment should be tailored for every patient according to an individual's morphology and comorbidity. This review article is designed to highlight the most recent philosophies in the management of iliac occlusive diseases.
Open versus Endovascular Techniques
Generally, TransAtlantic Inter-Society Consensus (TASC) type A lesions are best treated with endovascular therapy, whereas TASC type D lesions are best treated with surgical revascularization (TASC lesion types are described in Table 1). 1 However, the revolution in endovascular technology has expanded the feasibility and applicability of percutaneous treatment. A recent meta-analysis review showed significant improvement in functional capacity and ankle-brachial index after percutaneous revascularization in claudicants. 2 Some recent studies report encouraging results in patients with intermittent claudication suffering from TASC type C and D iliac disease. 3,4 They concluded that open surgical bypass should be delegated to those patients without an endovascular option. However, despite more than a decade of experience with these techniques, debate continues regarding the optimal strategy for flow restoration and the use of stents, especially for TASC type C and D iliac disease. Historically, iliac angioplasty alone has proven to be quite favorable, with a reported technical success rate ranging from 50 to 96% and 2- and 5-year patency rates averaging 81 and 72%, respectively. 2 Outcomes are particularly advantageous for short stenoses and occlusions, as well as for lesions localized to the common iliac artery (CIA), which together comprise nearly half of all iliac lesions referred for treatment. 5 Additionally, angioplasty with stenting may be appropriate for patients deemed at high operative risk of conventional repair. 6–8
TASC Iliac Lesion Types
CFA = common femoral artery; CIA = common iliac artery; EIA = external iliac artery; TASC = TransAtlantic Inter-Society Consensus.
Angioplasty
Percutaneous angioplasty by means of coaxial dilating catheters was first reported by Dotter and Judkins in 1964. 9 However, modern percutaneous angioplasty came of age with the introduction of balloon catheters in the 1970s by Grüntzig. 10 Percutaneous transluminal angioplasty (PTA) used for focal iliac artery stenoses demonstrated acceptable success rates (Figure 1). Parsons and colleagues reported that the results of catheter-based interventions on the iliac vessels have approached those of open surgery. 11 This technique is applicable not only to chronic ischemia but also to acute limb ischemia. 12 However, in some early studies, the definitions of success were not well defined and treatment of complex disease was not completely reported. Iliac angioplasty has been used not only as a stand-alone procedure but also as a viable option for improving inflow in patients requiring distal bypass procedures. 13,14 Complications associated with PTA include vessel dissection, abrupt closure, spasm, and thrombus formation. Moreover, some studies evaluating the use of PTA for total iliac artery occlusions generally showed significant embolization, which led some to question the usefulness of PTA in this patient subset. 15–17

Aortoiliac arteriogram revealing right common iliac artery origin stenosis. Before (A) and after (B) percutaneous transluminal angioplasty. A 24% diameter luminal compromise of the left common iliac artery resulted (arrow).
In addition, combined use of PTA with or without stenting and open surgical bypass has been found to be effective and durable and can be performed simultaneously, especially for iliac lesions of less than 5 cm. 18
Endovascular Stenting
Endovascular stents have become an accepted therapy for patients with iliac occlusive disease. 19 They have been associated with symptomatic improvement and a greater than 90% patency rate. 20
Self-Expanding Stents
With the introduction of these stents, an increased number of complex diseases were treated with success rates comparable to those of open surgery. 21 Additionally, the deployment of a bifurcated stent graft appeared to be technically feasible, effective, and safe in the management of aortoiliac occlusive disease. 22
In a contemporary study, the use of the stainless steel Wallsent (Boston Scientific Corporation, Natick, MA) had a 6-year primary patency rate of nearly 80% in claudicants (Figure 2). 23 The Cordis SMART nitinol self-expanding stent (Cordis, Inc, Miami Lakes, FL), with its unique design, has contributed to greater procedural success and more accurate stent deployment. 24 Early results of stent graft placement to treat diffuse aortoiliac occlusive disease were shown to be more successful than using a stent alone. Concomitant common femoral endarterectomy may also improve the durability. 25
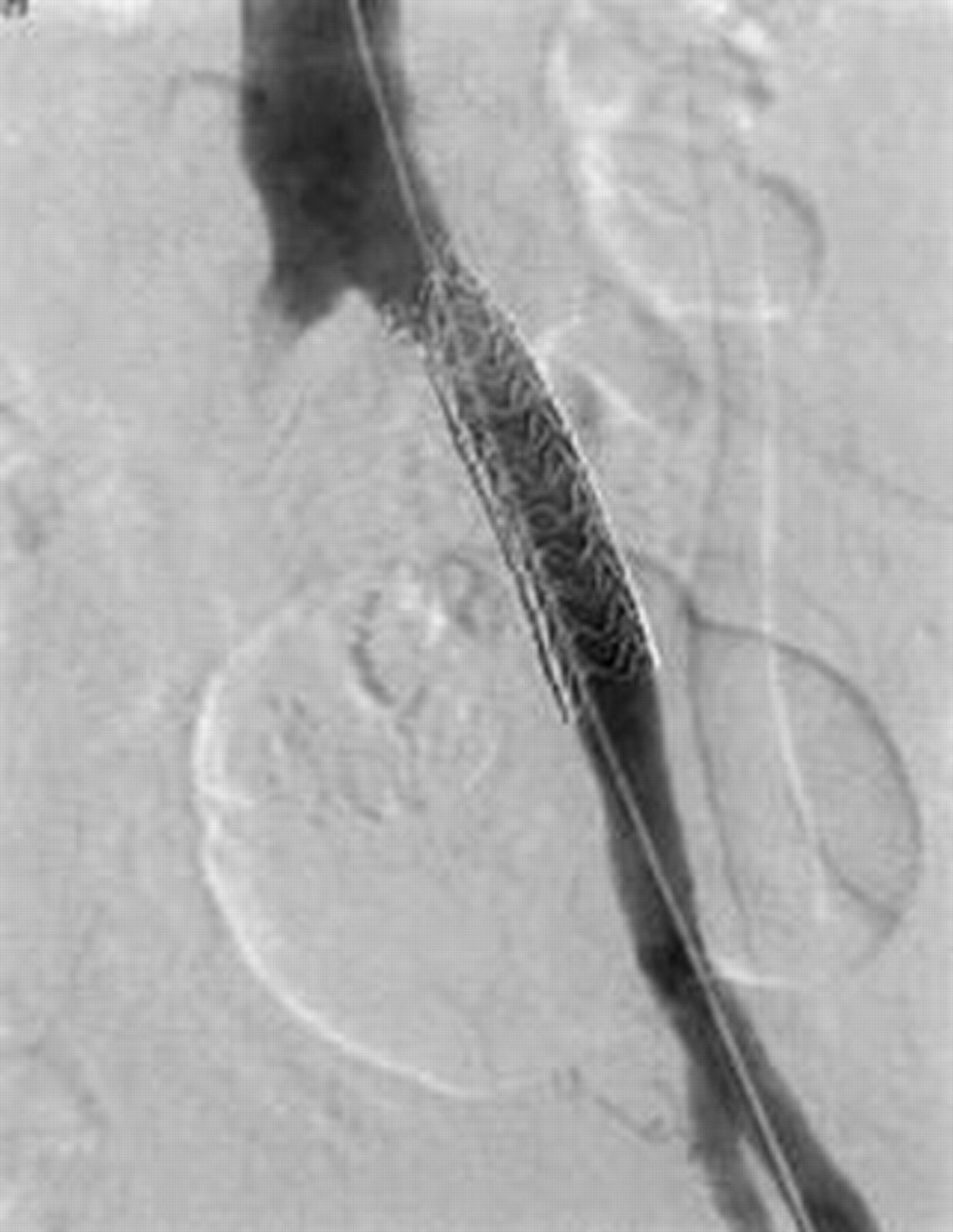
Completed angiogram after left common iliac artery stent placement. The stent has been successfully placed, eliminating both the residual stenosis after initial angioplasty and the persistent pressure gradient.
According to Ballard and colleagues, factors such as female sex, superficial femoral artery occlusion, perioperative vascular complications, and hypercholesterolemia proved to be risk factors for lower patency rates in iliac artery stents. 26 In their multivariate analysis, they failed to show that stent location in the CIA versus the external iliac artery (EIA) made a difference in patency rates.
Treiman and colleagues analyzed risk factors for early stent failure and found no independent variable in predicting success. 27 In their study, superficial femoral artery patency did not correlate with outcome, nor did anatomic location of the iliac artery stent.
Lee and colleagues found that anatomic patency rates for EIA and CIA stents appeared to be similar despite the fact that patients with EIA stents were older and had more ischemic limbs compared with the patients who had CIA stents. 28
The utility of selective provisional stenting to salvage iliac lesions after failed or unsatisfactory PTA owing to elastic recoil, flow-limiting dissection, or residual gradient is well established and incontrovertible. It was seen in a series of 250 patients undergoing either PTA alone or PTA with provisional stenting that the provisional stent arm was associated with more than a 2.5-fold reduction in immediate failures, although cumulative 4-year patency rates in the two groups were similar (primary, 58% and 64%; secondary, 68% and 74%; p value .005). 29 In a further meta-analysis study of iliac artery intervention, stent placement was found to reduce the risk of long-term failure by 39% when compared with PTA alone, and the 4-year success rate for iliac angioplasty was approximately 44 to 65%. 30 Another study comparing angioplasty alone with angioplasty with stenting showed that the 5-year primary patency rate had increased 24%, with a secondary patency rate more than 80% at 32 months, with reduction in long-term failure by 39% when stents were used. In this analysis, stenting improved the 4-year primary patency rates by approximately 10% for both patients treated for claudication and critical ischemia and patients treated for iliac stenoses and occlusions. 31 Despite the recent widespread use of iliac artery stenting, the approach of selective stenting appears to be as efficacious and more cost-effective. The correlation between unsatisfactory PTA more with multisegmental disease and long-segment iliac occlusions led to the recommendation of primary stent placement. 31–34 Other investigators suggested that complex multilevel iliac occlusive disease treated with stenting is prone to failure, particularly when there is involvement of the EIA. 14,33,35 In fact, failures from angioplasty alone in these cases may be overestimated and predominantly due to the inability to cross an occluded vessel that would not be salvageable with stenting.
Balloon-Expandable Stents
When using these stents for total iliac occlusions, one can expect early technical success in up to 97% of procedures, with 3-year primary and secondary patency rates of 70 and 80%, respectively. 36
Several randomized studies comparing endovascular stenting with stand-alone PTA showed stenting to be superior in both hemodynamic parameters and Rutherford classification. Time has demonstrated an increasing superiority of stents compared with balloon angioplasty. 20,21,23,26,27,37 In a greater than 4-year follow-up, only 67% of the PTA group showed clinical improvement (one or more Fountain class), whereas approximately 90% of the stent group improved. The Dutch Iliac Stent Trial Study Group performed a randomized comparison of primary stent placement with primary angioplasty followed by selective stent placement in patients with iliac artery occlusive disease. The investigators showed that selective stent placement, in which a stent is placed after iliac artery angioplasty when there is a pressure gradient of more than 10 mm Hg across the treated site, was equally as effective in maintaining iliac patency when compared with primary stent placement. They also showed that the selective stent placement is more cost-effective than primary stenting of iliac artery stenosis. 36,38 Yet nearly half (43%) of the patients randomized to balloon angioplasty necessitated stent placement for a suboptimal result during the primary procedure. Complication rates were nearly doubled (4% vs 7%) in the angioplasty group. Interpretation of these study results is difficult because of a mean follow-up of < 1 year and low acute technical success rates (approximately 80% for both groups). A later report with 5-year follow-up of this study did not find a significant difference between the groups, although repeat intervention was more common in the angioplasty group. 39 A meta-analysis of more than 1,300 patients comparing iliac angioplasty and stenting found significantly higher acute technical success, as well as improved primary patency in both claudicants and those with limb-threatening ischemia of > 90% and 2- and 5-year patency rates of > 70%. 5,30 In another study on 106 patients, kissing iliac stents showed good results in aortic bifurcation disease, which can be very problematic for balloon angioplasty, with primary and secondary patency rates of 78% and 98%, respectively, at 3 years. 40
Covered Stent Grafting
Self-expanding polyethylene terephthalate and polytetrafluoroethylene-covered stents have been shown to decrease the need for repeat procedures in the iliac artery. 41 Similar to surgical bypass, minimal luminal diameter will affect the patency of these stents.
A review of the current literature (1995 to the present) was also undertaken to evaluate the use of stents and long-term patency after endovascular treatment of aortoiliac disease. All articles were published between 1995 and 2006, and those with less than 20 patients were excluded. The results are summarized in Table 2.
Literature Review of Endovascularly Treated Iliac Occlusive Disease
BE = balloon expandable; CS = covered stent; NA = not available; SE = self-expanding; SS = Wallstent stainless steel; V = Viabahn.
Cost-Effectiveness
As previously discussed, more than 40% of balloon angioplasty procedures for focal disease will be associated with significant residual physiologically important stenosis. A primary stent philosophy offers many benefits, including improved technical success, the ability to treat complex disease, and lower radiation exposure and contrast use. In addition, complications from dissection, acute vessel closure, and distal embolization are significantly decreased, and long-term restenosis rates appear to be significantly improved. It appears as though the only reason not to use a stent is the associated upfront cost. Today, the stent market has expanded to the point where prices have significantly decreased and repeat procedural costs are much lower than before, virtually negating this argument. Furthermore, selective iliac stenting is extrapolated to be cost-effective. In the Dutch iliac stent trial, this approach prevented stent use in 57% of patients, without affecting outcomes. 39 An economic analysis of the treatment of iliac stenoses by Bosch and Hunink using meta-analytic and prospective trial data sets concluded that primary stenting has an incremental cost of almost $1,000 more at analysis 1 year after treatment (including the impact of reinterventions) compared with selective stenting. 30 Even if selective stenting is applied to more complex chronic occlusive disease, the 10 to 15% of cases that may avoid stenting yield a cost-effectiveness over a strategy of primary stent placement. 3 Considering a 12 to 30% 5-year cardiovascular mortality rate for patients with iliac disease and the recently proven durability of selective stenting out to more than 5 years, the late-term cost-effectiveness of a selective stenting approach is likely to be even further enhanced. 39
Complications
The main complication after endovascular intervention is embolic phenomena, which are estimated to be 4% but may be as high as 24% when treating longer-segment occlusions. 14,42 However, chronic total occlusions of the iliac artery comprise only 13% of lesions in a larger series of iliac interventions, and newer methods of clot removal prior to angioplasty may theoretically lower embolic risks. 43
Conclusion
Percutaneous revascularization of the CIA and EIA using PTA with or without stents is a well-established, minimally invasive technique and has supplanted aortofemoral bypass for the majority of patients who have symptomatic iliac atherosclerosis. Decisions regarding the appropriateness of stenting for a patient with iliac atherosclerosis knowingly need to be individualized. Existing data suggest that angioplasty alone or with strictly defined provisional stenting is expected to have similar initial results and long-term durability compared with primary stenting in most scenarios, which may, in fact, be a cost-effective strategy. The primary use of stents for occlusions exceeding 5 cm in length may be justified to reduce procedural complications. However, long-segment chronic occlusions comprise a minority of treated iliac lesions. In these cases, the major determinant of successful therapy is an ability to traverse the obstruction rather than the mode of therapy. The impact of evolving technologies, including cryoplasty, drug-elution platforms, and stent grafts, will undoubtedly continue to fuel future controversies regarding the optimal management of iliac disease.