
Abstract
Behçet's syndrome is a multisystemic disease characterized by relapsing uveitis, oral and genital ulcerations, and vascular system involvement. The vascular involvement is seen as venous occlusion, arterial occlusion, and aneurysm formation in this disease, and the surgical treatment of a Behçet's aneurysm has technical difficulties. In this report, we suggest that the huge popliteal artery aneurysm in Behçet's syndrome can be treated by ligation of the popliteal artery.
A 58-year-old male patient was admitted to our clinic because of an infrapopliteal great mass at the left leg. Color Doppler ultrasonography and arteriography revealed a 71 × 54 mm aneurysmal dilatation at the distal popliteal artery. Surgery did not reveal any suitable arterial formation for bypass to the distal area of the popliteal artery and tibial arteries. For this reason, we applied ligation of aneurysmal dilatation at the distal popliteal artery. The patient tolerated the operation well and had no signs of ischemia during the postoperative period.
In conclusion, especially in aneurysm of arteries such as the popliteal artery, which has critical importance for maintaining distal perfusion, ligation may be a treatment method if there are no other alternatives.
Behçet's syndrome, first defined by Hulusi Behçet in 1937, 1,2 is a multisystemic disease characterized by relapsing uveitis, oral and genital ulcerations, and vascular system involvement. The disease is common in Mediterranean countries and Asia. The etiology remains unknown, but it is supposed that autoimmunity triggered by bacterial or viral infection or other environmental factors plays a role. The frequency of arterial disease varies between 15 and 32% in patients with Behçet's syndrome. Vascular involvement is seen as venous occlusion, arterial occlusion, and aneurysm formation in this disease. Behçet's aneurysms, which tend to be multiple, could involve the whole arterial tree. The artery most often affected is the aorta, followed by the pulmonary and femoral arteries. 1,2
Histologic examination of involved specimens reveals a panvasculitis with edematous changes of the endothelial cells. The underlying medial layer is disrupted owing to disorganization of the elastic components of the vessel wall. Inflammatory cells invade the outer layers of the artery and infiltrate the perivascular tissue. 2
Surgical treatment of a Behçet's aneurysm has technical difficulties because the aneurysm usually adheres tightly to concomitant veins, nerves, and the perivascular tissues. In this report, we suggest that popliteal artery aneurysm in Behçet's syndrome can be treated by ligation of the popliteal artery.
Case Report
A 58-year-old male patient was admitted to our clinic because of an infrapopliteal great mass at the left leg, pain, sensitivity, and difficulty in walking. On physical examination, we found a large pulsatile and painful mass at the left infrapopliteal region. Color Doppler ultrasonography revealed a 71 × 54 mm aneurysmal dilatation at the left distal popliteal artery (Figure 1). According to the patient's record, he had undergone surgery for a right radial and left ulnar arterial aneurysm owing to Behçet's syndrome 2 years previously. After neurologic, ophthalmologic, dermatologic, and rheumatologic consultation, the diagnosis was Behçet's syndrome, according to the criteria of the International Study Group for Behçet's Disease. A family history of Behçet's syndrome was not noted. No pathologic findings were observed in electrocardiography, chest radiography, chest and abdominal computed tomography, and abdominal ultrasonography. The erythrocyte sedimentation rate was elevated at 72 mm/h, C-reactive protein was 54 mg/dL, and serum electrolytes, blood urea nitrogen, creatinine, glucose, cholesterol, and blood cell counts were normal. Angiography revealed aneurysms at the left distal popliteal artery and ectasia of the proximal peroneal artery. Distal arterial trees and collaterals of the left leg were not visualized (Figure 2). Ankle-brachial indices were not performed in the preoperative period.
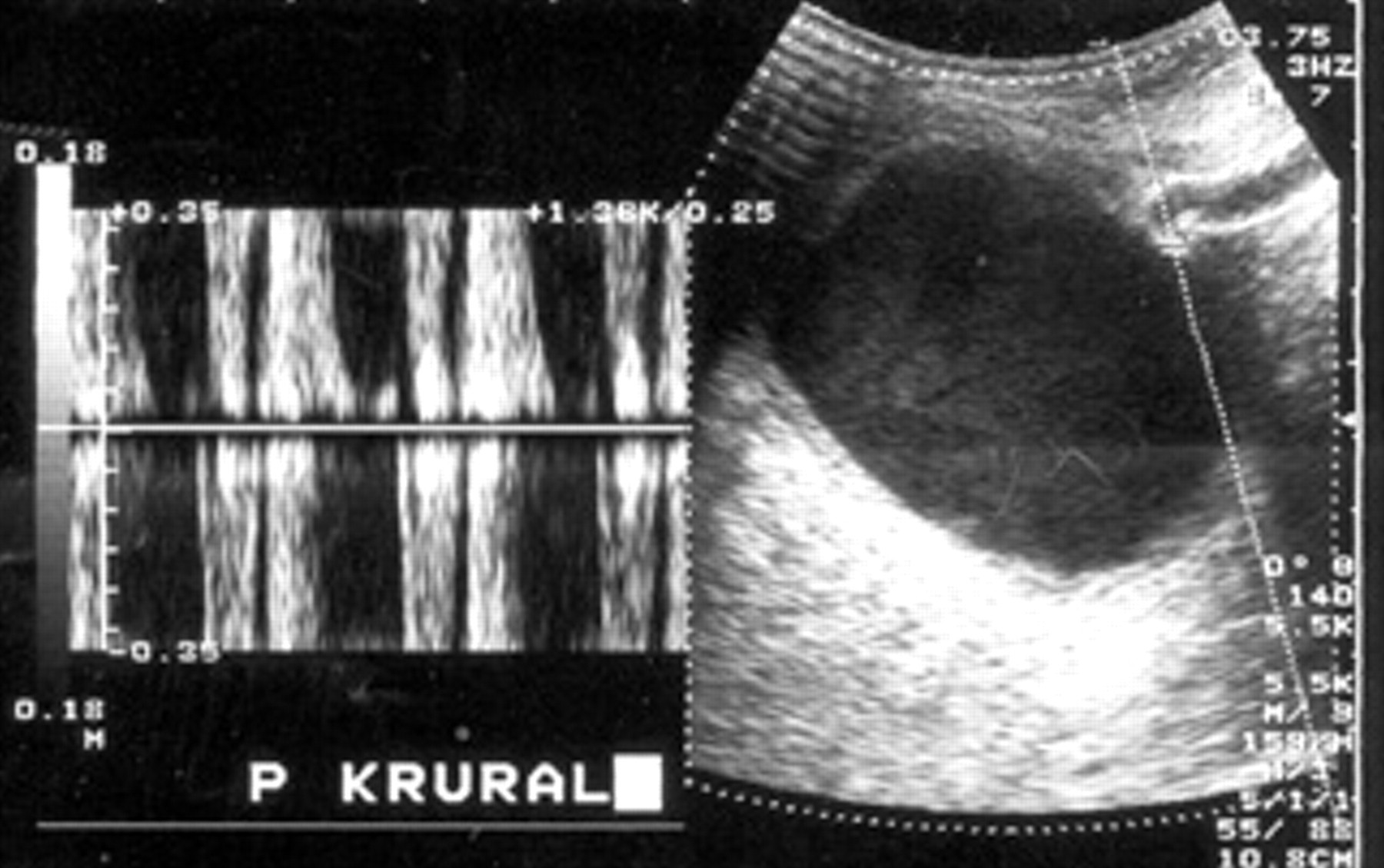
Color Doppler ultrasonography revealed a 71 × 54 mm aneurysmal dilatation at the left distal popliteal artery.

Angiography revealed aneurysms at the left distal popliteal artery and ectasia of the proximal peroneal artery.
Because of the possibility of rupture and excessive pain, the patient underwent surgical repair. We planned a by-pass operation between distal superficial femoral artery and tibial arteries together with aneurysmal ligation. A medial approach was used. We could not find any suitable arterial formation for bypass to the distal area of popliteal artery and tibial arteries at operation. The aneurysmal sac was not tightly adhered to surrounding tissue. All of the tibial arteries were found to be very fibrotic and their lumens were occluded. For this reason, we applied ligation to the distal and proximal edges of aneurysmal dilatation at the distal popliteal artery. Because the intra-aneurysmal pressure did not decrease and pulsation continued, the aneurysmal wall opened. Three vascular orifices were found that had good backflow in the aneurysmal sac, and all of them were ligated. We thought that the patient would tolerate the ligation in light of these two findings. These branches were not felt to represent important collaterals. We did not find these small branches important, which is why a bypass was not done. The patient tolerated the operation well and had no signs of ischemia or postoperative complications. Claudication or rest pain did not develop postoperatively. The patient had no problems during the 3-month follow-up period.
Discussion
Popliteal artery aneurysms are defined as localized dilatations of the popliteal artery 2 cm in diameter or 150% of the normal arterial caliber. Popliteal artery aneurysms are mostly atherosclerotic in origin. Other rare causes include mycotic aneurysms or those associated with Marfan or Behçet's syndrome. Popliteal artery aneurysm disease appears to be relatively uncommon in the general population, with an estimated incidence of less than 0.1%. 3 The original treatment of atherosclerotic popliteal aneurysms was proposed by Dr. Rudolph Matas at the turn of the century. He performed popliteal arterial ligation and opened the aneurysm to oversew branches in the body of the aneurysm.
Aneurysm formation in the arterial system can be seen in Behçet's syndrome. The most common location for the formation of the aneurysm is the abdominal aorta. The ratio of the popliteal artery aneurysm is not known. Patients with Behçet's syndrome are at increased risk of synchronous and metachronous arterial aneurysms, both peripheral and aortic. 1 This reported patient had aneurysms at the left distal popliteal artery and ectasia of the proximal peroneal artery. In spite of this, there was no large vessel pathology. The prognosis seriously depends on thrombotic obstruction of distal vessels in Behçet's syndrome patients who have an aneurysmal artery. In these patients, thrombus formation and distal embolism may cause loss of the extremities. Our patient's distal vessels were occluded from chronic microembolisms and consisted of fibrosis. For this reason, we could not perform a bypass operation to provide distal perfusion. The other risk in these cases is the need for an emergency operation because of aneurysmal rupture. Mortality and the loss of the extremities are high in such cases.
In the reported case, the aneurysmal diameter was increased and had high levels of rupture risk. For this reason, the aneurysm was ligated from the distal and proximal edges. Because the rich collateral circulation developed due to the chronic distal occlusions, the pressure in the aneurysmal sac did not decrease. So we opened the aneurysmal sac and closed the collateral vessel orifices, and the aneurysmal sac was capitoned. Frequently, ligation of the popliteal artery causes loss of the extremity. However, as seen in our presented case ligation of the popliteal artery without bypass may not cause problems in chronically occluded states, especially after collateral development in the popliteal area. Perhaps this is a special clinical state in Behçet's syndrome. Tuzun and colleagues introduced ligation as a means of surgical treatment for extremity aneurysms because the likelihood of finding an intact artery is low in Behçet's syndrome patients. 4 They reported eight cases of extremity aneurysms: one carotid, one subclavian, four superficial femoral, one popliteal, and one posterior tibial artery aneurysm treated with ligation after confirming an adequate stump pressure.
Recurrent aneurysm frequently occurs in Behçet's syndrome patients. During the postoperative period, these patients must be followed up frequently. To report case, the patient operated from each two upper extremities in consequence of aneurysmal formation 2 years ago. 4
In Behçet's syndrome, the timing of the operation is exclusive; generally the operation during active period is not advised. Most authors suggest medical treatment in the active period of disease before surgery. 4,5 But we operated on our patient in the active period because of the seriousness of his symptoms and the risk of aneurysmal rupture. Afterward, the patient was referred to the rheumatology clinic for the purpose of medical treatment and follow-up.
For popliteal artery aneurysms, endovascular treatment is also an alternative. 6 But we could not apply this treatment because of the lack of sufficient technical equipment in our hospital. However, for the case described, endovascular repair would be a poor choice. First, the patient would have had a large type 2 endoleak, probably requiring opening of the sac, with ligation of the vessels. Second, if there was no outflow, this endovascular bypass would not have any benefit. In addition, the success of this treatment is a subject for discussion in cases that had distal artery occlusion and high collateral circulation in the aneurysmal sac, as in our case. The patient's ectasia of the proximal peroneal artery was asymptomatic, and its diameter was small, which is why we did not intervene. For planning the timing of the procedure for this aneurysm, we suggested medical treatment of Behçet's syndrome with control of the patient at 3-month intervals. In conclusion, serious difficulties may occur in surgical treatment of vascular involvement in Behçet's syndrome.
We believe that, especially with regard to aneurysms of arteries such as the popliteal artery, which has critical importance for maintaining distal perfusion, ligation may be a treatment method if there are no other alternatives.