
Abstract
We evaluated the incidence, risk factors, and clinical consequences of renal microembolic events following endovascular aneurysm repair using suprarenal or infrarenal fixation. Pre- and postoperative (1 month) computed tomographic angiograms were reviewed for new renal perfusion defects. Suprarenal aortic and infrarenal neck thrombus load was classified by circumference involved and thrombus thickness. Serum creatinine was measured preoperatively, on the first postoperative day, and 1 month postoperatively. Among 136 patients, 8 (5.9%) had bilateral microembolic cortical defects. Patients with moderate or severe suprarenal thrombus were more likely to have renal microemboli than those with no or mild suprarenal thrombus (17% vs 0%; p < .001). Similarly, patients with moderate or severe infrarenal neck thrombus were more likely to have renal microemboli than those with no or mild infrarenal thrombus (9.6% vs 1.5%; p = .08). Severe infrarenal thrombus was independently predictive of microembolization (odds ratio 15.0; 95% confidence interval 1.6–142; p = .018). There was no statistically significant difference in the incidence of renal microembolization when comparing suprarenal and infrarenal fixation (8.2% vs 4.0%; p = .47). Changes in creatinine from baseline were not different in those with or without renal microemboli. Renal microembolization is an uncommon but distinct radiographic finding that is more associated with significant neck thrombus than fixation level.
Endovascular aneurysm repair (EVAR) has emerged as an acceptable alternative to the open surgical repair of abdominal aortic aneurysms (AAAs). Recently completed randomized controlled trials documented the lower perioperative morbidity and mortality of EVAR compared with open repair. 1,2 Candidacy for EVAR remains dependent on the presence of an adequate length and diameter of infrarenal aorta for proximal sealing, absence of severe neck angulation, and appropriate iliac anatomy to facilitate stent graft delivery and distal sealing.
Despite the significant early advantages when compared with open repair, EVAR is not without associated risks. These include device failure, endoleak, stent graft limb thrombosis, aortoiliac vascular injury, contrast nephropathy, and distal thromboembolization. Thromboembolic events after EVAR may result in mesenteric, renal, or lower extremity ischemia. These have been attributed to wire-, catheter-, and device-related manipulations within a thrombus-lined descending aorta or the AAA itself. The kidneys may be especially vulnerable to such events as the suprarenal and infrarenal aorta represent sites of stent graft fixation and/or proximal sealing, depending on the type of device chosen. Major segmental renal infarctions, usually unilateral, have been described following EVAR, often attributed to macroemboli or coverage of accessory renal arteries. 3–5 However, diffuse bilateral renal microembolic events, often predominantly involving the renal cortex, have not been described and represent a unique radiographic and clinical entity (Figure 1). In this study, we evaluated the incidence, risk factors, and clinical consequences of diffuse bilateral renal microembolic events following EVAR using both suprarenal and infrarenal fixation.

Bilateral renal microemboli (arrows) noted on computed tomographic angiography 1 month following endovascular aneurysm repair.
Methods
Medical records and imaging studies for consecutive patients undergoing EVAR from February 2003 through July 2004 were reviewed. Preoperative helical computed tomographic (CT) angiography was performed to assess AAA morphology and candidacy for EVAR. Specifically, AAA diameter, infrarenal neck length and diameter, and the presence of accessory renal arteries were noted. Suprarenal aortic and infrarenal neck thrombus load (Figure 2) was classified by the circumference of the involved segment and thickness of the thrombus: none, mild (< 25% circumference and < 5 mm thick), moderate (25–50% and < 10 mm), and severe (> 50% or > 10 mm). The suprarenal aorta was defined as that segment between the celiac trunk and the renal artery level. The infrarenal neck was defined as the nonaneurysmal aortic segment extending 15 mm distal to the lowest main renal artery.
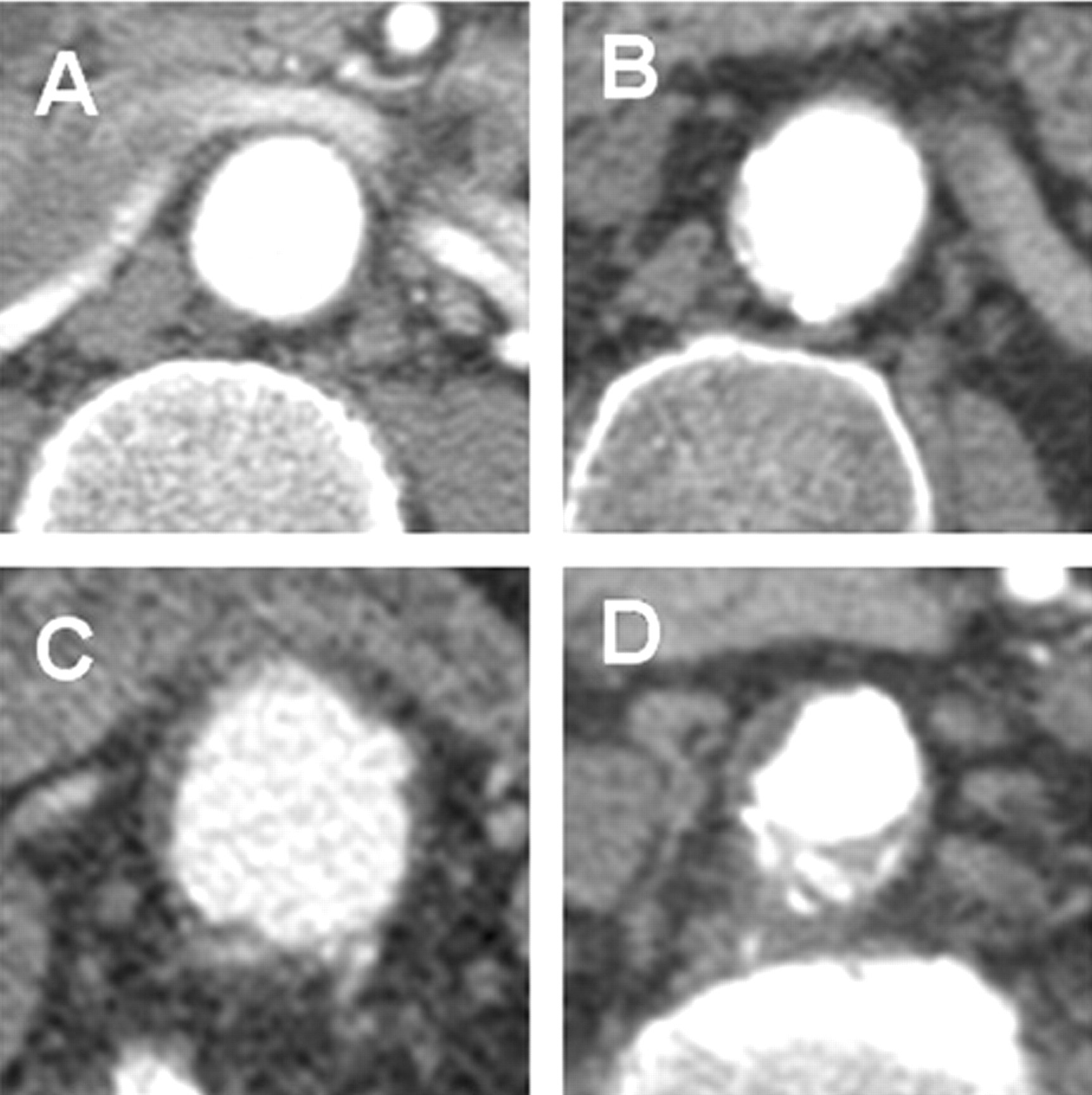
Increasing amounts of thrombus lining the infrarenal aneurysm neck. A, None; B, mild (< 25% circumference and < 5 mm thick); C, moderate (25–50% and < 10 mm); D, severe (> 50% or > 10 mm).
A wide variety of stent grafts employing both suprarenal and infrarenal fixation techniques were used during EVAR. Intentional coverage of accessory renal arteries or simultaneous stenting of renal artery stenoses was noted, as were any other intraoperative renal events. Per our protocol, helical CT angiography was performed postoperatively at 1 month. Both pre- and postoperative CT scans were reviewed for the presence of new renal perfusion defects, with confirmation of all findings by a radiologist.
Serum creatinine concentrations were reviewed to assess renal function and were measured preoperatively, on the first postoperative day, and at the 1-month postoperative visit. Changes in serum creatinine were assessed by comparing preoperative and postoperative levels for each patient. When examining those with and without renal microemboli, mean changes in creatinine were compared using Student's t-tests. To identify predictors of renal microembolization, categorical variables were analyzed using chi-square and multivariate logistic regression as appropriate. Continuous variables were analyzed using Student's t-test or paired t-test. The Cochran-Mantel-Haenszel test-for-trend was used to analyze relationships between thrombus severity and renal microembolization. A p value of ≤ .05 was considered significant. The study was approved by the University of Pittsburgh Institutional Review Board.
Results
From February 2003 through July 2004, 153 patients underwent EVAR. Of these, 136 patients (110 men; mean age 76 ± 7 years) with documented pre- and postoperative CT angiograms were identified. Although all 136 patients had preoperative assessment of AAA diameter, neck dimensions, and renovascular anatomy noted within our medical records, the preoperative CT angiograms of 18 of 136 patients obtained at other institutions were not available for direct measurements of pararenal thrombus load at the time of this study.
AAA and neck morphology are summarized in Table 1. The mean AAA diameter was 55 ± 10 mm, whereas the mean infrarenal neck diameter and length were 25 ± 3 mm and 22 ± 9 mm, respectively. Accessory renal arteries were present in 11% of cases. Moderate or severe thrombus was noted in the suprarenal aorta in nearly a third and the infrarenal aorta in nearly half of all patients.
Abdominal Aortic Aneurysm Pararenal Thrombus Load (n = 118)
With respect to operative technique (Table 2), suprarenal fixation was used in 61 patients (45%), with infrarenal fixation in 75 patients (55%), employing a wide variety of stent grafts. There was no difference in preoperative thrombus distribution when those with suprarenal and infrarenal grafts were compared. Accessory renal arteries were intentionally covered in 7 cases (5%), and simultaneous renal artery stenting for stenoses was performed in 5 cases (4%).
Operative Characteristics of Endovascular Aneurysm Repair (n = 136)
There were 20 (14.7%) new renal perfusion defects identified on postoperative CT angiography. Twelve (8.8%) patients had segmental renal infarcts, half of which were associated with intentional coverage of accessory renal arteries or concomitant renal stenting. The remaining 8 (5.9%) patients had evidence of diffuse bilateral microembolic cortical defects.
By univariate analysis, there were no differences in AAA diameter, neck dimensions, or the incidence of accessory renal arteries in patients with and without renal microembolization. There was no statistically significant difference in the incidence of renal microembolization when comparing suprarenal and infrarenal fixation (8.2% vs 4.0%; p = .47). There was also no difference in the distribution of supra- or infrarenal thrombus between the fixation groups. Patients with moderate or severe suprarenal thrombus were more likely to have renal microemboli than those with no or only mild suprarenal thrombus (17% vs 0%; p < .001; Table 3). Similarly, there was a trend toward more frequent renal microembolization among patients with moderate or severe infrarenal neck thrombus when compared with those with no or mild infrarenal thrombus, although this did not reach statistical significance (9.6% vs 1.5%; p = .08). When also analyzed using the Cochran-Mantel-Haenszel test-for-trend, there was a direct relationship between increasing suprarenal (p = .001) and infrarenal (p = .02) thrombus severity and the incidence of diffuse renal microembolization (see Table 3). When both suprarenal thrombus severity and infrarenal thrombus severity were included in a multivariate analysis, severe infrarenal thrombus was identified as an independent predictor of microembolic events (17% vs 1.1%; odds ratio 15.0; 95% confidence interval 1.6–142; p = .018).
Pararenal Thrombus Load and Renal Microembolization
*Cochran-Manel-Haenszel test for trend.
Serum creatinine levels were available both preoperatively and on the first postoperative day in 108 patients. Patients without renal microemboli (n = 100) had a statistically significant decrease in serum creatinine on the first postoperative day (1.13 vs 1.07 mg/dL; p = .001), with a mean decrease in serum creatinine of 0.06 mg/dL. Those with microemboli (n = 8) had no significant change in serum creatinine on the first postoperative day (1.22 vs 1.26 mg/dL; p = .63). Changes in serum creatinine were not significantly different (p = .13) between groups (with or without microemboli).
At 1 month following EVAR, 56 patients had serum creatinine levels available. Those without microemboli (n = 52) had no significant change in serum creatinine (1.13 vs 1.15 mg/dL; p = .46). Similarly, patients with renal microemboli (n = 4) experienced no significant change in serum creatinine within the first postoperative month (1.35 vs 1.50; p = .41). The difference between groups (+0.02 vs +0.15 mg/dL) was again not statistically different with the small number of patients available for review (p = .29).
Discussion
Over the past decade, endovascular repair of AAAs has become a viable alternative to open repair, especially in patients considered medically high risk. Recent prospective randomized trials have concluded that EVAR may be associated with lower periprocedural morbidity and mortality compared with open repair and at least similar midterm outcomes. 1,2,6,7 Much of this may be attributed to improved patient selection, increasing surgeon experience, and dramatic advances in device development, including the introduction of devices with suprarenal fixation. Associated with the significant increase in EVAR volume, complications unique to or more frequent following EVAR have come to the forefront, especially when selection criteria are relaxed following commercial release of devices.
Although clinically significant thromboembolic complications are rare events following EVAR (< 1%), radiographic evidence of thromboemboli is present in approximately 10% of cases and can affect any visceral vascular territory. 8 The kidneys are particularly susceptible, given their proximity to the most diseased aortic segments during device deployment. Although several authors have described segmental renal infarctions complicating EVAR, 3–5,8 few have differentiated this pattern from that of diffuse bilateral cortical microembolization, identified in nearly 6% of the patients in this series. Contributing to this may be the generally asymptomatic nature of this phenomenon, in addition to its subtle radiographic presentation, which is often overlooked on initial review of postoperative CT angiograms.
In this study, we found that those patients with moderate or severe suprarenal or infrarenal aortic luminal thrombus were at increased risk of renal microembolization and that this risk was directly related to thrombus severity. Specifically, severe infrarenal thrombus was an independent predictor of microembolization on multivariate analysis. This concurs with other reports correlating thrombus load with renal thromboembolic complications. Harris and colleagues used volumetric analysis of infrarenal neck thrombus load and found a significant increase in the risk of postoperative renal perfusion defects (45% vs 10%) when the percentage of neck atheroma volume exceeded 40%. 3
In terms of the mechanism, microembolization is likely directly related to manipulations of catheters, wires, balloons, and other devices that disturb the laminated pararenal aortic thrombus and/or friable atheromata most significantly during device deployment. Despite this simplistic explanation, why certain patients develop segmental infarcts whereas others have strictly cortical microemboli remains unclear. The outcome may depend on unique local anatomic factors, such as the presence of loosely attached thrombus or ulcerogenic plaque. Interestingly, no patients in the microembolization group had any other peripheral stigmata of emboli (eg, in the lower extremities) noted postoperatively. One might speculate that at the time of stent graft deployment, some pararenal thrombus may be expelled into the renal arteries, showering the renal parenchyma. This leaves the remaining thrombus trapped by the body of the stent graft and not free enough to embolize distally in the lower extremities. Alternatively, subtle lower extremity microembolization may have been unnoticed or undocumented if clinically insignificant, highlighting the limitations of this retrospective review.
Although this study represents the first to identify suprarenal thrombus as a second possible risk factor, multivariate analysis failed to verify an independent relationship between suprarenal thrombus severity and renal microembolization. This likely reflects the small numbers of patients with microembolization, as well as the frequent coexistence of severe infrarenal thrombus in patients with severe suprarenal atheromatous disease. Nevertheless, it is likely that suprarenal thrombus load does contribute to renal thromboembolic phenomena, albeit to a lesser degree, given the manipulations within the suprarenal aorta necessary for precise stent graft deployment.
Suprarenal devices may be expected to generate more embolizations when pararenal thrombus is noted. Although the rate of microemboli was twice as high compared with that for the infrarenal devices, the small numbers may have prevented us from detecting any significant association with the type of device. Similarly, Krämer and colleagues found no difference between suprarenal and infrarenal fixation in the incidence of renal thromboembolic events, emphasizing that most perfusion deficits were “punctate” and likely related to intraortic instrument manipulation. 4 Interestingly, in our study, no patients with moderate or severe suprarenal thrombus experienced renal microembolization following suprarenal stent graft implantation. The reasons for this are not completely clear. Although this may represent a type II error related to small sample size, it may also reflect local differences in plaque or thrombus stability at these two levels, leaving the infrarenal aorta more vulnerable to plaque or thrombus dislodgment.
When renal function was examined in the immediate postoperative setting, those patients with microemboli did not experience the same significant drop in serum creatinine observed in those without microemboli. Although the observed drop in creatinine within this group is likely related to a “dilutional” effect, the absence of a similar drop in the microemboli group suggests a possible early, albeit minor, reduction in renal function. Other factors, such as the amount of contrast administered and operative blood loss, may also have influenced this finding, although this information was not consistently available within the medical record. The short- and midterm effects of microembolization are certainly difficult to assess, given the absence of enough patients with available serum creatinine levels beyond the initial hospital stay. Clearly, this study is underpowered with respect to the effects of microembolization on renal function. Furthermore, the use of serum creatinine levels as a marker for renal function has been criticized, in favor of the normalized, calculated creatinine clearance derived from the Cockgroft formula. Unfortunately, preoperative patient weights were not uniformly available for the small group of patients with microembolization.
This retrospective study is subject to several other significant limitations. First, renal microembolization represents a radiographic phenomenon, and the long-term clinically relevant effects on renal function remain unknown as serum creatinine levels or glomerular filtration rates were not uniformly available for all patients and only short-term data could be accrued. Despite this, others have documented the stable renal function and lack of symptoms noted in the vast majority of patients with renal thromboembolic events immediately post-EVAR, whether infarctions or cortical microemboli. 4 This reflects the significant renal functional reserve available in those with relatively normal renal function. Patients with chronic renal insufficiency therefore may be especially vulnerable to the effects of renal microembolization and may benefit the most from the development of renal “embolic protection devices” currently used in some centers during renal stenting. 9
Second, since all renal perfusion deficits in this study were noted on the 1-month CT angiogram post-EVAR, the true incidence of renal microembolization is not known. That is, although some patients go on to develop cortical thinning or scarring, some patients may resolve these deficits rapidly without noticeable abnormalities on follow-up CT angiography, suggesting that the true incidence may be significantly higher than the 5.9% reported in this study. Finally, the small sample size may limit our ability to document real differences among the subgroups and draw significant conclusions, especially with the relatively low incidence of renal microembolization.
In conclusion, renal microembolization is an uncommon but distinct radiographic finding that is associated more with significant neck thrombus than with fixation level. Patients with moderate to severe aortic thrombus, especially in the infrarenal position, should be approached with caution, especially in the setting of preexisting chronic renal insufficiency or impaired renal reserve. Long-term follow-up will be necessary to determine the chronic clinically significant effects of renal microembolization.
Footnotes
Presented in part at the 2005 annual meeting of the Midwestern Vascular Surgery Society, Chicago, IL.